
Abstract
Keywords
Coronary artery calcium (CAC) score, derived from cardiac computed tomography (CT) scans, enhances the risk of cardiovascular disease (CVD) assessment by quantifying plaque burden and predicting future cardiovascular events. 1 Despite extensive research on the predictive power of CAC for coronary heart disease (CHD) and overall mortality, its relationship with stroke, including stroke-related mortality, is understudied. Therefore, our study aimed to evaluate the ability of CAC to predict stroke mortality independent of established traditional cardiovascular risk factors.
We included 63,630 participants referred for CAC scans without baseline stroke or CHD from the prospective, multicenter CAC Consortium study (mean age: 53.4 ± 10.3 years; women: 33.1%; CAC present: 54.1%; CAC absent: 45.9%). 2 Cardiac-gated CT scans were performed at baseline to assess CAC, categorized as absent/present, 0, 1–99, 100–299, or ⩾ 300. Mortality status was determined from the Social Security Index Death Master File and the causes of death were categorized using the International Classification of Diseases (9th and 10th revisions). 2 Participants provided consent at participation sites, with institutional review board approval from Johns Hopkins University School of Medicine for coordinating center activities and death ascertainment. 2 Patients with concurrent myocardial infarction at the time of stroke death were excluded from the analysis. We utilized Cox proportional hazards models to examine the relationship between CAC and stroke mortality, adjusting for traditional risk factors. To evaluate the predictive power of CAC in clinically relevant patient populations, we conducted subgroup analyses excluding those with baseline hypertension, diabetes, or both.
Over a mean follow-up period of 12.3 ± 3.9 years, there were 152 stroke deaths. Individuals with CAC > 0 had a higher incidence of stroke mortality than individuals with CAC = 0 (0.30 vs 0.06 per 1000 person-years) (χ2 = 63.03; p ⩽ 0.001). Compared with CAC = 0, individuals with CAC had a significantly higher risk for stroke mortality (aHR [adjusted hazard ratio], 1.79; 95% CI: 1.11–2.88). Stroke mortality risk increased significantly with higher CAC scores, albeit findings for CAC = 1–99 were not significant (aHR range: 1.36; 95% CI: 0.79–2.34 to 2.38; 95% CI: 1.41–4.01). Among individuals without baseline diabetes and hypertension, higher CAC values of ⩾ 300 were significantly associated with increased stroke mortality risk (aHR, 2.16; 95% CI: 1.00–4.70). Similar findings were observed among individuals free of hypertension (CAC ⩾ 300: aHR, 2.41; 95% CI: 1.14–5.11) (Table 1).
Stroke mortality risk by coronary artery calcium (CAC) score.
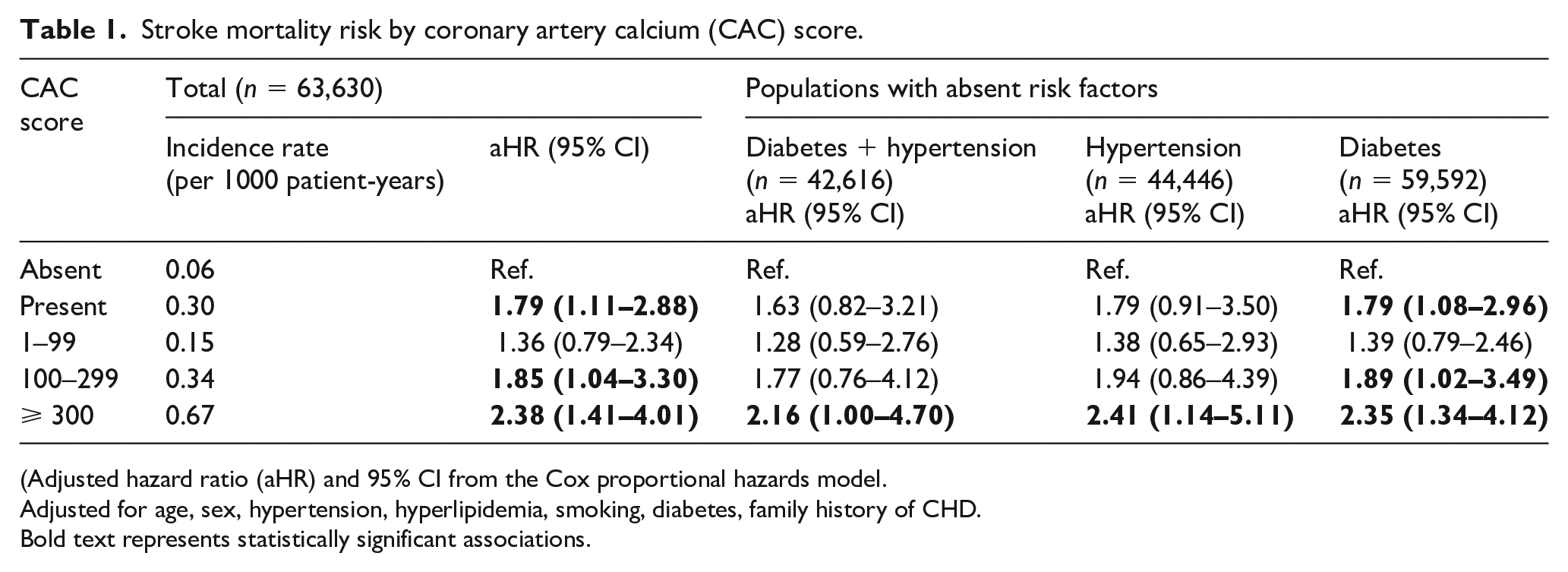
(Adjusted hazard ratio (aHR) and 95% CI from the Cox proportional hazards model.
Adjusted for age, sex, hypertension, hyperlipidemia, smoking, diabetes, family history of CHD.
Bold text represents statistically significant associations.
Our findings indicate that CAC is independently associated with stroke mortality among individuals free of stroke or CHD at baseline and remained associated with individuals free of diabetes, hypertension, or both. Importantly, our large-scale study is the first to link CAC and stroke mortality, distinct from other studies that primarily examined nonfatal stroke cases. 3
The limitations of our clinical study include a sample of predominantly White individuals and limited female representation, which may affect generalizability. Additionally, the lack of differentiation of stroke mechanisms due to limited information in death certificates, along with insufficient data on disease severity (e.g., blood pressure control, renal function) and nonfatal stroke events, as well as a lack of data on atrial fibrillation or medication use, are further limitations. However, our findings should accurately reflect the population typically undergoing CAC scans in routine clinical practice, as our sample was restricted to those obtaining clinical CAC scan referrals.
Our findings suggest that CAC may serve as an independent risk marker for all atherosclerotic disease-related mortality, extending beyond its primary role in predicting CHD and CHD-related mortality. The study also indicates the potential of CAC in enhancing risk stratification, particularly in the context of stroke mortality.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.