
Abstract
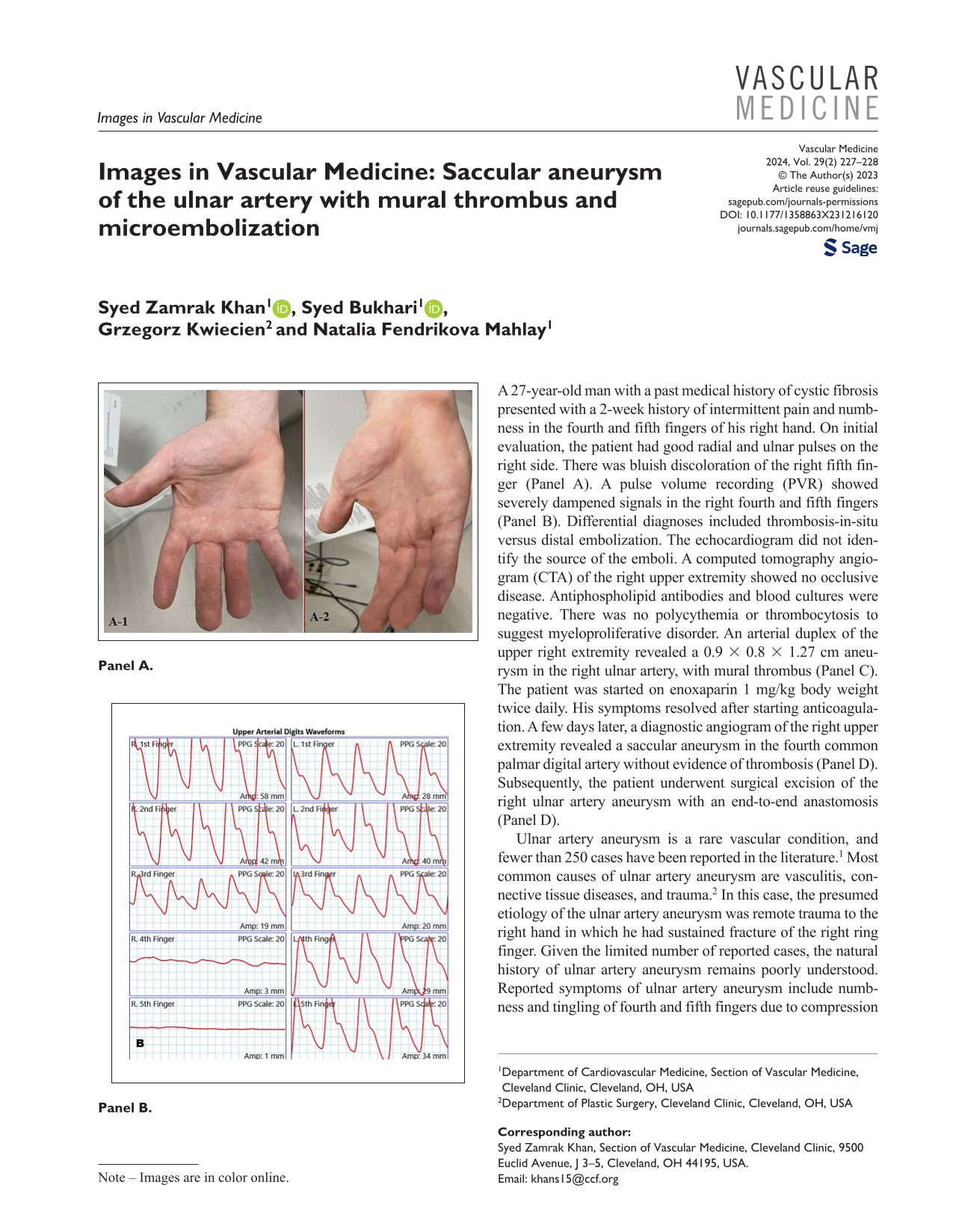
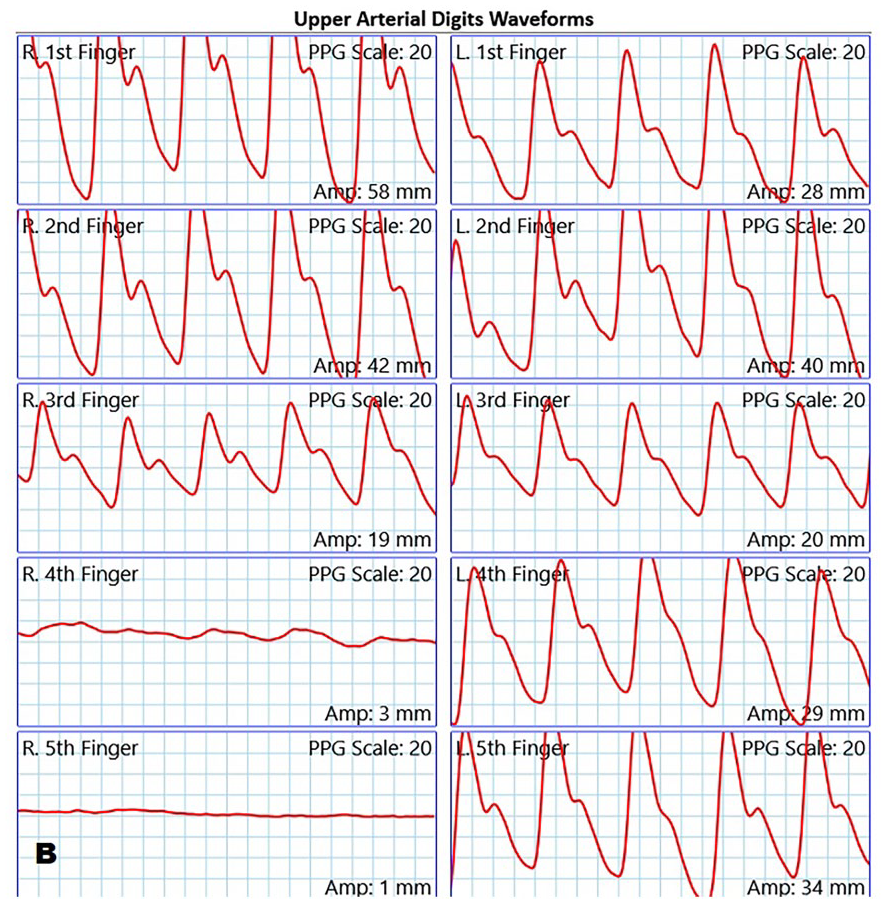
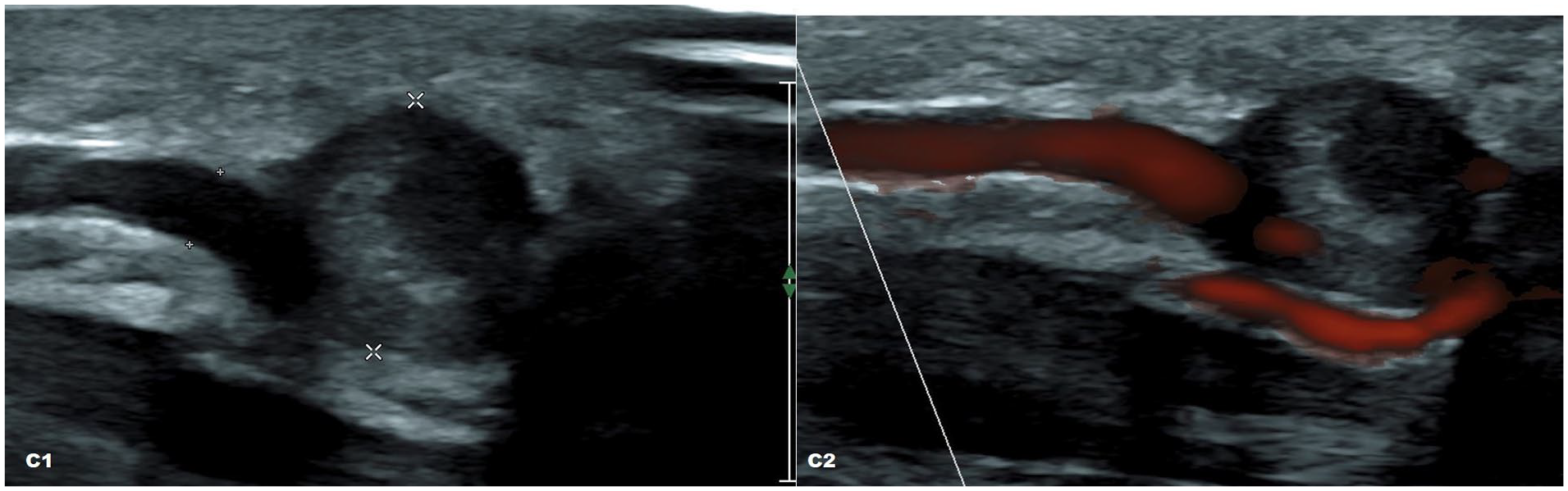
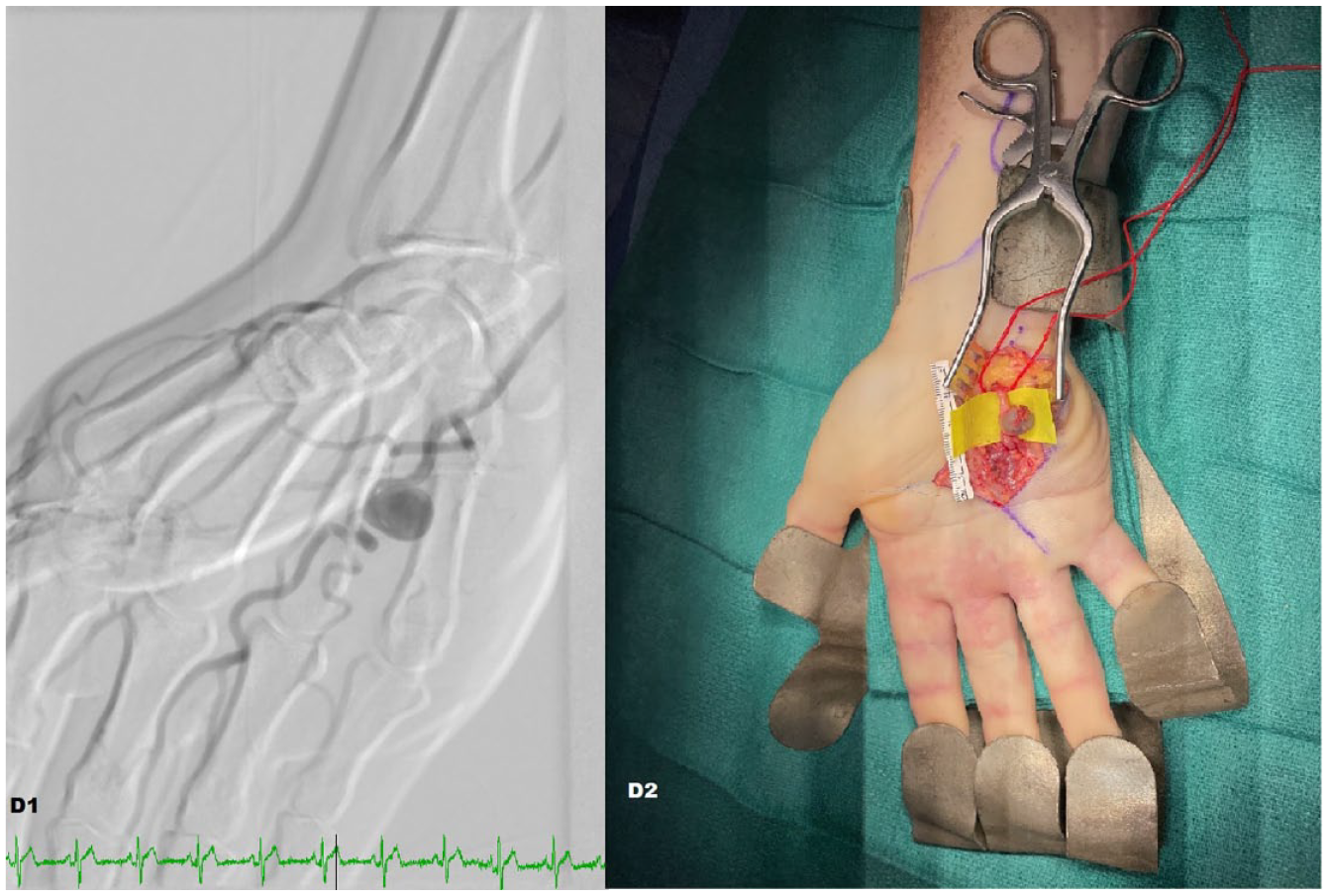
A 27-year-old man with a past medical history of cystic fibrosis presented with a 2-week history of intermittent pain and numbness in the fourth and fifth fingers of his right hand. On initial evaluation, the patient had good radial and ulnar pulses on the right side. There was bluish discoloration of the right fifth finger (Panel A). A pulse volume recording (PVR) showed severely dampened signals in the right fourth and fifth fingers (Panel B). Differential diagnoses included thrombosis-in-situ versus distal embolization. The echocardiogram did not identify the source of the emboli. A computed tomography angiogram (CTA) of the right upper extremity showed no occlusive disease. Antiphospholipid antibodies and blood cultures were negative. There was no polycythemia or thrombocytosis to suggest myeloproliferative disorder. An arterial duplex of the upper right extremity revealed a 0.9 × 0.8 × 1.27 cm aneurysm in the right ulnar artery, with mural thrombus (Panel C). The patient was started on enoxaparin 1 mg/kg body weight twice daily. His symptoms resolved after starting anticoagulation. A few days later, a diagnostic angiogram of the right upper extremity revealed a saccular aneurysm in the fourth common palmar digital artery without evidence of thrombosis (Panel D). Subsequently, the patient underwent surgical excision of the right ulnar artery aneurysm with an end-to-end anastomosis (Panel D).

Ulnar artery aneurysm is a rare vascular condition, and fewer than 250 cases have been reported in the literature. 1 Most common causes of ulnar artery aneurysm are vasculitis, connective tissue diseases, and trauma. 2 In this case, the presumed etiology of the ulnar artery aneurysm was remote trauma to the right hand in which he had sustained fracture of the right ring finger. Given the limited number of reported cases, the natural history of ulnar artery aneurysm remains poorly understood. Reported symptoms of ulnar artery aneurysm include numbness and tingling of fourth and fifth fingers due to compression of the ulnar nerve from aneurism and mural thrombus formation, and distal embolization leading to critical limb ischemia. 2 In symptomatic patients, surgical repair is recommended to avert digital emboli and alleviate pain arising from nerve compression. 3
Footnotes
Note – Images are in color online.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.