
Abstract

In honor of Dr. Jay D. Coffman (1928–2006), distinguished internist and researcher of vascular medicine and clinical cardiology, SVM sponsors an annual award in vascular medicine and biology research.
YOUNG INVESTIGATOR AWARD FINALIST
Poster No. 01
Abstract ID No. 1498332
Mechanistic interrogation of a gene-by-environment interaction informs segment-specific predisposition to thoracic aortic aneurysm in heritable aortopathies
Nicole K. Anderson, PhD1, Elena Gallo MacFarlane, PhD1, Jefferson J. Doyle, MD, PhD1, Katelynn A. Toomer, PhD1, Tyler J. Creamer, PhD1, Emily E. Bramel, BS1, Harry C. Dietz, MD2
1Johns Hopkins Medical Institutions, 2Johns Hopkins University
Background: The mechanism for regional vulnerability to thoracic aortic aneurysm is poorly understood. Bicuspid aortic valve with distal ascending aortic aneurysm (BAV/DAscAA) is the most common heritable aneurysm condition with a strong male bias. Unlike Marfan syndrome (MFS), which is characterized by aortic root aneurysm, little is known about the genetic and mechanistic causes of BAV/DAscAA although rare cases have been attributed to haploinsufficiency in NOTCH1. In a mouse model of MFS, calcium channel blocker (CCB) exposure shifts vulnerability to the DAscAA in an ERK1/2-, AT1R-, and PKC- dependent manner.
Methods: We applied ascending aortic RNA-sequencing to identify gene expression changes that occur in tight temporal sequence with conditional provocations including CCB exposure with or without concomitant rescue upon ERK1/2 antagonism. Candidate pathways and downstream mechanistic hypotheses were interrogated with targeted pharmacologic and/or genetic manipulations.
Results: Pathway analysis revealed enrichment of differentially expressed genes in the NOTCH or androgen receptor signaling pathways. Treatment of MFS mice with CCBs and the NOTCH antagonist DBZ resulted in hyper-acute acceleration of DAscAo growth and rupture. This could be prevented by concomitant ERK1/2, PKC, or AT1R antagonism, and the more severe phenotype observed in males could be normalized by androgen receptor antagonism. Further mechanistic interrogation led us to develop and rigorously test a hypothesis accounting for regional vulnerability that collapses upon composite expression of Rgs genes, encoding potent negative regulators of AT1R. CCBs or DBZ selectively suppress Rgs4 or Rgs5 expression, respectively, while selective deletion of the Rgs4 gene fully phenocopied the deleterious influence of CCBs. Both genes show natural low expression in the DAscAo and are suppressed in Marfan syndrome.
Conclusion: These data elucidate a mechanism for regional predisposition to thoracic aortic aneurysm and show that NOTCH signaling is protective in the face of underlying disease predisposition. Identical results were found in mouse models of other inherited aortopathies including Loeys-Dietz syndrome.
YOUNG INVESTIGATOR AWARD FINALIST
Poster No. 02
Abstract ID No. 1494042
Light exposure alters platelet-mediated thrombosis
Elizabeth Andraska, MD1, Mohammad Zarisfi, BS2, Fredrik Denorme, BS3, Matthew Rosengart, MD2, Robert Campbell, PhD3, Matthew Neal, MD2
1UPMC, 2University of Pittsburgh, 3University of Utah
Background: The risk of thrombotic events such as venous thrombosis (VT) and stroke have been found to oscillate with the day-light cycle. The aim of this study was to investigate the impact of altering light exposure on platelet function in thrombosis.
Methods: WT C57BL/6J mice were exposed to ambient (micewhite, 300lux) or long wavelength red light (micered, 617nm, 1,700lux). After 72 hours of light exposure, platelet aggregation and activation were measured. Platelets were isolated and evaluated for transcriptomic and metabolomic changes. The ability of released products of platelet activation to induce thrombosis-generating NET formation was quantified. Subsequent thrombosis was measured using a murine models of VT and stroke. Hemostasis was measured with tail bleeding assays and coagulation biomarkers. We compared patients undergoing cataract surgery with implantation of low-wavelength filtering intraocular lenses (IOL) versus natural IOL over 8-years for risk of VT using multivariable logistic regression clustered by hospital.
Results: Exposure to long wavelength red light resulted in reduced platelet aggregation (micered 16.0±4.1 vs. micewhite 23.8±5.6 Ohm, p=.02) and activation (P-selectin; micered 35.2% vs. micewhite 53.2%; p=.02; Figure 1). Hemostasis assays were not significantly different between groups when mice were exposed to different wavelengths of light. RNA-seq analysis demonstrated no significant transcriptomic changes between micered and micewhite. There were global metabolomic changes in platelets from micered compared to micewhite. Releasate from activated platelets resulted in reduced NET formation (fold increase from control: micered 1.1 vs. micewhite 1.9, p=.03). Micered had reduced VT weight (micered 4.2±5.1 mg vs. micewhite 16.5±7.7 mg; p < .01) and brain infarct size following stroke (micered 38.8±17.6 mm3 vs. micewhite 73.3±15.0 mm3; p < .01). In a risk adjusted analysis, low-wavelength filtering IOL were associated with a reduced risk of VTE (OR 0.89; 95% CI 0.80-0.99; p=.04).
Conclusion: Exposure to long wavelength red light results in reduced platelet aggregation and activation. Light exposure modulation is a promising alternative for prophylaxis of venous and arterial thrombosis.
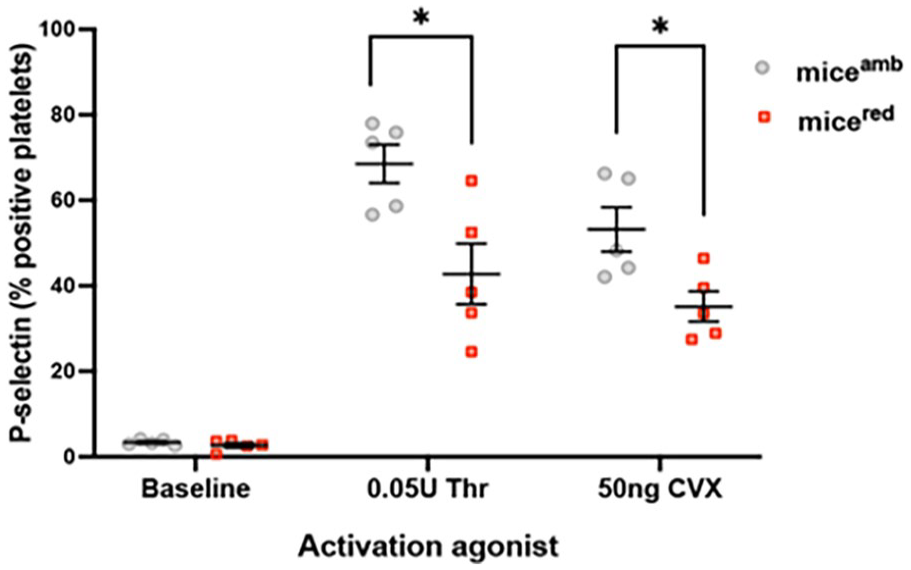
Platelet activation (CD41+/P-selectin +) is reduced in micered compared to micewhite (amb).
YOUNG INVESTIGATOR AWARD WINNER
Poster No. 03
Abstract ID No. 1495937
Androgen and mineralocorticoid receptor signaling contribute to pubertal vascular rupture in vascular Ehlers-Danlos syndrome (VEDS) mice
Emily Juzwiak, BS, Caitlin Bowen, MD PhD, Anthony Zeng, MS, Harry C. Dietz, MD
Johns Hopkins University
Background: Males with VEDS are at a high risk of spontaneous death due to arterial rupture during puberty compared to females. Our VEDS mouse model (Col3a1G938D/+) recapitulates this sexually dimorphic vulnerability, with 51% vs. 63% survival of males vs. females at 60 days of age, respectively.
Methods: Given the male bias of death at puberty, we hypothesized that vascular rupture involved androgen-dependent perturbation of cellular function. We treated Col3a1G938D/+ mice with the selective AR antagonist (ARa) bicalutamide or the dual ARa and mineralocorticoid receptor antagonist (MRa) spironolactone from weaning until 60 days of age. We also initiated treatment of Col3a1G938D/+ mice with spironolactone after the completion of puberty. As a control, we treated Col3a1G938D/+ mice with the selective MRa finerenone from weaning until 60 days of age. We also induced the null state for the AR in Col3a1G938D/+ mice using a conditional (floxed) allele for the Ar gene in combination with an allele that globally express Cre recombinase.
Results: We observed that male Col3a1G938D/+ AR null mice have improved survival compared to untreated Col3a1G938D/+ mice at 60 days (80% vs. 51%), a protective performance similar to treatment with bicalutamide (69% survival). Immunoblot analysis of aortic lysates showed that AR blockade, either chemical or genetic, normalizes activation of the PKC/ERK axis. These data suggest that AR signaling contributes to vascular disease in Col3a1G938D/+ mice. Notably, male Col3a1G938D/+ mice treated with the dual ARa/MRa spironolactone showed the best performance (92% survival at 60 days). Interestingly, use of the selective MRa finerenone afforded intermediate protection (83% male survival at 60 days). Identical trends were observed in female Col3a1G938D/+ mice. Postpubertal treatment with spironolactone afforded essentially complete protection in both sexes.
Conclusion: These data document that pubertal vascular catastrophe in Col3a1G938D/+ mice is dependent on both AR and MR signaling with dramatic protection afforded by dual antagonism. There is therapeutic potential for isolated MR antagonism that will maintain normal sexual development in adolescent males.
YOUNG INVESTIGATOR AWARD FINALIST
Poster No. 04
Abstract ID No. 1497207
Lipedema and lymphedema as independent risk factors for venous thromboembolism
Muhammad Umar Khalid, MD1, Sameer Prasada, MD1, Courtney Jennings2, Matthew Godwin1, John Bartholomew, MD1, Wei Chen, MD1, Douglas Joseph, DO1, Graham Schwartz, MD1, Scott Cameron, MD, PhD1, Rohan Bhandari, MD1
1Cleveland Clinic Foundation, 2Case Western Reserve University
Background: Lymphedema is an inflammatory vascular disorder manifesting as lymphatic dysfunction and is associated with difficulties in ambulation which may portend a higher risk of venous thromboembolism (VTE). Lipedema is an inflammatory disorder of limb adipocytes often mistaken for lymphedema. Obesity is also an inflammatory condition that increases VTE risk. Since patients with lymphedema or lipedema (LL) often have increased BMI, we considered the effect of LL on VTE in obese patients.
Methods: The Nationwide Inpatient Sample from 2016-2019 was queried for patients with a discharge diagnosis of Obesity using International Classification of Disease, 10th revision, Clinical Modification coding. Male gender and patients with age < 18 years were excluded. We used t-tests and chi-square tests to compare baseline characteristics. Patient sample was matched using nearest neighbor matching. Uni- and multivariate logistic regression identified predictors of VTE. Clot formation kinetics in plasma of patients with lymphedema and lipedema were evaluated by video-microscopy.
Results: 188,003 (0.8%) patients with LL were selected. LL patients were more likely to be obese than those without LL (48% and 17%, respectively). LL was one of the strongest independent predictors of VTE (OR 1.69; 95% CI 1.61-1.72; p< 0.01) compared with obesity alone (OR 1.27; 95% CI 1.24-1.27, P< 0.01). In obese patients, LL increased the odds of VTE (OR 1.4; 95% CI 1.36-1.45; p< 0.01). In a propensity matched analysis, Lipedema and Lymphedema were independent predictors of VTE in obese patients (OR 1.2; 95% CI 1.03-1.41; p=0.02) and (OR 1.4; 95% CI 1.26 – 1.49; p< 0.01) respectively. Fibrin clot formation kinetics for matched healthy subjects (n=21) were 28307U ± 1212 vs. 32949 U ± 1199 (p=0.02) for lymphedema (n=25) vs. 31274U ± 11086 (p=0.24) for lipedema (n=29).
Conclusion: Patients with LL have risk of VTE that is distinct from obesity. In addition, obese patients with lymphedema and lipedema have a higher risk of VTE events. These results are also confirmed by evaluation of thrombosis ex vivo that is driven more by a lymphedema phenotype.
Poster presentations
FEATURED YOUNG INVESTIGATOR
Poster No. 05
Abstract ID No. 1496264
Time course of improved walking performance and patient reported outcome measures in response to supervised treadmill exercise in peripheral artery disease: a randomized clinical trial
Nina C. Byskosh, BS1, Lu Tian, D.Sc2, Lihui Zhao, PhD1, Dongxue Zhang, MS1, Mary M. McDermott, MD1
1Northwestern University Feinberg School of Medicine, 2Stanford University School of Medicine
Background: Supervised exercise therapy is first line therapy for improving walking impairment in peripheral artery disease (PAD). The typical time required for supervised exercise to produce meaningful improvement in walking performance is unclear. This study identified the typical time course of improved walking performance in response to supervised treadmill exercise in people with PAD.
Methods: In a clinical trial, PAD participants were randomized to supervised treadmill exercise or a non-exercise control group for six months. Changes in 6-minute walk, treadmill walking distance, and the Walking Impairment Questionnaire (WIQ) distance score were compared between intervention and control at 6-weeks, 3-months, and 6-month follow-up.
Results: Among 210 randomized participants (mean 67 years, 38% female, 67% Black), 200 (95%) completed at least one follow-up. Results are shown in the Table.
Conclusion: More than six weeks of supervised treadmill exercise were required to attain meaningful improvements in six-minute walk, with large and meaningful benefits attained by 12-week follow-up. In contrast, effects of supervised treadmill exercise on patient reported outcomes measures were not durable.
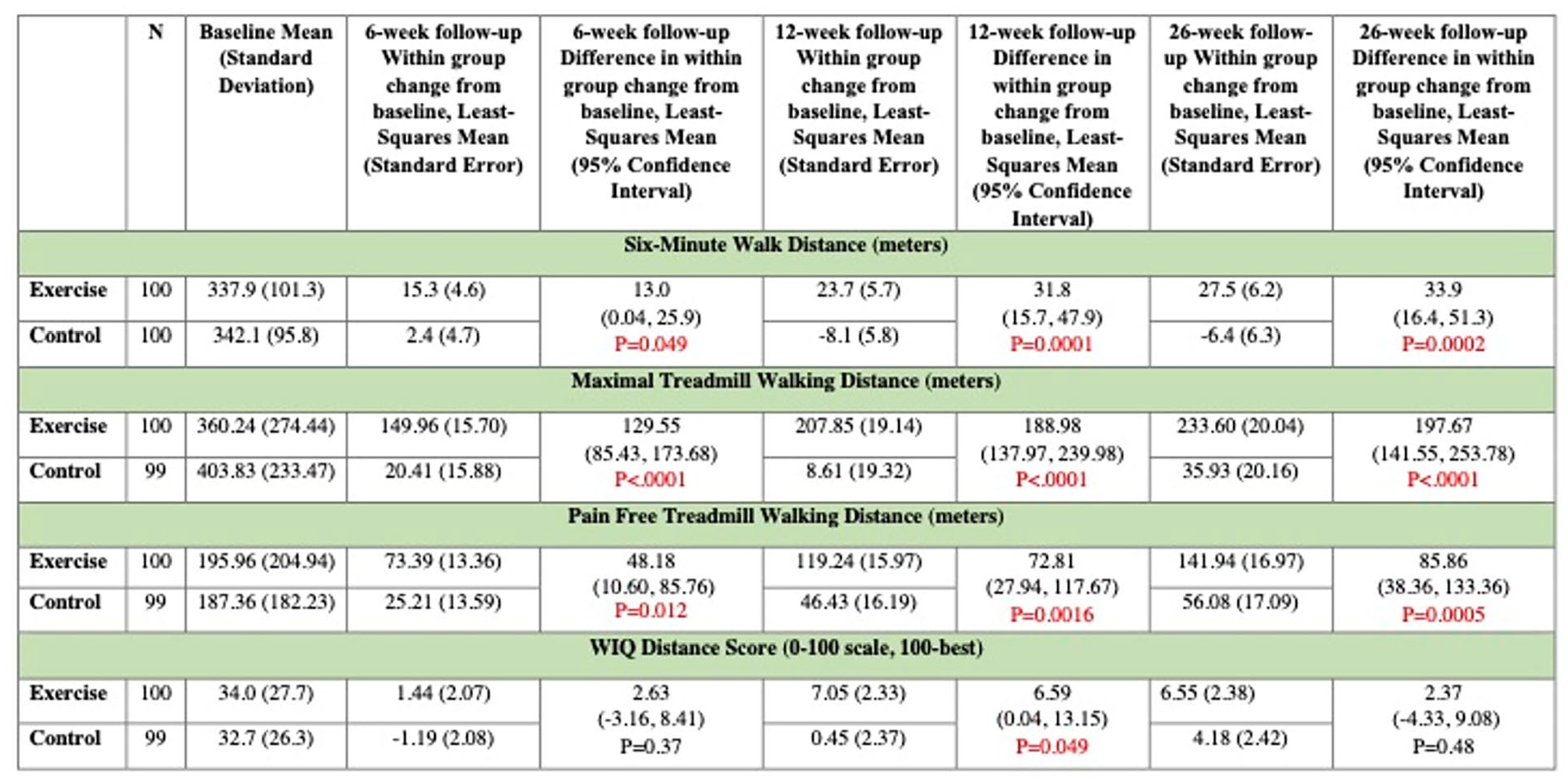
Temporal changes in walking outcomes in response to supervised exercise in peripheral artery disease.
FEATURED YOUNG INVESTIGATOR
Poster No. 06
Abstract ID No. 1511334
Utilizing an induced pluripotent stem cell platform to model arterial calcification resulting from deficiency of CD73
Chikage Noishiki, MD, PhD1, Tom Alsaigh, MD2, David Wu, BS1, Shaunak Adkar, MD, PhD1, Venita Chandra, MD1, Derek Klarin, MD1, Jason Lee, MD1, Eri Fukaya, MD, PhD1, Nicholas Leeper, MD1, Nazish Sayed, MD, PhD2
1Stanford University, 2Stanford University School of Medicine
Background: Vascular calcification is prevalent in atherosclerosis, diabetes and chronic kidney disease, and affected patients often suffer from significant morbidity and mortality related to complications of disease progression. The pathophysiology is not well known, and studies suggest involvement of a complex dynamic process between bone development and metabolism. The protein encoded by CD73 (NT5E) is involved in the conversion of AMP to Adenosine, a pathway necessary to block physiologic calcification and mutations in NT5E have been associated with arterial calcification. Arterial Calcification due to Deficiency of CD73 (ACDC) is a rare and poorly understood adult-onset vasculopathy consisting of large build-up of calcium.
Methods: We perform whole genome sequencing (WGS) of arterial tissue from a patient with severe arterial calcification of unknown etiology requiring serial limb amputations in the setting of poor extremity perfusion. We identified three culprit variant NT5E gene mutations known to affect patients with ACDC. Furthermore, to understand the ACDC pathophysiology in-a-dish, we generated induced pluripotent stem cells (iPSC) from the patient’s PBMCs and differentiated them to endothelial (ECs) and smooth muscle cells (SMCs).
Results: Patient-specific iPSC-ECs exhibited endothelial dysfunction as evident by their decreased capacity to form vascular networks or generate nitric oxide.
Conclusion: These results lay the groundwork to unravel the mechanisms underlying ACDC by conducting genome editing experiments to precisely identify the NT5E variant responsible for disease severity. Importantly, our iPSC platform provides an opportunity to set up drug screening experiments to evaluate treatment options for afflicted patients.
YOUNG INVESTIGATOR POSTER
Poster No. 07
Abstract ID No. 1495985
A quantitative analysis of lymphedema patient perceptions and subjective outcomes within the healthcare system
Catharine Bowman, BHFC1, Stanley G. Rockson, MD2
1Stanford University, 2Stanford University School of Medicine
Background: Lymphedema is an incurable, progressive lymphatic disease that potentiates physical and psychosocial distress. Patients report lymphatic ignorance throughout the healthcare system, yet there is minimal epidemiologic evidence to substantiate the subjective burden of relative disease neglect. This study was designed to characterize patient reported lymphedema interactions within the American healthcare system.
Methods: We implemented a cross-sectional design . A 23-item, unbiased online questionnaire was anonymously distributed to self-identified lymphedema patients utilizing social media and organizational platforms. Clinical characteristics, healthcare experiences and patient satisfaction were analyzed with descriptive statistics. For validation, a focus group of active lymphedema patients was interrogated with a similar array of questions before and after exposure to a didactic lecture about lymphedema detection, diagnosis and treatment. Descriptive statistics were performed with SAS software.
Results: The questionnaire was completed by 1739 participants. More than half of the respondents had cancer-related lymphedema (CRL, 52.4%). The impact of lymphedema on quality of life was greater in participants with non-CRL than with CRL (P< 0.05). Both non-CRL and CRL respondents reported similar levels of physician disinterest in the lymphedema; however, non-CRL patients reported more dissatisfaction with the lymphedema diagnosis and treatment (P< 0.05). Participants experienced substantial delays in diagnosis and treatment, with 45.9% of CRL and 81.3% of non-CRL patients requiring consultation with more than one physician prior to diagnosis (P< 0.05). These findings were validated through the observations of the in-person lymphedema focus group.
Conclusion: Lymphedema has substantial impact upon patient well-being. Nevertheless, patients continue to face delays in diagnosis and treatment, and remain dissatisfied with their current lymphatic healthcare. This is the first formal attempt to validate and quantitate levels of dissatisfaction within the patient community. Research and reform are needed to optimize lymphatic healthcare education and delivery within the U.S. medical system.
YOUNG INVESTIGATOR POSTER
Poster No. 08
Abstract ID No. 1493396
Comparative performance of bleeding risk scores (IMPROVE and HAS-BLED) among critically ill and non-critically ill patients with prophylactic dose of enoxaparin admitted at a tertiary hospital: a prospective cohort study
Rowena Q. Javonillo, Jasmin Melissa B. Bernardo, Paolo Joel T. Nocom
Philippine Heart Center
Background: In patients who need prophylactic anticoagulants for venous thromboembolism (VTE), the benefits and the risks of bleeding must be weighed to potentially prevent its occurrence. This study was conducted to compare the IMPROVE bleeding risk score (BRS) with the HAS-BLED BRS in predicting anticoagulant-related bleeding events in the critically-ill and non-critically ill patients admitted at a tertiary hospital who were given prophylactic dose of enoxaparin for VTE.
Methods: Sixty nine (69) patients admitted in the intensive care unit (ICU) and ward, who were given prophylactic dose of enoxaparin were included in the study and followed up until discharge. Their demographic data, comorbid conditions, IMPROVE and HAS-BLED BRS were noted during admission and they were followed up for bleeding events.
Results: Sixteen percent of these patients (11) had episodes bleeding (major and minor) in the study population. An IMPROVE BRS ⩾7 (high risk) had more statistically significant bleeding events compared to those who had scores of < 7 (low risk) (p < 0.001). The mean HAS-BLED BRS was 2.20 (±1.09); and those with higher HAS-BLED BRS did not necessarily signify statistically significant bleeding events (bleeding event, 2.73 [±1.19] vs. no bleeding event, 2.09 [±1.04], p = 0.079). The IMPROVE BRS had an area under the curve (AUC) of 0.96, while the HAS-BLED BRS had an AUC of 0.67 in predicting anticoagulant-related bleeding events.
Conclusion: In patients receiving prophylactic dose anticoagulant for VTE, the IMPROVE BRS was superior to predict major anticoagulant-related bleeding events compared to HASBLED BRS with higher sensitivity, specificity and accuracy. Both risk scoring system are helpful in assessing the risk of bleeding prior to pharmacologic VTE prophylaxis. However, the IMPROVE BRS was more accurate in predicting bleeding events.
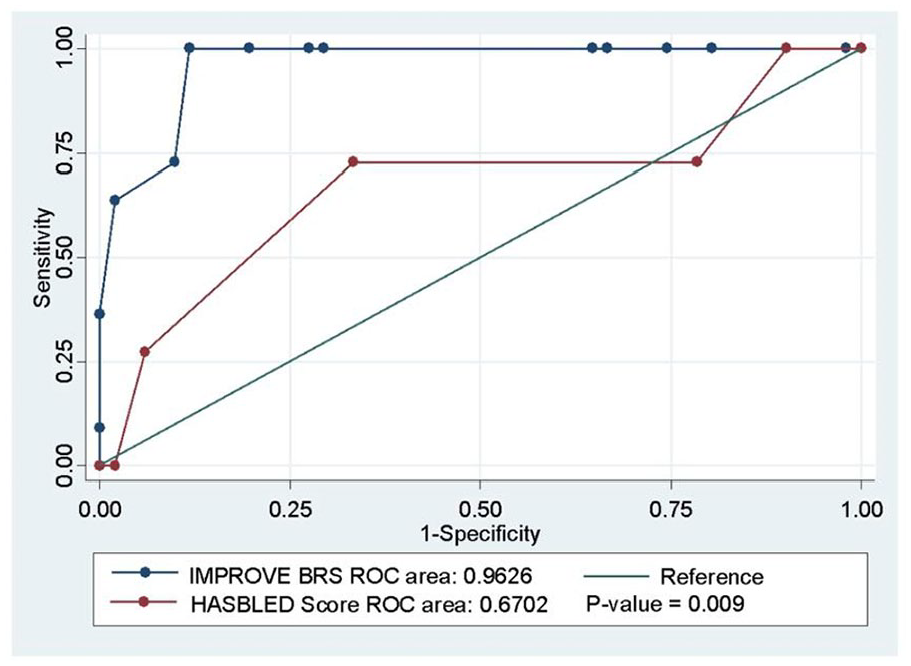
Area under the ROC curve of different bleeding risk score to accurately diagnose anticoagulant-related bleeding events.
YOUNG INVESTIGATOR POSTER
Poster No. 09
Abstract ID No. 1492366
Speckleplethysmography (SPG) for wearable continuous hemodynamic monitoring
Helen E. Parker, PhD1, Elise M. Berning1, Brian Hill1, Timothy Quang, PhD1, John Kakareka2, Thomas Pohida2, Dahianna M. Gallo, MD, PhD3, Mariachiara Bosca, MD3, Roberto Romero, MD1, Bruce J. Tromberg, PhD2
1Eunice Kennedy Shriver National Institute of Child Health and Human Development, 2National Institute of Biomedical Imaging and Bioengineering, 3Wayne State University
Background: Photoplethysmography (PPG) is a non-invasive technique whereby the interaction of light with tissue is used to determine pulsatile changes in blood volume. The PPG signal is typically acquired from a peripheral digit and some studies have found correlations of PPG to various hemodynamic states. However, PPG signals suffer from poor signal-to noise, sensitivity to low perfusion (such as during vasoconstriction) and loss of fidelity with increasing vascular resistance. Speckleplethysmography (SPG) is an emerging optical technique which measures blood flow, rather than volume. SPG can be deployed in the same, wearable form-factor as PPG, but without many of the same drawbacks. To date, little work has been done to characterize SPG in a clinical population. We compared the signal fidelity of co-registered PPG and SPG in a clinical setting and explored the feasibility of using SPG to monitor hemodynamics during perturbations.
Methods: We conducted a pilot study with a cohort of pregnant women with and without hypertensive disorders (6 hypertensive, 19 normotensive). We collected ECG, PPG, SPG, and blood pressure data from each participant during a baseline period and during a breath-hold challenge. To assess the signal fidelity of PPG and SPG we used a normalized pulse amplitude (NPA) metric. The frequency components of the signal related to the pulses (0.2 - 15 Hz) were normalized against the low frequency components (< 0.2 Hz) of the signal. The amplitudes of the normalized pulses were then calculated across all participant data.
Results: We found the mean NPA of SPG was at least an order of magnitude greater than PPG (70.9 ±27.5 and 1.0 ±0.7, respectively). Furthermore, we found that SPG retained its NPA during breath-holds and PPG did not (77.9 ± 34.2 and 0.59 ± 0.46, respectively).
Conclusion: With higher signal fidelity and robustness to perturbations, SPG is a promising alternative to PPG. For example, preliminary results suggest we can even correlate harmonic features of the higher fidelity SPG to beath-holds. Future work will involve a healthy volunteer study (n=50) to assess SPG as a modality for measuring vascular stiffness, rheological properties, cardiac function and blood pressure.
YOUNG INVESTIGATOR POSTER
Poster No. 10
Abstract ID No. 1485739
Ischemic leg symptom severity and response to supervised exercise in peripheral artery disease (PAD): results from three randomized clinical trials
Mary O. Whipple, PhD, RN, PHN1, Lihui Zhao, PhD2, Lu Tian, D.Sc3, Dongxue Zhang, MS2, Mary M. McDermott, MD2
1University of Minnesota, 2Northwestern University Feinberg School of Medicine, 3Stanford University School of Medicine
Background: In a clinical trial of home-based walking exercise for PAD, ischemic leg symptoms during exercise were necessary to achieve significant improvement in walking performance. This study evaluated whether, among people with PAD, more severe ischemic leg symptoms during walking at baseline was associated with greater improvement in six-minute walk (6MW) in response to a supervised walking exercise intervention.
Methods: Data were combined from individual participants from three randomized trials comparing supervised treadmill exercise to a control group. To measure severity of ischemic leg symptoms, participants ranked their degree of difficulty walking due to calf or buttock symptoms on a 1-5 scale (5-worst). The primary outcome was 6-month change in 6MW.
Results: Of 427 people randomized (59% Black; 43% women), participants with more severe ischemic leg symptoms during walking at baseline had greater improvement in 6MW at 6-months follow-up, compared to control (Table).
Conclusion: Compared to less severe ischemic leg symptoms at baseline, more severe ischemic leg symptoms at baseline were associated with greater response to a supervised treadmill exercise intervention. These results suggested that ischemic leg symptoms were necessary for meaningful improvement in response to walking exercise in PAD.
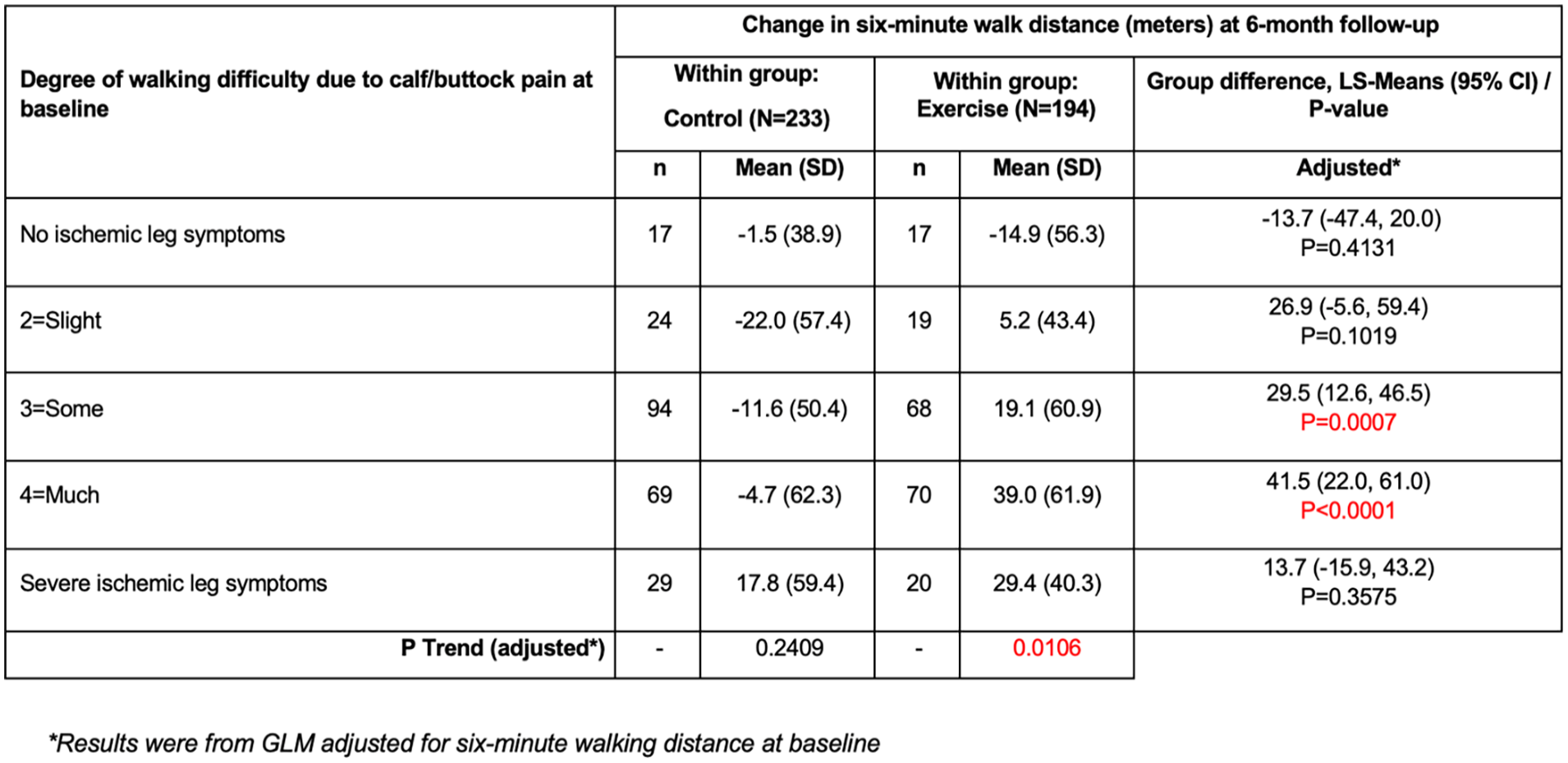
Six-month changes in six-minute distance in the exercise and control groups, according to baseline severity of ischemic leg symptoms during walking.
YOUNG INVESTIGATOR POSTER
Poster No. 11
Abstract ID No. 1506600
Identifying novel variants associated with hemangiomas using an International Classification of Diseases (ICD-10) based approach in the UK biobank
Fahad Alkhalfan, MD, Alex Gyftopoulos, MD, Yi-Ju Chen, MS, Charles Williams, PhD, James Perry, PhD, Charles Hong, MD, PhD
University of Maryland
Background: Hemangiomas, benign tumors of vascular endothelium, are some of the most common tumors of childhood. Although its etiology is not well understood, the most likely proposed hypothesis is that hypoxic stress upregulates vascular endothelial growth factor 1 (VEGF1) leading to mobilization of endothelial progenitor cells. Additionally, it is believed to be partly hereditary. Understanding the genetic component of hemangiomas can help us further our understanding of this condition.
Methods: The UK Biobank is a prospective cohort with genetic and clinical data on over 500,000 individuals. We ran a genome-wide association study to identify variants associated with hemangiomas (ICD-10 code D180). We compared cases to age, sex, and ancestry matched controls in a 1:20 ratio. We used a cut-off of 1x10-6 to identify variants with possible significance and a cut-off of 5x10-8 for statistical significance. We restricted the analysis to variants with minor allele frequency (MAF) greater than 0.5%.
Results: There were 2005 individuals with the diagnosis of hemangiomas in the UK Biobank. We identified 14 variants for 8 genes with p < 1x10-6. Of those, one variant had p < 5x10-8 (the intronic SNP rs561170328 in AGAP1 (ArfGAP with GTPase domain, ankyrin repeat and PH domain 1) with OR 2.7, p = 5.1 x 10-9, 95% CI 1.9 – 3.7, MAF of 0.51%). Other potential variants of interest include rs71645268 (intronic in COP1 (COP1 E3 ubiquitin ligase), OR 2.3, p = 3.5 x 10-7, 95% CI 1.7 – 3.3, MAF 0.5%) and rs10954423 (best of 5 intronic variants in linkage disequilibrium, located in EXOC4 (Exocyst complex component 4), OR 1.2, p = 5.3 x 10-7, 95% CI 1.12 – 1.29, MAF 23.2%).
Conclusion: Using data from the UK Biobank, we identified a novel variant in AGAP1 that was significantly associated with an increased risk of hemangiomas. Although little is known about the link between AGAP1 and hemangiomas, recent studies have suggested that mutations in AGAP1 can lead to adverse outcomes in patients who receive bevacizumab (a monoclonal antibody targeting VEGF). This supports the notion that VEGF may play a role in the development of hemangiomas. Further studies are required to verify the results of this analysis and the applicability of these findings to other VEGF-related conditions.
YOUNG INVESTIGATOR POSTER
Poster No. 12
Abstract ID No. 1508773
Utilizing an International Classification of Diseases (ICD-10) based approach to identify novel variants associated with colonic angiodysplasia in the UK biobank
Fahad Alkhalfan, MD, Alex Gyftopoulos, MD, Yi-Ju Chen, MS, Charles Williams, PhD, James Perry, PhD, Charles Hong, MD, PhD
University of Maryland
Background: Colonic angiodysplasia is characterized by progressive degenerative malformation of the gastrointestinal (GI) tract vessels leading to fragile and often leaky vessels. It is the second leading cause of lower GI bleed in adults over the age of 60. While it’s cause is unknown, one of the most accepted theories is that it occurs due to degenerative changes to small blood vessels that is associated with aging. It is not known if colonic angiodysplasias has a genetic component.
Methods: The UK Biobank is an ongoing prospective cohort study with data from over 500,000 individuals. We conducted a genome-wide association study to identify variants associated with the ICD-10 diagnosis of colonic angiodysplasia (K55.2). We compared cases to controls in a 1:20 ratio and matched for age, sex and ancestry. We used a cut-off of 5x10-8 for statistical significance to assess for statistical significance. We restricted our analysis to variants with a minor allele frequency (MAF) of greater than 0.5%.
Results: There were 704 individuals who carried the diagnosis of colonic angiodysplasia. We identified 18 variants that met the threshold for statistical significance. The most significant variant was rs10109912 in chromosome 8 which had an odds ratio of 0.68, p = 2.4 x 10-10, 95% CI 0.61 – 0.77, and MAF 36.6%. rs10109912 is a missense variant for one of the transcripts of TNFRSF10C (TNF receptor superfamily member 10c) which would produce a mutant protein.
Conclusion: We identified several variants associated with colonic dysplasia, the most significant of which was rs10109912. The location of rs10109912 suggests that it may affect the expression of TNFRSF10C. The variant lies in the transcription-factor binding site for POLR2A and also lies in an enhancer region as identified by the GeneHancer study. Previous studies showed that TNFRSF10C promotes AKT phosphorylation and is believed to play a role in the PI3K-AKT pathway. The PI3K-AKT pathway is involved in endothelial functions such as regulation of vascular tone, control of adhesion and angiogenesis. This may contribute to the occurrence and progression of colonic angiodysplasia. Further studies are required to verify the results of this analysis.
HIGHLIGHTED ORIGINAL RESEARCH
Poster No. 13
Abstract ID No. 1495957
A Comparison of genetic variants associated with cutaneous and systemic vasculitis using an International Classification of Diseases (ICD-10) based approach in the UK biobank
Fahad Alkhalfan, MD, Alex Gyftopoulos, MD, Yi-Ju Chen, MS, Charles Williams, PhD, James Perry, PhD, Charles Hong, MD, PhD
University of Maryland
Background: Cutaneous vasculitis consists of a group of inflammatory disorders that affect the skin blood vessels and has no visceral involvement. Visceral involvement, if occurs, can present later, revealing an underlying systemic process. Prior to the diagnosis of cutaneous vasculitis, a workup is required to rule out systemic involvement. Since genes contribute to the pathogenesis of vasculitis, it may also help differentiate between cutaneous and systemic vasculitis.
Methods: The UK Biobank is a prospective cohort that contains clinical and genetic data from over 500,000 individuals. We ran two genome-wide association studies (GWAS) to identify variants associated with cutaneous vasculitis [ICD code L95] and systemic vasculitis [ICD codes I73.1, M05.2, M30.0, M30.1, M30.2, M30.8, M30.3, M31.3, M31.7, M31.2, M31.4, M31.5 and M31.6]. We compared cases to age, sex, and ancestry-matched controls in a 1:20 ratio. We used a cut-off of 1x10-6 to identify variants with possible significance and a cut-off of 5x10-8 for statistical significance. We only assessed genes outside the HLA locus on chromosome 6.
Results: There were 161 and 925 cases of cutaneous and systemic vasculitis respectively. In the cutaneous vasculitis group, we identified 28 variants linked to 19 genes with p< 1x10-6. Of those, 3 variants linked to 3 genes with p< 5x10-8: ITK (IL2 inducible T cell kinase) OR 8.9, P= 1.9x10-10; PEX14 (peroxisomal biogenesis factor 14) OR=5.5, p = 3.9x10-8; RTL4 (retrotransposon Gag like 4) OR=2.9, p = 4.68x10-8. In the systemic vasculitis group, we identified 28 variants linked to 11 genes with p< 1x10-6. Of those, 1 had p< 5x10-8 (MIR4318 (microRNA 4318) OR=3.4, p = 2.6x10-8). There was no overlap in the variants that met the p< 1x10-6 threshold between the two groups.
Conclusion: Using the UK Biobank, we identified variants in both systemic and cutaneous vasculitis with p< 1x10-6. Both IL2 and peroxisomes are involved in regulating inflammation. Additionally, microRNAs have been associated with ANCA vasculitis. The lack of overlap suggests that there is a potential to utilize genetics to differentiate between cutaneous and systemic vasculitis with a greater degree of accuracy. Further studies are required to verify the results of this analysis.
HIGHLIGHTED ORIGINAL RESEARCH
Poster No. 14
Abstract ID No.1511569
Differences in proteomic composition of retrieved stroke emboli associated with susceptibility to in vitro thrombolysis
Sajal K. Akkipeddi, BA, Redi Rahmani, MD, Nathaniel R. Ellens, MD, Derrek A. Schartz, MD, Logan M. Worley, BA, Siddharth Chittaranjan, BA, Tarun Bhalla, MD, PhD, Thomas K. Mattingly, MD, MSc, Matthew T. Bender, MD
University of Rochester Medical Center
Background: Fibrin, von Willebrand factor, and extracellular DNA from neutrophil extracellular traps (NETs) all contribute to AIS thrombus integrity. The understudied proteome of thrombi provides a quantitative avenue for exploring susceptibility to pharmacotherapy.
Methods: Thromboembolic material from 26 AIS patients retrieved by mechanical thrombectomy was portioned into four representative segments. A small piece of each representative segment was collected and pooled for mass spectrometry to generate a proteome for the corresponding thrombus. The remainder of the four segments were subjected to one hour of in vitro lysis at 37ºC in one of four lytic solutions with: the standard-of-care tissue plasminogen activator (T), tPA + von Willebrand factor-cleaving ADAMTS13 (TA), tPA + DNA-cleaving DNase I (TD), and all three enzymes (TDA). Post-lysis residual, characterized by the post-lysis thrombus weight as a percent of the pre-lysis weight, was compared across the four solutions. Spearman coefficients were used to describe the association between lysis and the abundance of each of 2,790 proteins identified by mass spectrometry.
Results: Post-lysis residual in the T condition was significantly greater than in the TD or TDA conditions (post-hoc Tukey, p < 0.01). Numerous proteins were strongly positively and negatively associated with lysis in each of the four lytic solutions. Notably, several histone protein signatures were associated with greater post-lysis residual in the T and TA conditions (Spearman’s ρ > 0.39 for all). However, these same proteins were associated with less residual in the t and TDA conditions (Spearman’s ρ < 0.40 for all).
Conclusion: This study demonstrates a synergistic effect of DNase and tPA in the in vitro lysis of stroke emboli. Proteomic analysis suggests that composition is directly associated with susceptibility to lysis. Specifically, DNA composition of clots, and thus NET load, is associated with decreased residual when subjected to DNase in addition to tPA, hinting at a potential pharmacologic target in the treatment of AIS.
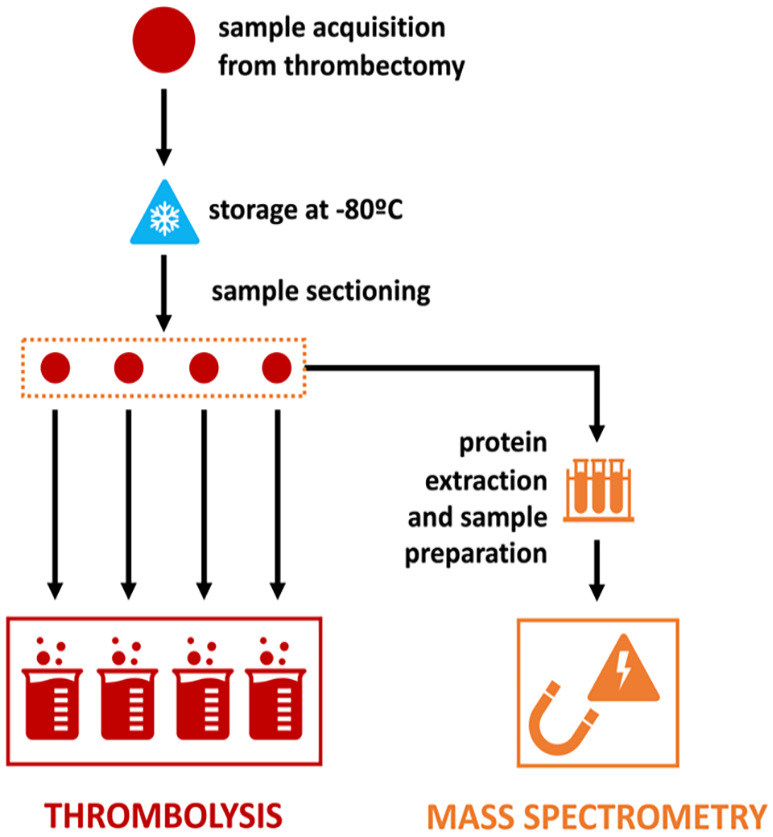
Sample processing schema for thrombolysis with matched sample mass spectrometry.
HIGHLIGHTED ORIGINAL RESEARCH
Poster No. 15
Abstract ID No. 1511485
Characteristics of people with PAD identified with ankle brachial index testing in three U.S. cities
Madeline Cetlin, BA1, Shujun Xu, MS1, Lihui Zhao, PhD1, Lu Tian, D.Sc2, Mary M. McDermott, MD1
1Northwestern University Feinberg School of Medicine, 2Stanford University School of Medicine
Background: The extent and significance of clinically undiagnosed PAD is unclear. As part of recruitment for randomized clinical trials of people with lower extremity peripheral artery disease (PAD), these analyses compared characteristics of people with PAD (ankle brachial index (ABI) < 0.90) identified using mailed postcards in three U.S. cities to patients with established PAD identified from medical centers in the same three cities.
Methods: To recruit people with PAD for randomized clinical trials, mailing lists were purchased and postcard advertisements were mailed to people age 50 and older living in Chicago, Minneapolis, and New Orleans. The postcards invited people with “difficulty walking” and cardiovascular risk factors to call a telephone number to learn about randomized clinical trials testing interventions for people with PAD. Individuals with difficulty walking who were interested in clinical trial participation were invited to attend a study visit for ABI testing. Patients with established PAD from medical centers in the same cities were also invited to participate in the randomized trials. All participants underwent evaluation that included walking performance measures and medical history.
Results: Of 2,431 identified from the community who underwent ABI testing, 499 (20.5%) had an ABI < 0.90, consistent with PAD. Characteristics of these 499 people were compared to 184 with PAD identified from a medical center in the same three cities.
Conclusion: 20.5% of people in three US metropolitan cities identified using mailed postcards who reported walking difficulty had an ABI < 0.90 consistent with PAD. Compared to people with PAD identified from a medical center in the same three cities, those with PAD identified from the community had significantly greater walking impairment and included a higher proportion of people who were Black.
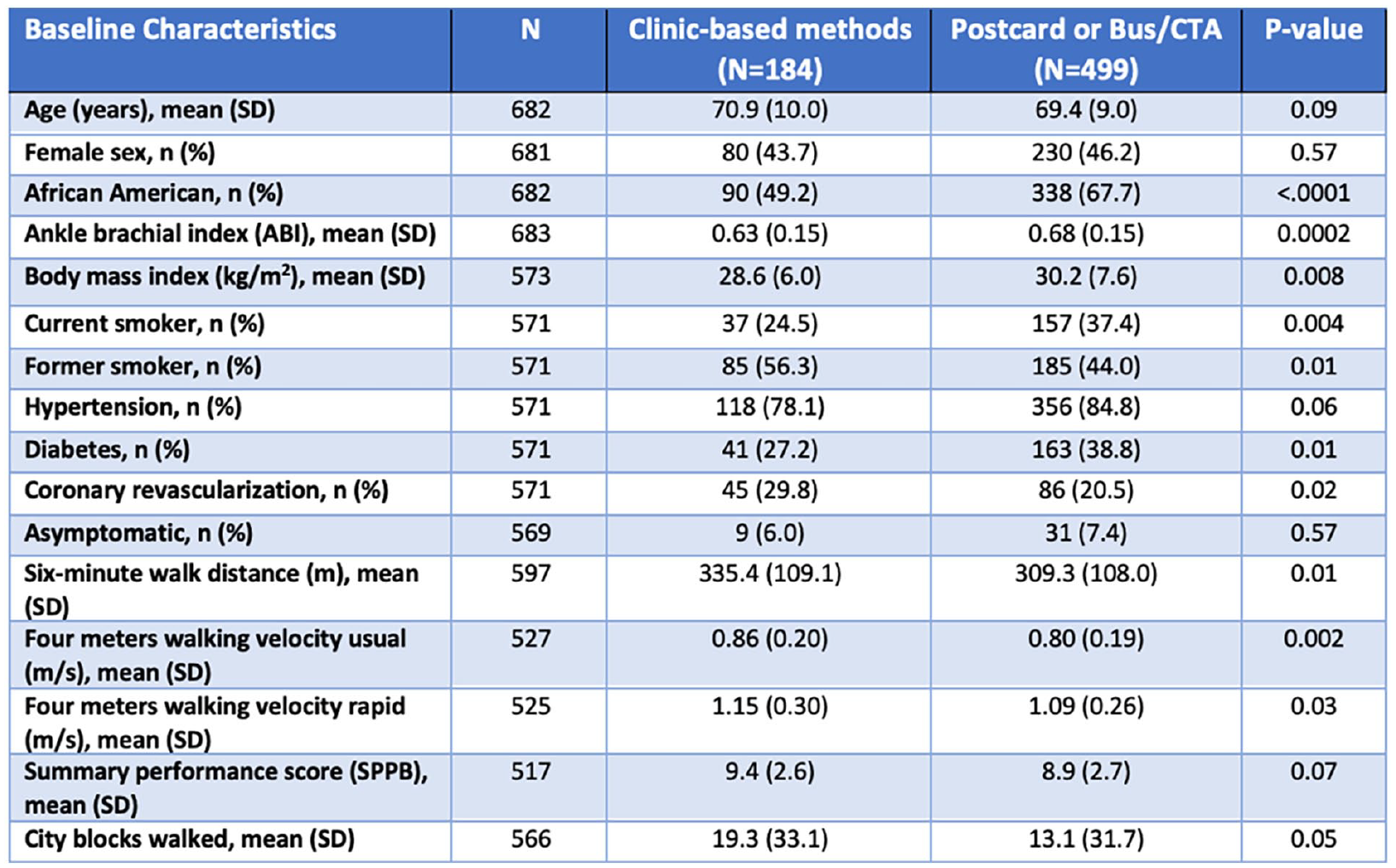
Characteristics of people with PAD identified from a community ABI testing program compared to those identified from a medical center in three U.S. cities.
HIGHLIGHTED ORIGINAL RESEARCH
Poster No. 16
Abstract ID No.1498745
The impact of the Affordable Care Act Medicaid expansion in patients with peripheral artery disease
Stanislav Henkin, MD, MPH, RPVI1, Stephen Kearing, MS2, Nikolaos Zacharias, MD, MPH3, Mark Creager, MD1, Philip Goodney, MD, MS1, Michael Young, MD1, Jesse Columbo, MD1
1Dartmouth-Hitchcock Medical Center, 2Dartmouth Institute for Health Policy and Clinical Practice, 3Massachusetts General Hospital
Background: In 2014, the Affordable Care Act Medicaid expansion (ME) increased Medicaid eligibility for adults with an income level up to 138% of federal poverty threshold, leading to an overall decline in the uninsured population by 47% in 2016. The impact of ME on the outcomes in patients with peripheral artery disease (PAD) is unknown. In this study, we examined the impact of ME on mortality and amputation in patients with PAD.
Methods: The 100% MedPAR and Part-B Carrier files from 2011-2018 were queried to identify all fee-for-service Medicare beneficiaries with PAD using ICD codes. Our primary exposure was whether a state had adopted the ME on January 1, 2014. Our primary outcomes were all cause 1-year mortality and major leg amputation. We used a state-level difference-in-differences (DID) analysis to compare the rates of the primary outcomes among patients who were in states who adopted ME (n=25) versus those who were in states that did not (n=26). We performed a pre-specified sub-analysis of patients who were Medicare/Medicaid dual eligible.
Results: Over the 8-year period, we studied 37,743,929 patients, with a mean age of 78.4±8.30 years; 54.4% were female, 8.2% were black, and 22.0% were Medicare/Medicaid dual eligible. The unadjusted 1-year mortality improved in both non-ME (9.76% to 9.32%, p< 0.001) and ME (9.21% to 8.77%, p< 0.001) states. Across the entire cohort, the DID model revealed that ME did not lead to a significant change in mortality (p=0.87). Among dual eligible patients, the unadjusted rate of death increased in non-ME states (15.27% to 15.70%, p< 0.001) but not in expansion states (14.23% to 14.22%, p=0.94). Among dual-eligible patients, the DID model demonstrated that ME was associated with lower mortality in ME states (p=0.01). There was no association between ME and rates of amputation in the overall cohort or among dual-eligible patients with PAD.
Conclusion: Implementation of ME was associated with a decrease in mortality among dual-eligible patients with PAD. Policymakers in states without ME should consider the implication of these findings when making decision about expanding dual eligibility.
FEATURED ORIGINAL RESEARCH
Poster No. 17
Abstract ID No.1483253
The impact of CD73 immune checkpoint blockade on procoagulant tissue factor
Evan Garrad, BS1, Sumith Panicker, PhD2, Jaideep Moitra3, Yogen Kanthi, MD3
1University of Missouri – Columbia, 2National Institutes of Health, 3NIH, NHLBI
Background: Monocytes play a key role in initiating immune-mediated thrombosis through expression of tissue factor (TF) and release of TF-bearing extracellular vesicles. Extracellular adenosine is a key intravascular brake on the self-amplifying cycle of thromboinflammation following tissue injury. CD73, an immune checkpoint ectoapyrase, hydrolyzes the terminal phosphate group from extracellular AMP to generate adenosine. Genetic or post-natal inhibition of CD73 exacerbates venous and arterial thromboinflammation in animal models. Recent studies have also identified CD73 as an immune checkpoint on tumor cells, leading to many phase 2 clinical trials with CD73 inhibitors in patients already at high risk of thrombosis.
Methods: To assess the impact of CD73 inhibition on monocyte tissue factor expression, we incubated THP-1 monocytes and healthy hPBMCs with the CD73 inhibitor, adenosine 5'-(α, β-methylene) diphosphate (AMPCP). We then examined PBMCs and plasma from a cohort of patients with ultrarare, loss-of-function gene mutations that result in loss of CD73 (ACDC) and who present with premature peripheral artery calcific disease and occlusions.
Results: In a human monocytic cell line in vitro, CD73 inhibition increased surface tissue factor expression in a time-dependent manner (p=0.01). However, hPBMCs treated with CD73 inhibitor did not demonstrate changes in tissue factor expression at baseline or following cytotoxic challenge with LPS (p=0.17, p=0.98). In a pilot study comparing PBMCs from patients with ACDC (n=8) and healthy controls (n=6), surface tissue factor expression was similar between the groups at baseline and after LPS challenge (p=0.31). Correspondingly, analysis of plasma-derived extracellular vesicle tissue factor activity from ACDC and controls revealed no differences (p=0.145).
Conclusion: These findings suggest exogenous suppression or innate deficiency of CD73 does not increase monocyte tissue factor expression or extracellular vesicle tissue factor activity at baseline or following exposure to LPS. Together, these data provide insight into the molecular mediators of thromboinflammation and may inform thrombotic risk in patients with ACDC or patients with cancer receiving CD73 inhibitors.
FEATURED ORIGINAL RESEARCH
Poster No. 18
Abstract ID No.1486002
The depression phenotype of TIA: prospective associations between depression and cerebrovascular disease after TIA in a population cohort study
Stephanie Zawada, MS1, Onelia Zorio, DO2, Katelyn Marsden, MBBS2, Anthony Windebank, MD, MS1, Bart Demaerschalk, MD, MS2
1Mayo Clinic, 2Mayo Clinic Arizona
Background: Transient ischemic attack (TIA) patients are at a heightened risk of subsequent CeVD. An emerging body of literature suggests that depressive symptoms may be associated with an increased risk of cerebrovascular disease (CeVD)-related events; however, current evidence elucidating the role of depression in the development of CeVD after a TIA is lacking. We sought to investigate associations between depression and subsequent risk for CeVD in adult patients who previously suffered a TIA.
Methods: This retrospective, population cohort study examined data collected from 4,131 participants who suffered a TIA (mean age = 62.08 + 5.93, 56.9% male) before the initial UK Biobank assessment (2006-2010) and their primary care, hospital admissions, self-report, and death records through February 2023. Cox proportional hazards regression was used to identify prospective associations between baseline depression (PHQ-2 score > 2) and any category of CeVD diagnosis (ICD-10 F01, H34, G46, I60-I69).
Results: In TIA patients, baseline depression was associated with an increased risk of intracerebral hemorrhage (adjusted hazard ratio (aHR) = 4.632, 95% confidence interval (CI) = 1.981 to 10.831; p < 0.001), occlusion and stenosis of precerebral arteries (aHR = 2.736, 95% CI = 1.602 to 4.672; p < 0.001), and sequelae of CeVD (aHR = 1.544, 95% CI = 1.069 to 2.229; p < 0.020).
Conclusion: These findings suggest that depression may be a risk factor appropriate for screening TIA patients to identify those most at risk of intracerebral hemorrhage (I61), precerebral artery stenosis and occlusion (I65), and long-term disability (I69). More research is required to understand the plausible role of depression as an observable phenotype specific to emerging CeVD conditions after a TIA.
Poster No. 19
Abstract ID No.1503511
Association between an elevated D-dimer and the presence of acute to subacute deep venous thrombosis in the lower extremities of hospitalized COVID-19 patients in a tertiary hospital in Cebu city
Anthony Jay E. Alvez, MD, Florema Sy. Sy-Garcia, MD
Cebu Doctors University Hospital
Background: Thrombosis and coagulopathy are emerging clinical features of COVID-19. COVID-19-positive patients can present with hypercoagulability and higher susceptibility for deep venous thrombosis and is added to the already extensive list of conditions that may be associated with elevated D-dimer.
Methods: This is a retrospective, single-center cohort study of 104 records of COVID-19 patients with a baseline d-dimer level upon admission who underwent venous duplex ultrasound of the lower extremities.
Results: There is a significant relationship (p-value =0.005) with D-dimer levels and COVID-19 severity and a significant difference (p-value=0.039) between those with acute to subacute DVT in lower extremities and those who without DVT. The diagnostic accuracy measures of D-dimer as indicator of acute to subacute DVT yielded a sensitivity of 100%, a negative predictive value of 100% and specificity is 30.43%, a positive predictive value of 8.57%, likelihood ratio – positive of 1.44 with over-all accuracy of 34.69%.
Conclusion: Out of 104, 6 were diagnosed with acute to subacute deep venous thrombosis in the lower extremities. The higher levels of D-dimer are associated with higher COVID-19 severity. There is a significant difference between those diagnosed with acute to sub-acute DVT in lower extremities and those who weren’t in which those with DVT had significantly higher D-dimer levels over those who did not develop such condition.
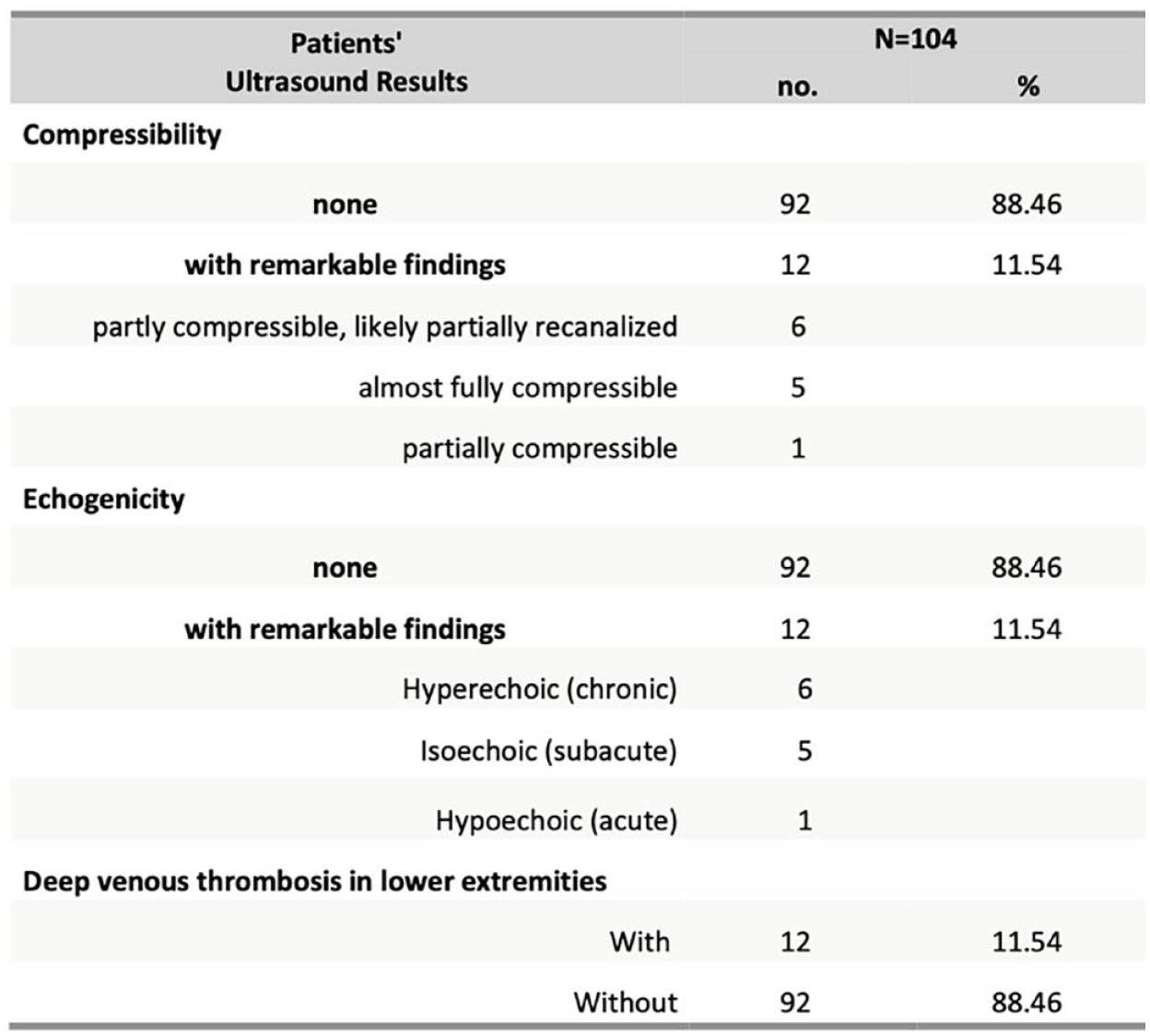
Venous duplex ultrasound of lower extremities of hospitalized COVID-19 patients.
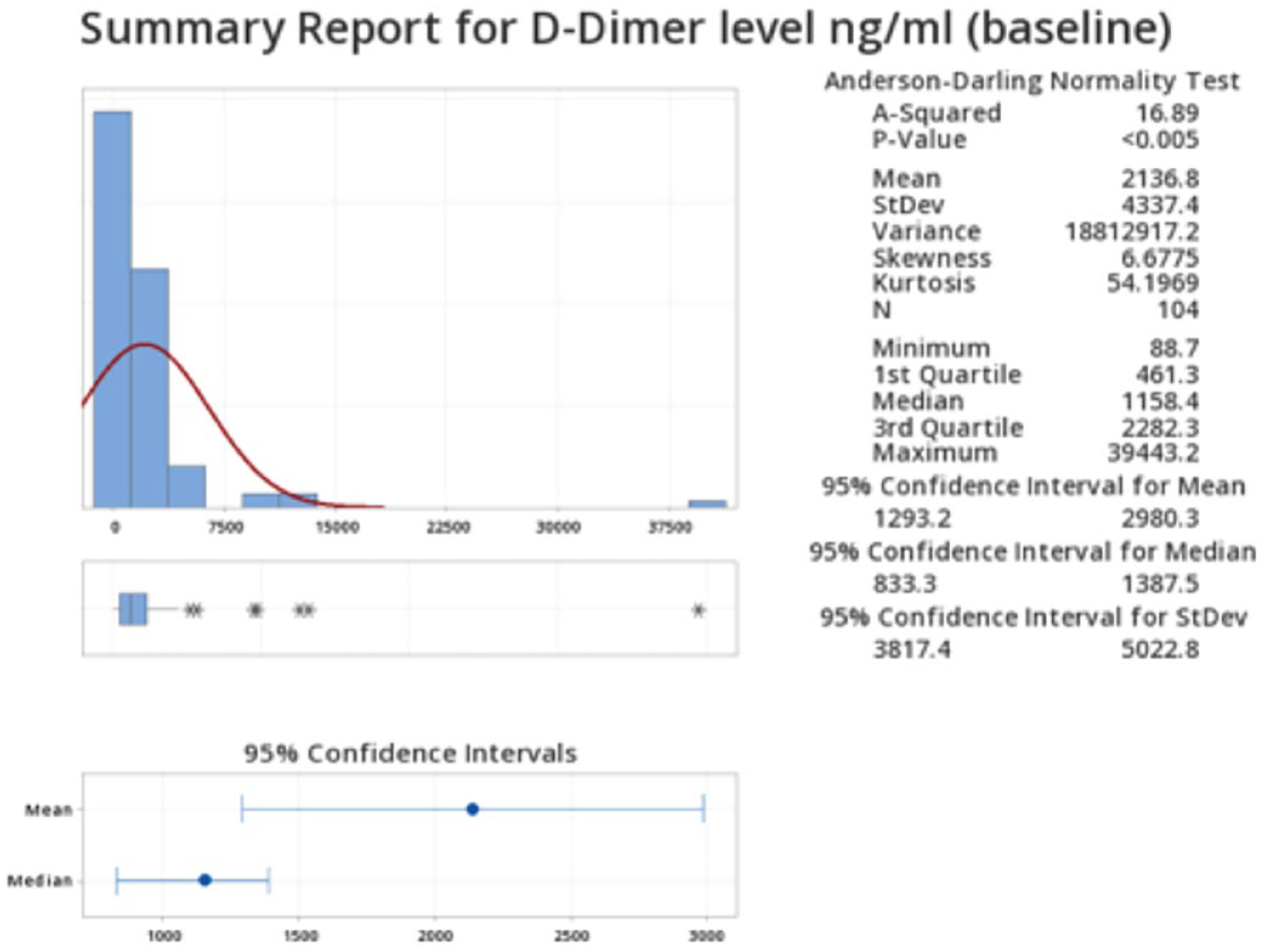
D-dimer levels of hospitalized COVID-19 patients.
Poster No. 20
Abstract ID No.1497021
Open surgical vs. endovascular repair of symptomatic above-knee peripheral arterial disease: is old still gold?
Samer Asmar, MD, Hussam Aridi, MD, Fouad Sakr, MD, Reem Dimachkie, MD, Zakaria Alameddine, MD, Rachelle Hamadi, MD, Jessica K. Bjorklund, MD, MPH, Mitchell D. Weinberg, MD
Staten Island University Hospital
Background: Peripheral arterial disease (PAD) remains an underdiagnosed cardiovascular disorder. Despite increasing use, the optimal revascularization strategy (open vs. endovascular) for patients with symptomatic PAD is still not established. Our study aims to compare outcomes and readmission rates of open vs. endovascular repair of symptomatic PAD.
Methods: The Nationwide Readmissions Database (2018) was queried for all adult (age ⩾ 18 y) patients presenting with above-knee PAD (common iliac, external iliac, internal iliac, and femoral arteries) who underwent isolated single vessel repair. Patients were stratified into 2 groups based on intervention: open vs. endovascular approach. Propensity score matching (1:1 ratio) was performed. Outcome measures included length of stay (LOS), 30-day readmission, complications, mortality, and hospital charges.
Results: Among 43,271 eligible patients, 18,652 underwent open repair and 24,619 underwent endovascular repair. The 18,652 open repair patients were matched to 18,652 endovascular repair patients. Patients undergoing endovascular repair had fewer in-patient complications including DVT (1.3 vs 2.3%, p< 0.001), seroma/hematoma formation (1.7 vs 1.4%, p=0.003), sepsis (1.6 vs 1.1%, p< 0.001), and compartment syndrome (1.2 vs 0.8%, p< 0.001). Hospital charges were lower with endovascular repair ($78,874 vs $112,206, p< 0.001) as was inpatient mortality (2.4 vs 1.8%, p=0.002). Patients with the open repair were more likely to be discharged to other rehabilitation facilities (24.2 vs 20.5%, p< 0.001) and more likely to be readmitted within 1 month (5.7 vs 5.1%, p=0.021). Furthermore, the 6-month readmission rate with new arterial thrombosis was lower with endovascular repair (23.8 vs 26.7%, p< 0.001).
Conclusion: Using population-based data, we demonstrated endovascular repair for PAD was associated with lower rates of in-hospital complications, readmissions, and costs. As this minimally invasive technique continues to develop, further evaluation of its indications, risks, and benefits is warranted.
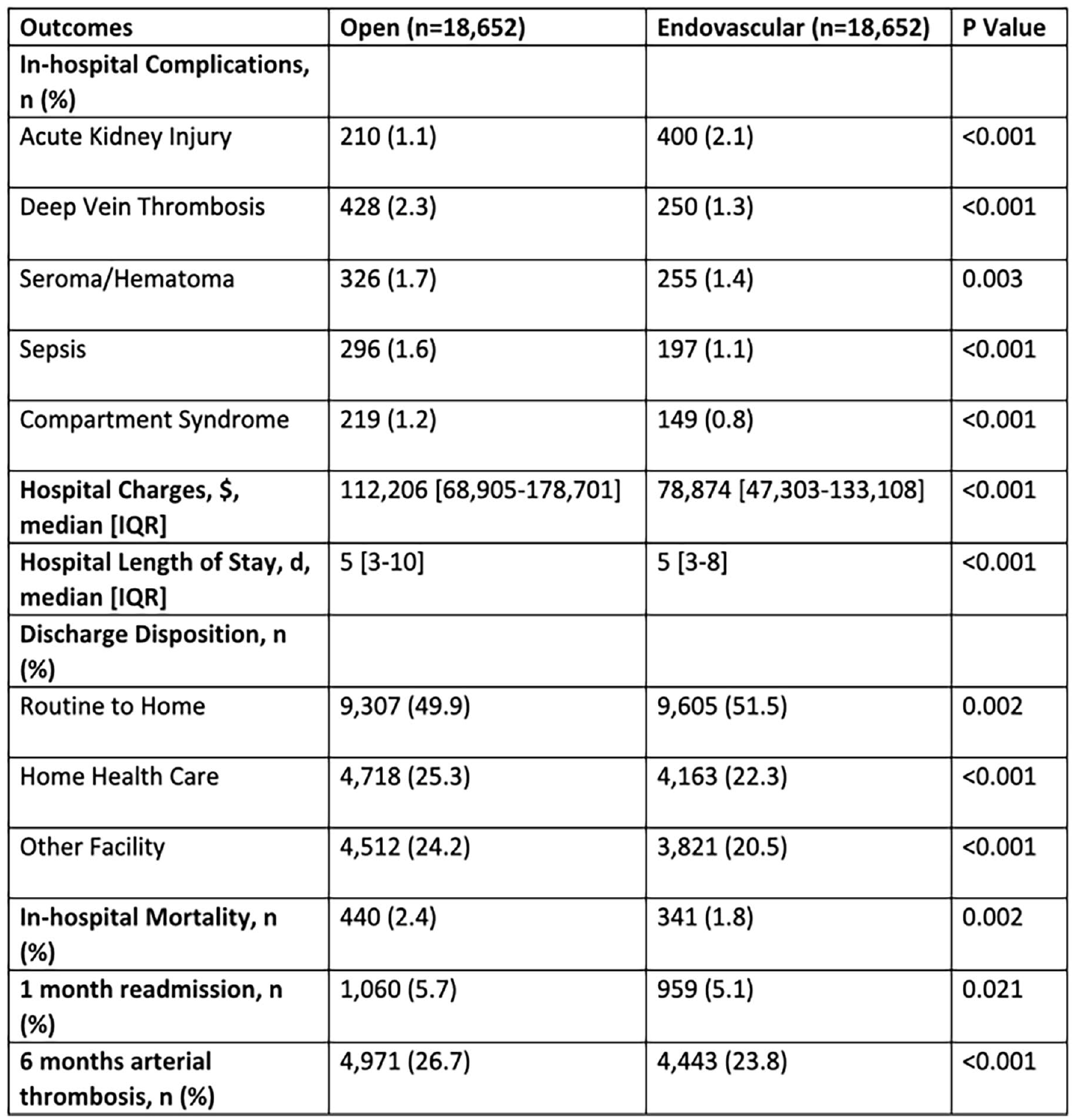
Outcomes of open surgical repair vs. endovascular repair of above-knee peripheral arterial disease.
Poster No. 21
Abstract ID No.1498470
Symptomatic below-knee peripheral arterial disease: does mode of intervention matter?
Samer Asmar, MD, Fouad Sakr, MD, Hussam Aridi, MD, Reem Dimachkie, MD, Rachelle Hamadi, MD, Zakaria Alameddine, MD, Jordyn Salak, MD, Jessica K. Bjorklund, MD, MPH, Mitchell D. Weinberg, MD
Staten Island University Hospital
Background: The optimal revascularization strategy for symptomatic lower extremity PAD is not well established. The 2016 American Heart Association/American College of Cardiology (AHA/ACC) guidelines on the management of patients with lower extremity PAD do not favor the use of surgical revascularization over endovascular revascularization for these patients.
Methods: The Nationwide Readmissions Database (2018) was queried for all adult (age ⩾ 18 y) patients presenting with below-knee PAD (popliteal, anterior tibial, posterior tibial, peroneal, and plantar arteries). Patients were stratified into 2 groups based on intervention: open vs endovascular approach. Propensity score matching (1:1 ratio) was performed. Outcomes measures were complications, length of stay (LOS), 30-day readmission, and hospital charges.
Results: Among 17,096 eligible patients, 1,992 underwent open repair and 15,104 underwent endovascular repair. The 1,992 open repair patients were matched to 1,992 endovascular repair patients. Patients undergoing endovascular repair had fewer in-patient complications including acute kidney injury (AKI) (10.5 vs 12.9%, p=0.021) and compartment syndrome (0.9 vs 2.2%, p< 0.001). There were no differences in rates of deep vein thrombosis (DVT) (2.0 vs 2.4%, p=0.383), seroma/hematoma formation (1.3 vs 1.5%, p=0.684), and sepsis (1.0 vs 1.0%, p=0.872) between the two groups. Hospital charges were lower with endovascular repair ($102,365 [64,576-166,126] vs $110,472 [61,817-189,413], p=0.025) as was hospital LOS (4 [2-6] vs 4 [3-7] days, p< 0.001). Patients with the open repair were more likely to be discharged to other rehabilitation facilities (32.5 vs 19.8%, p< 0.001) while those with the endovascular repair were more likely to be discharged home (58.2 vs 37.0%, p< 0.001). There was no difference between the endovascular and open interventions with respect to in-hospital mortality (p=0.069) and 1-month rehospitalization (p=0.427).
Conclusion: The use of endovascular repair for symptomatic below-knee PAD is associated with improved outcomes, lower hospital costs, and better discharge dispositions. Given that endovascular repair is a less invasive procedure, its role in managing PAD should be encouraged.
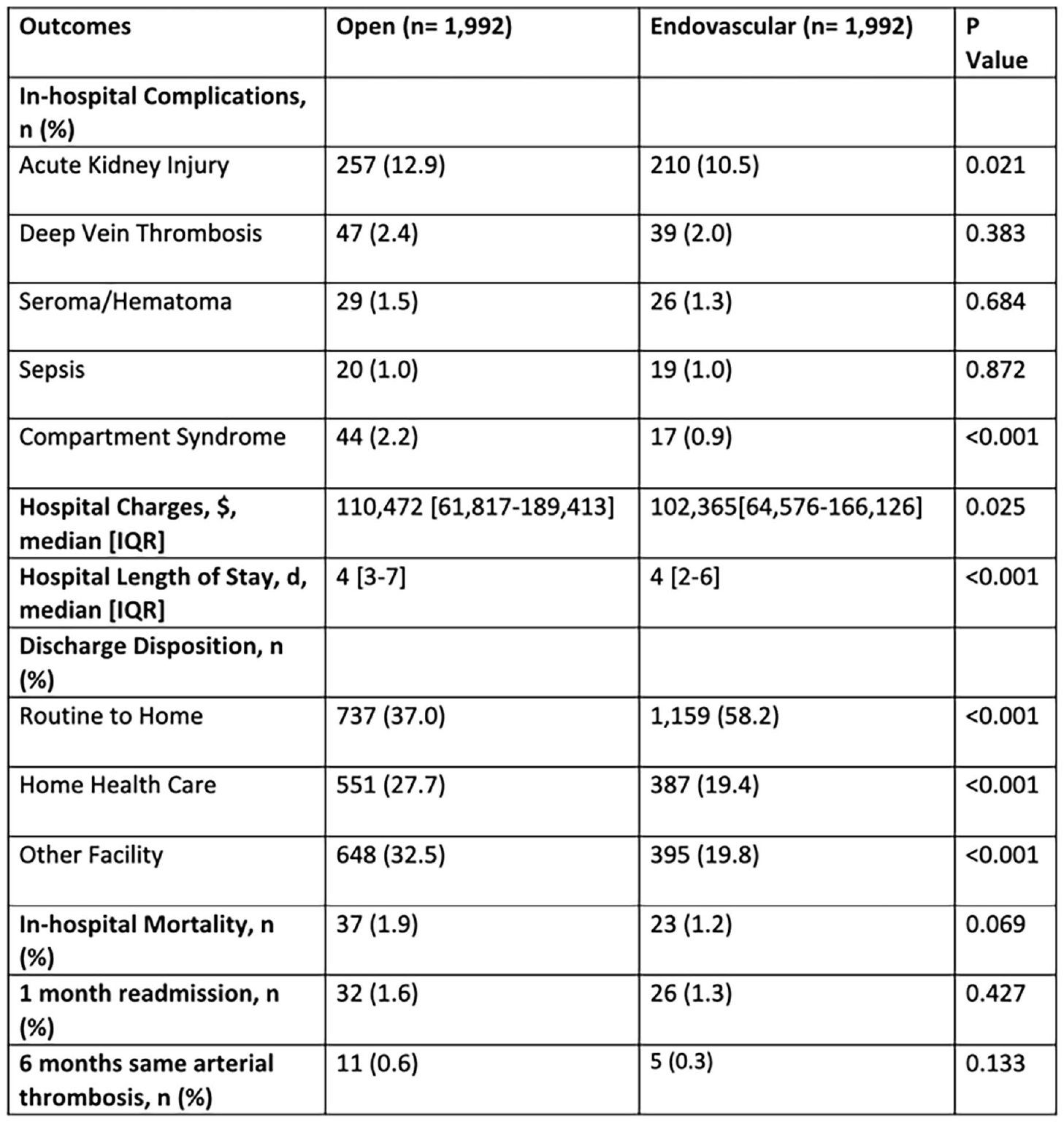
Outcomes of open surgical repair vs. endovascular repair of below-knee peripheral arterial disease.
Poster No. 22
Abstract ID No.1511286
Early observations on large language models for venous disease
Anand Athavale, MD1, Eri Fukaya, MD, PhD1, Jonathan Baier, BS2
1Stanford University, 2NextNext LLC.
Background: Large language models (LLM) and generative artificial intelligence such as ChatGPT have taken the world by storm, by its incredible ability to answer questions and provide feedback in instantaneous eloquent text. LLM can have many applications in medicine, but in its early days of use, how cautiously should we approach and recommend use to our patients? We hypothesize for well-defined questions asked in the correct context, LLM can produce excellent results. However, depending on how it is asked, it can give incorrect or nuanced responses which can be misleading.
Methods: We developed a question list for venous disease to be asked by different personas including a health care provider, patients with different education and language skills to the LLM. We analyzed how the same questions asked in different ways can produce answers and how same questions asked in different context can also produce different answers. We graded the answers as (1) appropriate and complete, (2) appropriate but incomplete, (3) neither right nor wrong, and (4) wrong.
Results: Preliminary results show that of 106 questions asked in both a professional and layman’s language, 86/106 (81%) were 1, 16/106 (15%) were 2, 4/106 (4%) were 3 and 0 were 4. The resources given for the provided answers were accurate, but the links were outdated. Although LLM gives a high rate of appropriate answers, this analysis provides guidance and shows where limitations may lie. For example, LLM can assert information too confidently or make recommendations without proper caveats or cautions. Given the fast-changing landscape of LLM capabilities, the output can be expected to rapidly change in a short period of time.
Conclusion: Although LLM is an elegant machine learning body that can give the persona of having the correct answers, LLM itself does not have the ability to “think” and there lie its limitations. Despite its limitations, the possibility for LLM to provide medical education to patients, caregivers, and healthcare providers is enormous thus continued consideration of how this can be used more effectively is necessary.
Poster No. 23
Abstract ID No.1501099
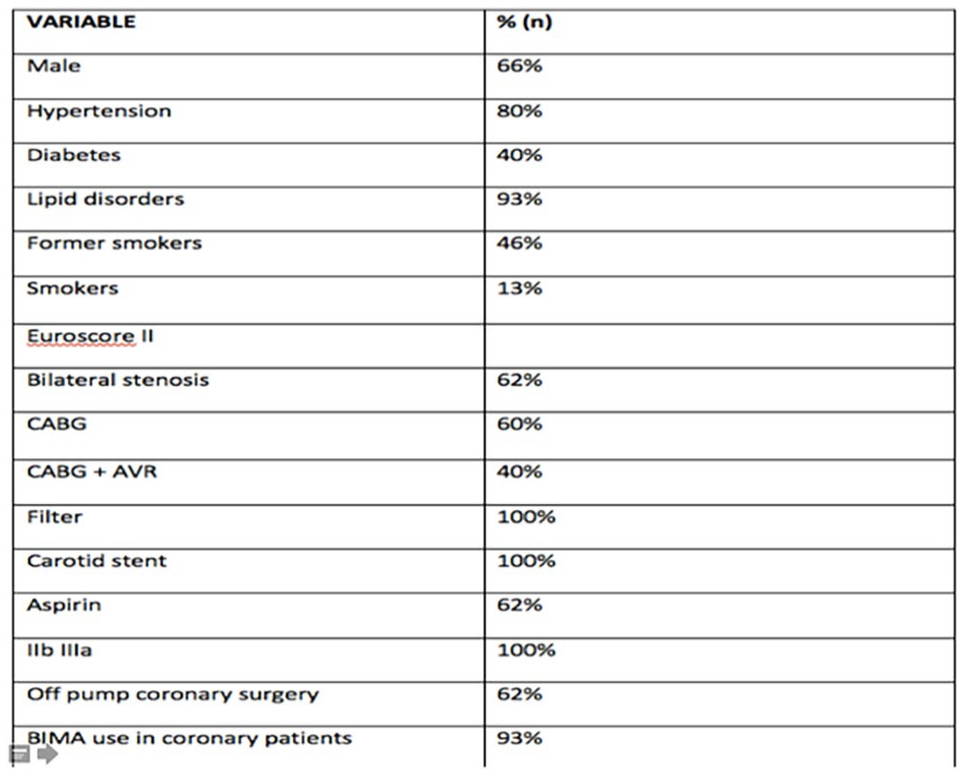
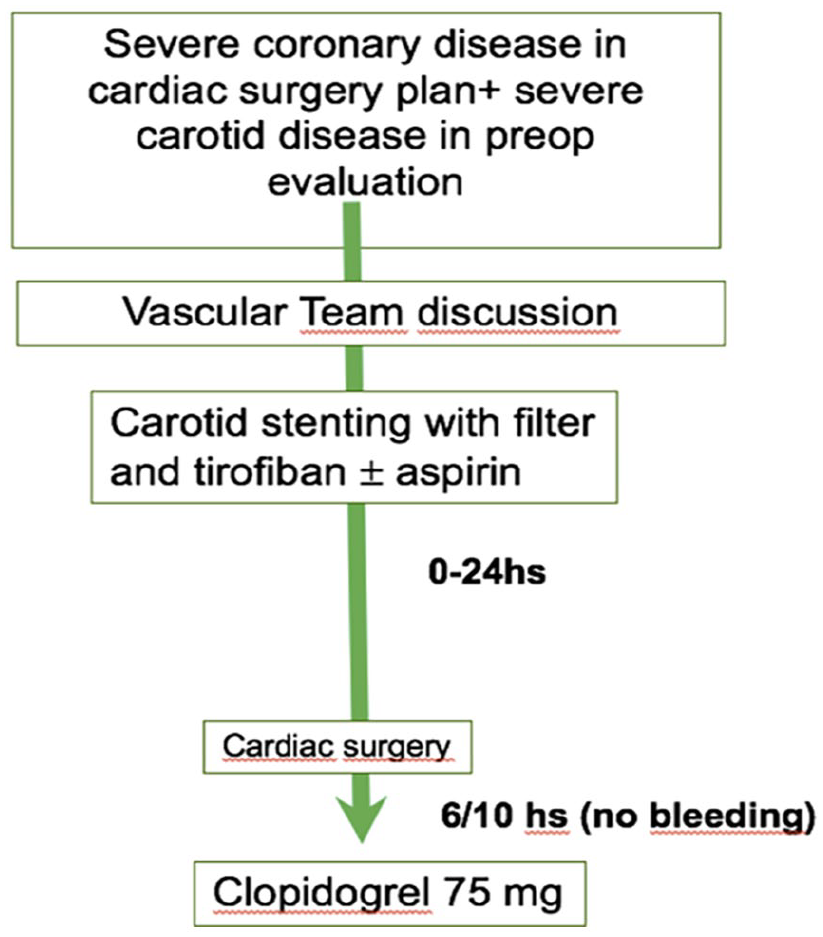
Hybrid one day strategy in patients with concomitant severe carotid and coronary or valve disease that required cardiac surgery
Fernando Belcastro, Pablo Elissamburu, Mariano Vrancic, Maria Esther Aris Cancela, Gustavo Pedernera, Sebastian Ghibaudo, MD, Maximiliano Villagra
Instituto Cardiovascular de Buenos Aires
Background: Background Optimal management of patients with internal carotid artery (ICA) stenosis concurrent with severe cardiac disease remains undefined. The aim of this study is to evaluate the safety and feasibility of the hybrid one-day, sequential approach by carotid artery stenting (CAS) followed by cardiac surgery in one center.
Methods: This is an observational and retrospective study from March 2014 until March 2021. All patients scheduled for cardiac surgery with associated carotid disease, with indication for carotid revascularization were selected. Patients with severe, symptomatic or asymptomatic carotid stenosis with rsk predictors and bilateral severe disease o unilateral carotid occlusion and severe for another side, were treated with carotid stenting after the anatomic and clinical evaluation. The carotid stenting was made in the cath lab with tirofiban and within the next 24 hs the cardiac surgery was performed.
Results: The study included 19 consecutive patients with severe ICA stenosis coexisting with severe coronary/valve disease in cardiac surgery plan. As we expected tha patient had high risk, all subjects had an increased surgical risk (EuroSCORE II 6.6 average). Sixty percent of the patients were men, as expected they had a high prevalence of risk factors, 80% were hypertensive, 40% diabetic, and more than half smoked or had smoked. With regard to the reason for cardiac surgery, 60% were coronary, using off-pump surgery in all sections and double mammary surgery in 93%, while in the rest it was combined (coronary plus valve surgery). From the carotid point of view, in 60% of cases the disease was bilateral and all patients had asymptomatic arotid stenosis (Table). Cerebral protection devices and stent were used in all patients. No neurologic complications occurred during the carotid stenting procedures or after cardiac surgery. The 30-day death rate was 5.2% (one cardiovascular death.
Conclusion: Patients with severe, concomitant carotid and cardiac disease require cautious assessment and a multidisciplinary approach. One-day, sequential CAS and cardiac surgery in this study was relatively safe and did not result in neurological complications.
Poster No. 24
Abstract ID No.1511519
In hospital outcomes and readmission rates of percutaneous carotid artery stenting in patients with morbid obesity: an insight from National Readmission Database
Olayiwola Bolaji, MD1, Olanrewaju K. Adabale, MD, MA2, Onyinye Ugoala, MD3, Faizal Oudraogo, MD1, Oriaifo Osejie, MD2, Edurance Evbayekha, MD4, Habeeb Sanni, MD5, Aurthur Dilibe, MD2, Rahman Olusoji, MD6
1University of Maryland Capital Region Center, 2East Carolina University, 3Texas Tech Amarillo, 4Saint Luke Hospital Missouri, 5Jamaica Hospital Medical Center, 6Harlem Hospital Center
Background: Carotid artery stenting is one of the most common vascular interventions in the United States. Studies have reported outcomes following this procedure; however, data regarding the outcomes of carotid artery stenting in morbidly obese patients is limited.
Methods: This retrospective study utilized data from the National Readmission Database from 2016 to 2020 to investigate the outcomes of carotid artery stenting among morbidly obese patients. The preadmission diagnosis of morbid obesity was defined based on BMI ⩾ 40. Coarsened Exact Matching (CEM) was applied to match groups based on baseline demographics, comorbidities, smoking history, median household income, size, and hospital teaching status to reduce confounding variables.
Results: Out of the 41,710 patients that had carotid artery stenting included in this study, 15% (6,334) of them were morbidly obese. In this subgroup, 88% (5,579) of patients were re-hospitalized. Of the readmitted patients, 56.1% (3132) of them were hypertensive, 29.7% (1658) had congestive heart failure, 40.2% (2241) had a stroke, 44.9% (2503) were diabetic, 17.9% (1001) had chronic kidney disease, 12.6% (705) had hypothyroidism, 17.5% (974) had coronary artery disease, and 4.25% (237) had peripheral vascular disease. The mortality rate between the morbidly obese patients compared to non-obese was 10.6% vs 13.6%. Multivariate logistic regression shows that morbid obesity and smoking are protective factors against in-hospital mortality (p < 0.0001) while age, hypertension, and diabetes mellitus increase the odds of in-hospital mortality (p < 0.001).
Conclusion: Morbid obesity has historically been linked to poor cardiovascular outcomes. However, this study further adds to the obesity paradox, where obesity is protective. Further studies are needed to elucidate this paradox.
Poster No. 25
Abstract ID No.1499748
Thirty days readmission rates and outcome in morbidly obese patients undergoing peripheral angioplasty and stenting for chronic lower extremity peripheral arterial diseases
Olanrewaju K. Adabale, MD, MA1, Olayiwola Bolaji, MD2, Faizal Oudraogo, MD2, Edurance Evbayekha, MD3, Ugochukwu Ebubechukwu, MD4, Osejie Oriafo, MD1, Habeeb Sanni, MD5, Aurthur Dilibe, MD1, Rahman Olusoji, MD6
1East Carolina University, 2University of Maryland Capital Region Medical Center2, 3Saint Luke Hospital Missuori, 4George's University School of Medicine, 5Jamaica Hospital Medical Center,6Harlem Hospital Center
Background: As an expanding field of cardiovascular intervention, there has been substantial data regarding peripheral angioplasty, stenting success, and complication rates. However, there is limited data on the thirty days readmission rates and underlying socio-economic determinants that affect the outcomes of this intervention among the morbidly obese demographic.
Methods: We queried the National Readmission Database from 2016 to 2020, using the validated International Classification of Diseases (10th Edition) for patients with a body mass index ⩾ 40 kg/m2 and a primary diagnosis of lower extremity peripheral arterial diseases (PAD). Exclusion criteria included patients with percutaneous intervention for coronary artery disease and valvular replacement/repair. We assessed the case fatality rate in index admission, readmission rate, etiologies of re-admission, sociodemographic and predictors of re-admission. All these outcomes were stratified by the index year of occurrence.
Results: About 12.9% (64,282) of patients with morbid obesity (497,165) who underwent peripheral angioplasty and stenting for chronic lower extremity PAD were readmitted within thirty days of discharge. The major reasons for readmissions were anemia (43.1%), hemodialysis (10.9%), periprocedural complications (4%), and liver disease (3.32%). With stratified Pearson’s chi-squared testing, hypertension (7.09, P = 0.001), sepsis (4.70, P = 0.03), deep vein thrombosis (6.22, P = 0.01), mortality (13.67, P = 0.0002), pulmonary embolism (4.86, P = 0.027), and diabetes mellitus (3.85, P = 0.049) were found to be significantly associated with increased risk of readmissions. The sex of the patient and type of admission [elective vs non-elective] showed no significant differences (P>0.05).
Conclusion: Our results show that morbid obesity is associated with critical complications that result in rehospitalization following revascularization procedures for chronic lower extremity PAD. Clinicians and prospective studies need to focus on and explore ways to prevent these common reasons for re-admission thirty days after revascularization.
Poster No. 26
Abstract ID No.1486174
Clinical characteristics and patient risk factors associated with acute deep venous thrombosis among COVID-19 patients in a tertiary hospital
Christopher P. Caras, PRC, Greggy A. Panga
St. Luke's Medical Center- Global City
Background: Characterize and identify risk factors in patients with deep venous thrombosis identified after admission for COVID-19.
Methods: All adult patients admitted from October 1, 2020 to October 31, 2021, underwent lower extremity venous duplex scan for DVT evaluation. Patients with positive COVID-19 test were divided into DVT and non-DVT group. An analytical cross-sectional study design was used to identify clinical characteristics and potential risk factors for DVT in patients with COVID-19 . Demographic, laboratories, treatment and clinical outcome were abstracted and analyzed
Results: There were 90 (19.3%) DVT among 466 hospitalized COVID- 19 patients. Those with DVT, 31.1% had PE vs 12.8% in non-DVT, 6.7% had COPD vs 2.9% in non-DVT and 8.9% had CKD vs 4.8% in non-DVT. . Severe and critical COVID-19 severity were significantly higher in DVT as compared to non-DVT. Among DVT, half were given Ceftriaxone vs 26.3% in non-DVT group. Among non- DVT, 11.7% were given Cefuroxime and 34.6% Pip-Tazo. Using multiple logistic regression analysis, the age, BMI and COVID severity were associated with DVT. There is a significant difference between the mean ICU admission and hospital stay among those with DVT and non-DVT group. The mean ICU days were longer in DVT (13.67±15.4 days) as compared to non-DVT (10.16± 11.65 days) with p-value of 0.017. The mean hospital days were longer in DVT (23. 7±19.4 days) as compared to non-DVT (19.66± 13.5 days) with p-value of 0.02 but there is no sufficient evidence to show that the 28-day mortality and in-hospital mortality were different between the DVT and non-DVT group.
Conclusion: This retrospective cohort study showed that the prevalence rate of acute DVT among COVID 19 positive patient who underwent VCT were 19.3%, suggesting it may be reasonable to screen COVID 19 patients for this potentially severe but treatable condition. Furthermore, with age, BMI and COVID severity to be significantly higher among DVT positive COVID 19 patients along with longer ICU and hospital stays, these findings highlight the need for intensive COVID 19 illness managements
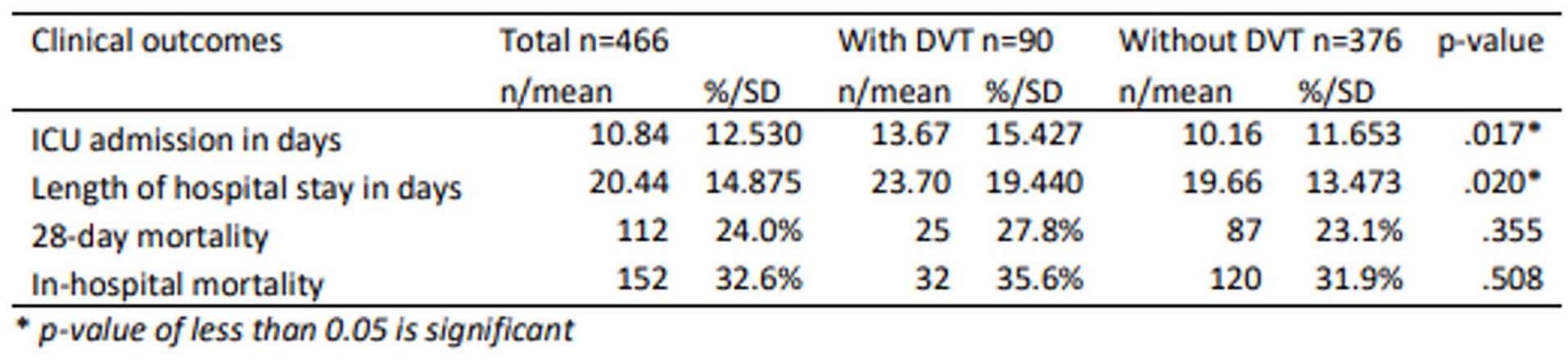
Clinical outcomes of those with DVT versus without DVT.
Poster No. 27
Abstract ID No.1511553
CaMKII antagonism improves endothelium-dependent vasomotor dysfunction in visceral adipose arterioles in human obesity
Bulbul Ahmed, PhD1, Melissa G. Farb, PhD1, Sophia D'Alessandro, BS1, Luise Pernar, MD1, Donald Hess, MD1, Brian Carmine, MD1, Kenneth Walsh, PhD2, Noyan Gokce, MD1
1Boston University School of Medicine, 2University of Virginia School of Medicine
Background: We have previously demonstrated increased activation of pro-inflammatory non-canonical WNT5a signaling in the visceral fat of obese humans that is associated with vasomotor dysfunction. Here, we sought to investigate the effect of WNT5a-CamKII in the regulation of vasodilation in adipose tissue arterioles susceptible to endothelial dysfunction.
Methods: In 10 human subjects with obesity (BMI 48±4 kg/m2, 38±6 years old), we isolated arterioles from visceral fat specimens obtained during planned bariatric surgery. We examined the effect of CamII antagonism on acetylcholine-mediated, endothelium-dependent vasodilation of arterioles using videomicroscopy in an organ bath ex vivo, and characterized vascular gene expression using real-time polymerase chain reaction.
Results: Pharmacological inhibition of calcium/calmodulin-dependent protein kinase II (CaMKII) with KN-93 improved endothelium-dependent dilation of vessels from visceral fat by three-fold (p< 0.01 compared to control). Inhibition of endothelial nitric oxide synthase with N(ω)-nitro-l-arginine methyl ester blunted KN-93-induced improvement in arteriolar vasodilation suggesting that reversal of vasomotor dysfunction is associated with increased nitric oxide bioavailability. Non-endothelium-dependent vasodilation to papaverine was not altered by KN-93 suggesting lack of a direct effect on vascular smooth muscle. Expression of mRNA transcripts relevant to Wnt-CamKII pathway were downregulated in arterioles treated with KN-93. Specifically, we observed decreased expression of JUN and NFAT5 (p< 0.05 for both), which are downstream of CamK and known to activate the inflammasome and augment proinflammatory cytokines IL6 and IL1β. No change in expression of Wnt5a or ROR2 were detected in vessels after treatment with KN-93 vs. control.
Conclusion: Collectively, these findings support the notion that CamKII signaling may negatively modulate microvascular function and partly contribute to the endothelial dysfunction observed in the vasculature of obese individuals.
Poster No. 28
Abstract ID No.1483141
Pilot study to evaluate etidronate treatment for arterial calcifications due to deficiency in CD73 (ACDC)
Elisa A. Ferrante, PhD1, Cornelia Cudrici1, Manfred Boehm1, Alessandra Brofferio1, Rebecca Huffstutler, CRNP1, Katherine Carney, RN, BSC, CCRC1, Marcus Y. Chen, MD2, Cynthia St Hilaire, PhD3, Carlos Ferreira, MD4
1NIH/NHLBI, 2National Institutes of Health, 3University of Pittsburg, 4NHGRI
Background: Arterial Calcifications due to Deficiency in CD73 (ACDC) is a rare genetic disease that results in calcium deposition within the lower extremity arteries and small joints of the hands/wrists, leading to claudication and pain at rest as well as severe joint pain and deformities. No standard treatments are currently available for ACDC. We have previously identified etidronate as a potential targeted treatment for ACDC in our work with in vitro and in vivo disease models with patient-derived cells. We designed a pilot clinical study to test the safety and effectiveness of etidronate in attenuating the progression of lower extremity arterial calcification and vascular blood flow based on CT calcium score and Ankle brachial index (ABI).
Methods: Seven adult patients with a confirmed genetic diagnosis of ACDC were enrolled in an open-label, non-randomized, single-arm pilot study for etidronate treatment. They took etidronate daily for 14 days every 3 months and were examined at the NIH Clinical Center bi-annually for 3 years as well as yearly baseline and follow-up visits before and after the treatment period. Study visits included imaging studies, exercise tolerance tests with ABIs, clinical blood and urine testing and full dental exams.
Results: Etidronate treatment appeared to have slowed the progression of further vascular calcification in lower extremities as measured by CT but did not have an effect in reversing vascular and/or periarticular joint calcifications in our small ACDC cohort.
Conclusion: Despite the small sample size, etidronate was found to be safe and well tolerated by our patients and appeared to show an effect in slowing the progression of calcification in our ACDC patient cohort, suggesting that it might be a useful treatment to prevent further disease progression in this patient population.
Poster No. 29
Abstract ID No.1470405
Utilizing soluble lectin-like low-density lipoprotein receptor-1 for estimating coronary plaque progression in psoriasis over 4-years follow-up: results from a prospective observational study
Elizabeth M. Florida, B.S1, Haiou Li, MS1, Christin G. Hong, BA1, Emily L. Ongstad, PhD2, Anna Collén, PhD2, Marcus Y. Chen, MD1, Alan T. Remaley, MD, PhD1, Alexander V. Sorokin, MD, PhD1
1National Institutes of Health, 2AstraZeneca
Background: Psoriasis is a chronic inflammatory condition associated with dyslipidemia and coronary artery disease (CAD). Excessive lipid oxidation results in high oxidized low-density lipoprotein (oxLDL) uptake by cellular lectin-like LDL receptor-1 (LOX-1) along with its soluble form (sLOX-1) released into the circulation.
Methods: Using an ELISA-based assay, we measured sLOX-1 in 327 psoriasis patients’ serum. Biochemical measurements were performed on a Cobas 6000 analyzer in the NIH Clinical Center (Bethesda, MD, USA). 81 subjects were identified by stratification of high sensitivity C-reactive protein (hsCRP) ⩾ 4.0 mg/L quartile (Q4) with coronary plaque phenotyping performed at baseline and longitudinally by coronary computed tomography angiography (CCTA). Statistical analyses were performed with StataIC 16 (TX, USA). Two-tailed P-values ⩽ 0.05 were deemed statistically significant.
Results: Participants in the hsCRP (Q4) cohort were middle-aged, predominantly male with moderate psoriasis disease severity. Those with sLOX-1 above median were characterized by increased CCTA vulnerable plaque features. At baseline, high sLOX-1 was significantly associated with total burden (rho=0.296; P=0.01), non-calcified burden (NCB) (rho=0.286; P=0.02), fibro-fatty burden (FFB) (rho=0.346; P=0.004) and necrotic burden (rho=0.394; P=0.002). A strong relationship between sLOX-1, NCB (β =0.39; P = 0.003) and FFB (β = 0.42; P = 0.001) was found in fully adjusted models at baseline, 1- and 4-year follow-up. Finally, in subjects with high sLOX-1 vulnerable coronary plaque characteristics progressed over 1 year regardless of biologic or systemic anti-psoriatic treatment.
Conclusion: Psoriasis patients with high sLOX-1 levels and elevated hsCRP demonstrate increased coronary plaque burden at baseline, which associate with plaque progression over time independent of biologic or systemic treatment. Thus, sLOX-1 represents a promising biomarker for estimating CAD risk in chronic inflammatory disease patients, including psoriasis.
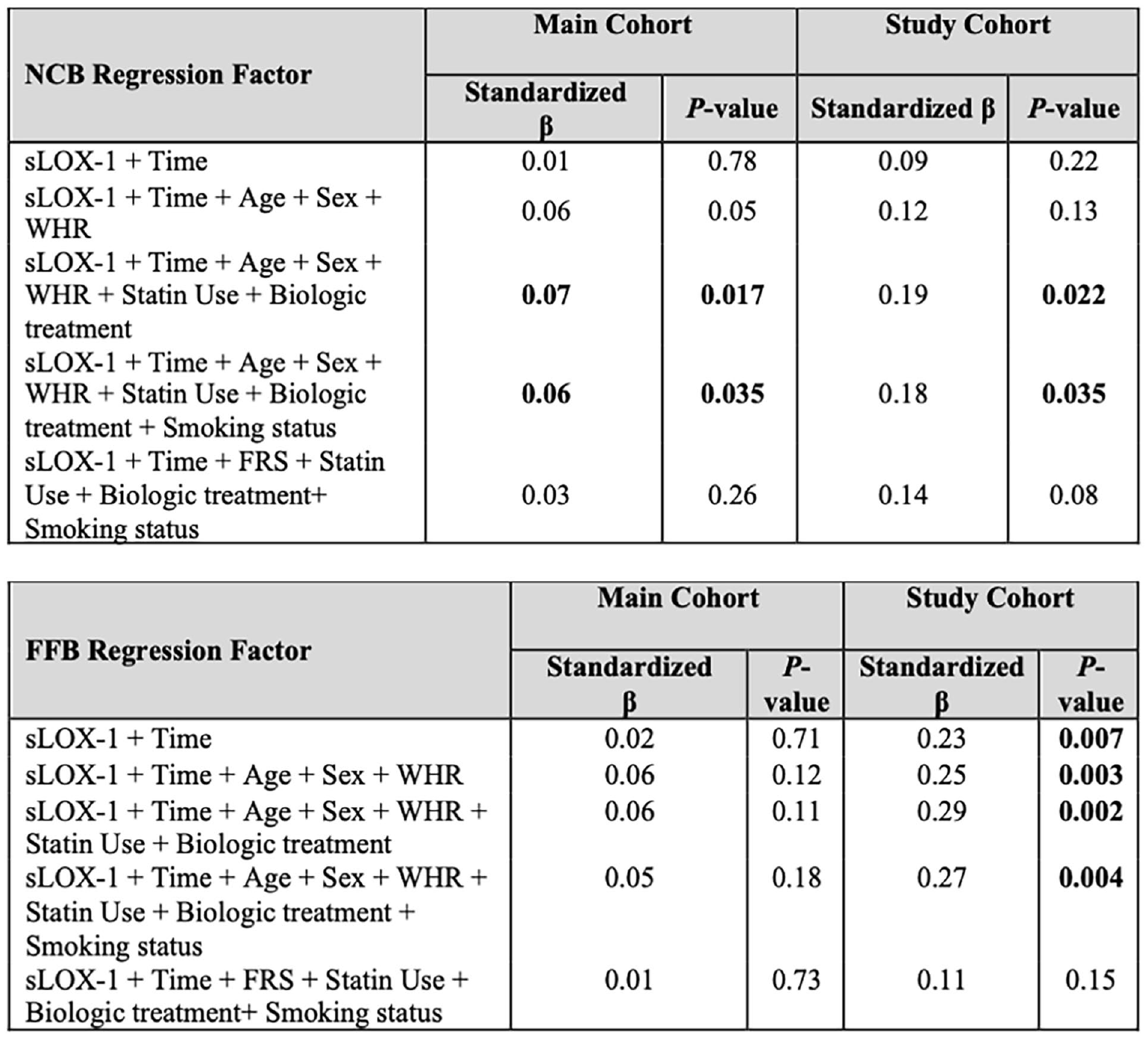
Longitudinal analysis of sLOX-1 with (A) non calcified burden and (B) fibrofatty burden at baseline, 1 year, and 4-years.
Poster No. 30
Abstract ID No.1511365
Psychological aspects in young people with thromboembolic disease, preliminary report
Alejandro Daniel Godoy, Noelle Bula Galli, MD, Aldo Tabares, MD
Hospital Privado Universitario de Cordoba
Background: The decline in the mental well-being of young adults following an episode of VTE may be related to the uncertainty of long-term health and fear of recurrence. In recent years, post-pulmonary embolism syndrome has gained acceptance, however, less attention has been given to the psychological impact of young patients after VTE. This study explores the prevalence, type, and severity of psychological disorders of patients following VTE.
Methods: An observational retrospective cohort study of patients aged ⩾ 18 years with VTE followed by the Vascular Medicine service at the Hospital Privado de Córdoba, Argentina from July 2020 to October 2021. Due to the Covid-19 pandemic, virtual interviews were conducted using two pre-established surveys administered by the same psychiatrist. The first survey gathered personal data, clinical history, and mental health information, while the second, evaluated mood disorders using the Mini International Neuropsychiatric Interview. Patients with a positive MINI score underwent further assessment with the Hamilton Scale. Patients were considered younger if ⩽ 45 years.
Results: A total of 50 patients were assessed, 56% were women, and 54% were ⩽ 45 years. Major depression was documented in 11 (22%) patients, 8 (72%) in the younger group, and 3 (28%) in the older group. Eight (16%) patients had an anxiety disorder, 4 younger group, and 10 (20%) patients had post-traumatic stress disorder (PTSD), 7(70%) of the younger patients. Generalized anxiety disorder was found in 20 (40%) patients with similar proportions in both groups
Conclusion: Following an episode of VTE, psychological and emotional symptoms are frequent. PTSD and depression appear to be numerically more prevalent in the young.
Poster No. 31
Abstract ID No.1497500
Identifying opportunities to expand implementation of the 2021 IAC recommended modified SRU consensus criteria for diagnosis of internal carotid artery stenosis: a survey of IAC accredited facilities
Marge Hutchisson, RVT1, Mary Beth Farrell, EdD, CNMT1, Nirvikar Dahiya, MD2, Michael Lilly, MD3, Laurence Needleman, MD4, Susana Robsion, MBA-HM, RVT, FASE5, John Pellerito, MD6, Tatjana Rundek, MD7, Heather L. Gornik, MD, MSVM8
1Intersocietal Accreditation Commission, 2Mayo Clinic Arizona, 3University of Maryland, 4Jefferson Health, 5Keck Hospital of University of Southern California, 6Northwell Health, 7University of Miami, 8University Hospitals Harrington Heart & Vascular Institute
Background: There is a lack of standardization of diagnostic criteria for internal carotid artery (ICA) stenosis. In 2021, a validation study of the SRU Consensus Criteria (SRUCC) proposed modification of velocity parameters for more accurate diagnosis of > 50% ICA stenosis. A subsequent statement by IAC Vascular Testing recommended that modified SRUCC be used in its accredited facilities. We sought to identify reasons why laboratories have not implemented the modified SRUCC.
Methods: Electronic email survey sent to 2,307 medical and technical directors of vascular laboratories accredited in extracranial carotid (EC) testing as of 12/2022. Analysis of data from respondents that reported not implementing the IAC recommended modified SRUCC.
Results: 574 respondents (24.9% response rate) representing 403 technical directors and 171 medical directors from 528 vascular laboratories. Among respondents familiar with the 2021 IAC recommendations, 60% (291/486) had implemented the modified SRUCC and 40% (195/496) had not. Respondents that had not implemented the modified SRUCC were less likely to be using the original SRUCC than those that had (28% vs. 44%). Primary reasons for not implementing the criteria are shown in the Figure and included need for more research, not having seen published research, and modified SRUCC criteria being too different from currently used criteria. Free text responses highlight multiple themes including: labs having internally validated their own criteria, no 80-99% ICA stenosis category in the modified SRUCC, yet to consider/discuss change among technical and medical leadership, and currently used criteria “working fine”. Among those respondents that had not implemented, 69% (120/173) were willing to do so in the future.
Conclusion: 40% of respondents from IAC accredited vascular laboratories familiar with IAC recommendations have not implemented the 2021 modification of the SRUCC. Among those not yet implementing, a majority were willing to consider doing so in the future. Need for more research, disseminating existing research, and organizational barriers are areas to target in future initiatives toward standardization of carotid diagnostic criteria in IAC accredited facilities.
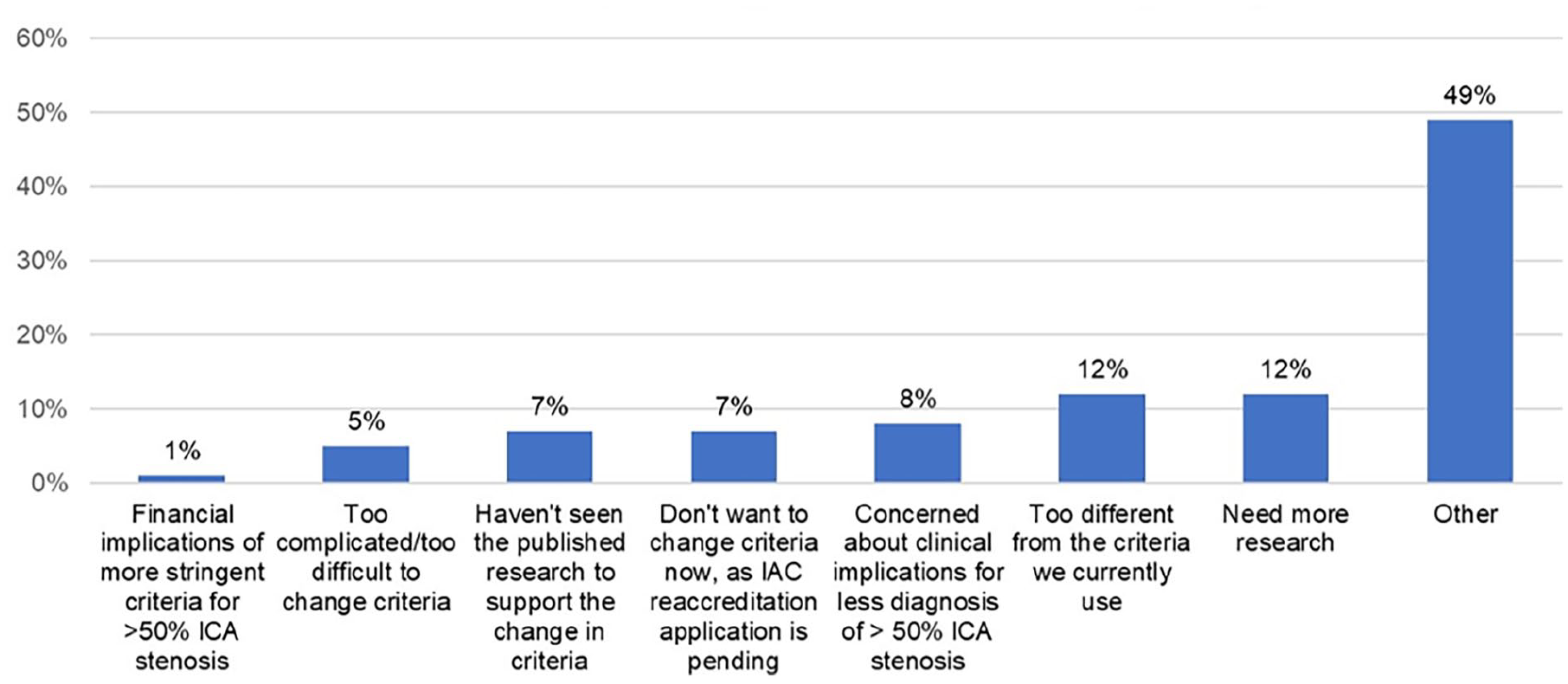
Reasons for not implementing modified SRUCC Criteria (n = 173).
Poster No. 32
Abstract ID No.1495605
Effectiveness of peripheral nerve blocks in opioid consumption and pain management after sclerotherapy of venous malformations
Aryaman Gupta, BSE, Anna Gong, BS, Robert Weinstein, BS, Prateek Gowda, BS, Clifford Weiss, MD
Johns Hopkins School of Medicine
Background: Venous malformations (VM) are the most common congenital venous anomalies with an estimated prevalence of 1% in general population. VM treatment includes surgery, laser therapy, sclerotherapy, or a combination. At our institution, an advanced anesthesia team is often asked to perform peripheral nerve blocks (PNBs) for post-procedural pain management associated with VM sclerotherapy.
Methods: In this IRB approved, retrospective study, patients who underwent sclerotherapy for VMs in the extremities between June 2016 - July 2022 were recruited. 86 patients who received a peripheral nerve block (PNB) and met inclusion criteria were included in the treatment group. Gender and age-matched (within 5 years) controls who did not receive a PNB were found for 83 of the study patients and included in analysis. The primary outcome was 24-hour, post-procedural total opioid consumption. The secondary outcomes were 24-hour, post-procedural non-opioid pain management and pain score 24-hours post-procedure.
Results: There was no statistically significant difference in gender proportion (p=0.79) or mean age at embolization (p=0.15) between the treatment and control groups. PNBs did not significantly reduce the proportion of patients receiving post-operative non-opioid pain management (p=0.25). However, PNBs did significantly reduce the proportion of patients receiving opioid pain management (p=0.0003). Additionally, the mean consumption of oxycodone during the 24-hour post-operative period was significantly lower in the PNB group (12.6mg vs 38.6mg, p=0.043). The average post-operative pain score (0-10 with 0 meaning no pain) was also significantly lower in the PNB group (1.59 vs 2.57, p=0.004). Of note, 27 patients (31%) in the PNB group and 12 patients (14%) in the control group had a history of chronic pain (p=0.01).
Conclusion: Peripheral nerve blocks are an effective post-operative pain management strategy prior to sclerotherapy of venous malformations. They are associated with reduced opioid prescription, decreased mean oxycodone consumption, and lower patient reported pain scores.
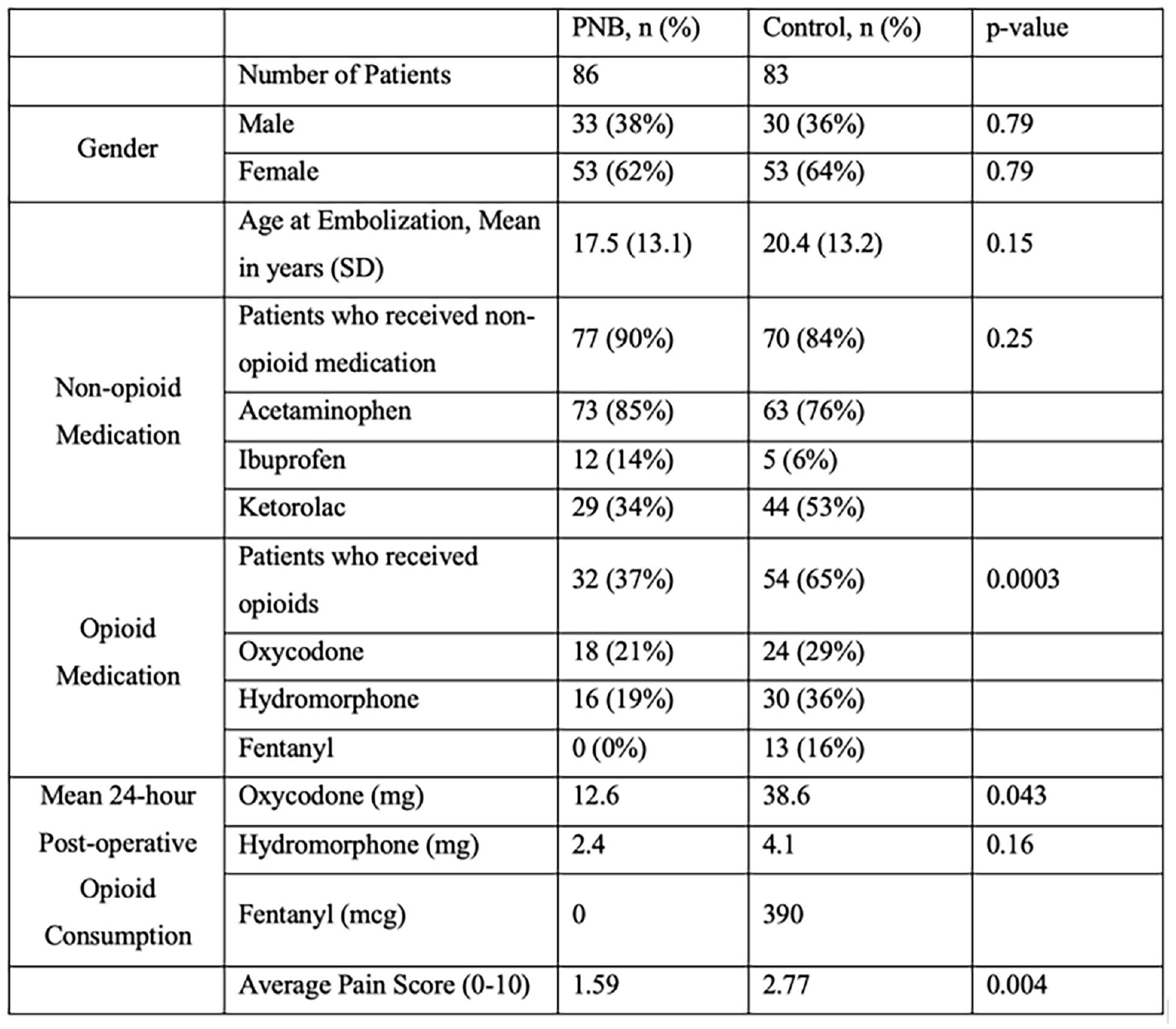
Poster No. 33
Abstract ID No.1498171
Associated pattern of the inflammatroy markers with severity of pulmonary embolism
Hatem Hassaballa, MD MPH1, Hesham Omar, MD2
1University of Wisconsin Health Hospital, 2Swedish American Hospital
Background: Inflammation is considered a risk factor for venous thromboembolism. However, the association between inflammatory markers and severity of acute pulmonary embolism (APE) has not been previously explored.
Methods: We studied the association between 2 crude markers of inflammation, serum albumin, and red cell distribution width (RDW), and massive versus non-massive APE in 552 consecutive cases of CT-angiogram-confirmed APE.
Results: A total of 46 cases (8.3%) had massive APE. Despite similar demographics and comorbidities, patients with massive APE had a higher frequency of acute kidney injury (P=0.005), higher lactic acid (P=0.011), troponin (P=0.001), and BNP (P< 0.001) levels, higher frequency of RV dilation (P=0.017), hypokinesis (P=0.003), and higher in-hospital mortality (15.2% vs. 2%, P< 0.001). Patients with massive APE had significantly lower albumin level [median (IQR): 2.8 (2.2, 3.0) vs. 3.2 (2.8, 3.6) gm/dL, P< 0.001] and higher RDW [median (IQR): 14.7 (13.8, 17.1) vs. 14.2 (13.3, 15.6), P=0.006] compared with non-massive APE. ROC curves showed that albumin and RDW had an AUC of 0.750 (P< 0.001) and 0.621 (P=0.006) in predicting a massive APE, respectively (Figure). The optimal cutoff values for albumin and RDW that had the highest combined sensitivity and specificity for predicting APE was ⩽3 gm/dL and >14, respectively. Restricted cubic splines showed a significant association between albumin (P=0.0002) and RDW (P=0.0446) and the occurrence of massive APE. After adjustment for patients’ age, body mass index, white blood cell count, requirement of antibiotics during hospitalization, diabetes and RDW, peak creatinine, serum albumin was independently associated with massive APE (OR 0.234, 95% CI 0.129- 0.4242, P< 0.001) (Table).
Conclusion: low serum albumin is a marker of massive APE risk. The association is likely a proxy for a higher inflammatory state in massive compared with non-massive APE.
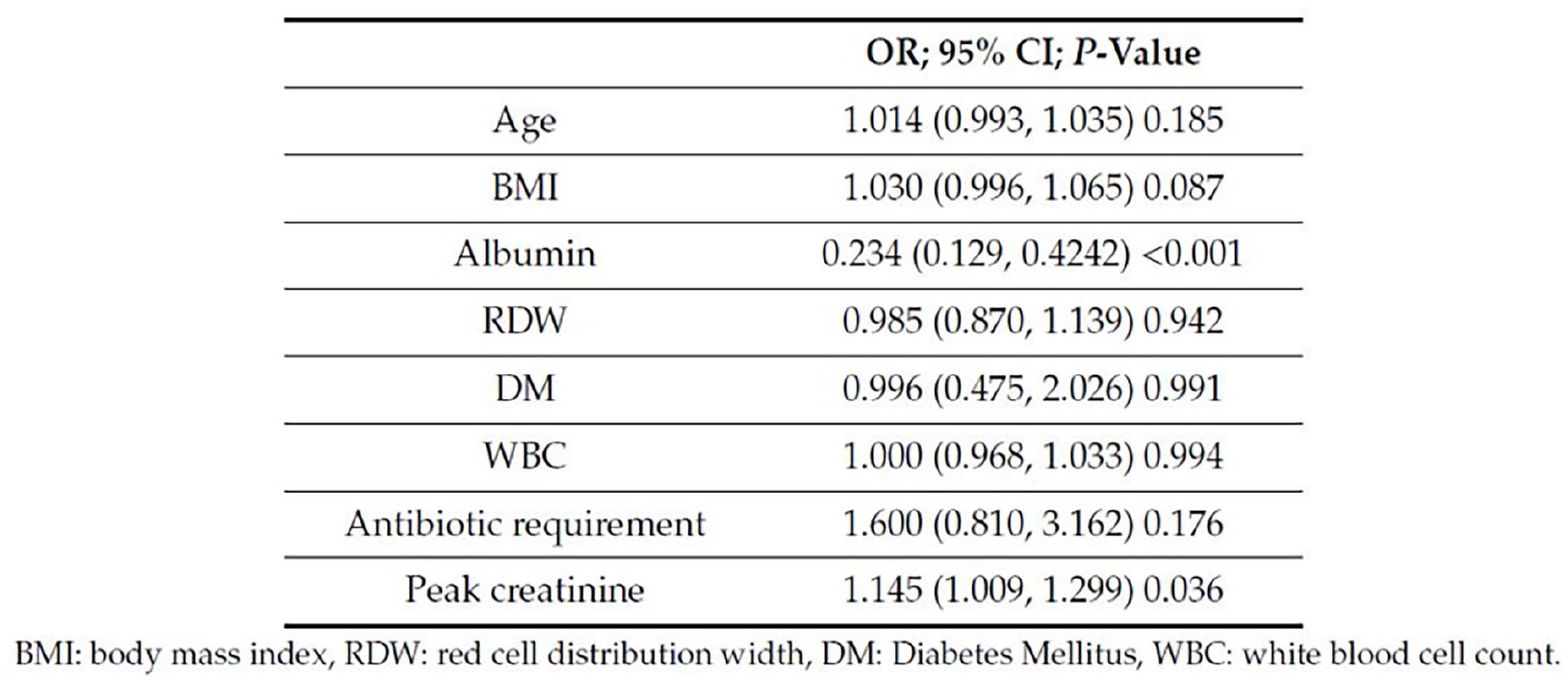
Multivariate analysis of determinants of massive acute pulmonary embolism.
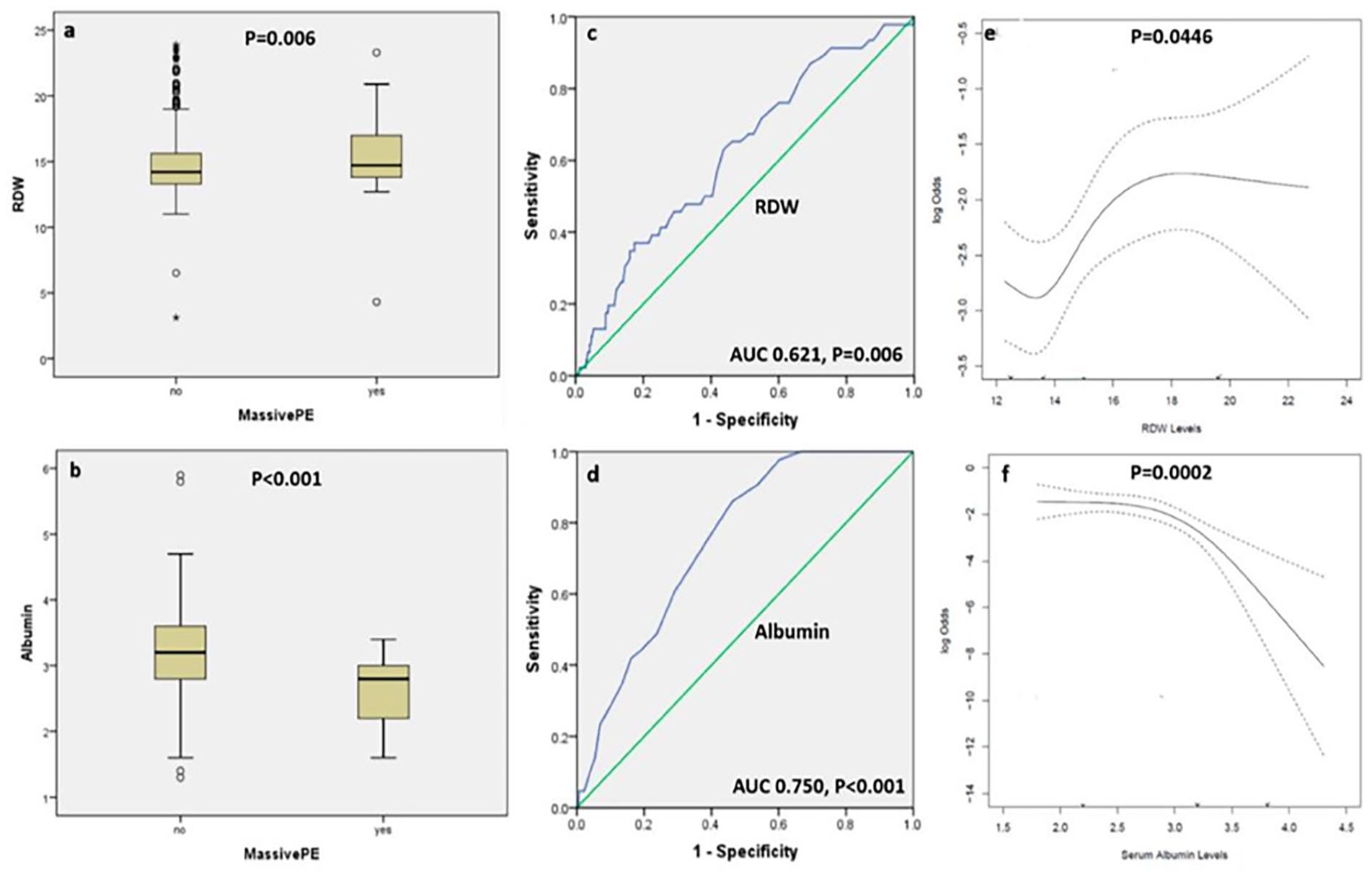
Box and whisker plots showing the level of red cell distribution width (panel a) and albumin (panel b) among patients with massive versus non-massive acute pulmonary embolism.
Poster No. 34
Abstract ID No.1499600
Bioengineering: infrarenal aortic stent graft explantation device
Solyman Hatami, BE1, Alwin Mathew, BS1, Vamsi Maturi, BS1, Shannon Lu, BS1, Nicholas Sears, PhD1, Maham Rahimi, MD, PhD2
1Texas A&M School of Engineering Medicine, 2Houston Methodist Hospital
Background: EVAR graft failure could be as high as 16-30% via endoleak, graft migration, and infection, necessitating endograft explantation. This leads to potential morbidity (31%) and mortality (6.3%). The current standard of care involves techniques such as the syringe technique which uses a cylinder created by cutting a syringe in half. There is currently no off-the-shelf technology for safe endograft explantation.
Methods: The needs exploration was performed through stakeholder interviews and analyzing different techniques used for endograft removal; design criteria were developed after addressing inefficiencies. The materials used to create different prototypes include plastic filaments, steel rods, and ball bearings. The prototyping process involved exploring mechanisms for explantation and iterative design. After identifying the top prototype, additional features were incorporated to address failure points and ergonomics. Benchtop testing was performed in 25mm and 30mm diameter silicone tubing to simulate the aorta and Cook Medical vascular endografts.
Results: Testing criteria included procedure time, reproducibility, and ease of removal. Surgeon feedback in simulations provided guidance for modifications and optimization. A major design criterion was the reduction of the diameter of the graft prior to explantation, the best prototype reducing the diameter from 25mm to 7mm. This device uses a tapered geometry that encloses the hooks when the device advances up the graft. To prevent endothelial damage, metal balls were added at the apex to reduce shear stress. To increase usability, a hinge mechanism was developed, allowing for closure around the graft while avoiding complications from the metal struts. Benchtop experiments validated feasibility and safety.
Conclusion: Our study has shown that the current standard of care is inefficient in multiple steps, necessitating novel off-the-shelf technology. We described the biodesign process for a technology improving endograft explantation. Our prototype indicated feasibility in use and effectiveness. The device is currently protected under a provisional patent. Our future work will involve continual improvement with testing in cadaveric and animal models.
Poster No. 35
Abstract ID No.1514703
A structured quality assurance program reduces six-minute walk test variability: insights from the OPTIMIZE PAD-1 trial
Connie Hess, MD, MHS1, Victoria Anderson, MPH2, Mark Nehler, MD1, Michael Szaerk, PhD2, Christopher Cannon, MD3, Judith Hsia, MD1, Marc Bonaca, MD, MPH1
1University of Colorado School of Medicine, 2CPC Clinical Research, 3Harvard Medical School
Background: Patients with peripheral artery disease (PAD) have impaired walking capacity and function. The 6-minute walk test (6MWT) is an important functional assessment, but variability in results may limit its utility and interpretation.
Methods: The randomized OPTIMIZE PAD-1 trial showed that a multidisciplinary vascular care team using an intensive lipid reduction program reduced cholesterol levels more than usual care in patients with vascular disease, including PAD. Patients in OPTIMIZE PAD-1 were also randomly assigned to undergo 6MWT conducted by a structured quality assurance program (EQuIP) or the site. Due to COVID-19, all 6MWT were performed virtually. Variability in 6MWT, a co-primary endpoint, was assessed using the Levene’s test.
Results: A total of 60 participating subjects were randomized to 6MWT administered by EQuIP (n=31) or the site (n=29). Baseline 6MWT data are shown in the Figure. The distance walked was longer among patients randomized to site (median 252.0 meters, IQR 180.0-428.0; mean 307.7 meters, standard deviation (SD) 201.4) than among those randomized to EQuIP (median 240.8, IQR 216.9-307.0; mean 255.6 meters, SD 79.1). Variability in 6MWT was significantly greater when conducted by the site than when administered by EQuIP (p=0.006).
Conclusion: In patients with vascular disease, including PAD, site administration of the 6MWT may
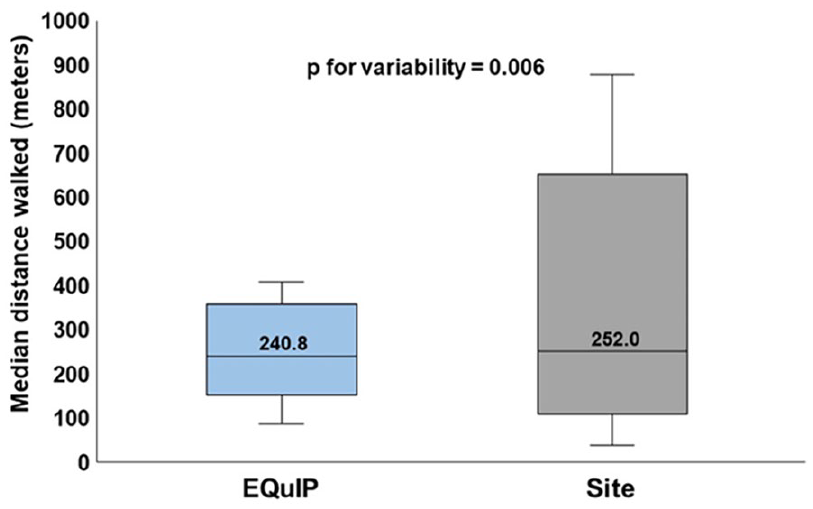
Impact of a structured quality assurance program on reducing variability in six-minute walk test.
Poster No. 36
Abstract ID No.1515483
Combination therapy lipid management in peripheral artery disease: insights from the OPTIMIZE PAD-1 trial
Connie Hess, MD, MHS1, Ashley Dafrron, PharmD2, Mark Nehler, MD1, Justin Morrison, MD1, Cullen Buchanan, MD3, Joseph Saseen, PharmD2, Christopher Cannon, MD4, Judith Hsia, MD1, Marc Bonaca, MD, MPH1
1University of Colorado School of Medicine, 2University of Colorado School of Pharmacy, 3Medical College of Wisconsin, 4Harvard Medical School
Background: Reducing low-density lipoprotein cholesterol (LDL-C) decreases ischemic risk in patients with peripheral artery disease (PAD). The OPTIMIZE PAD-1 trial demonstrated the effectiveness of multidisciplinary, algorithm-based care in reducing LDL-C in vascular patients. Recently presented data highlight the importance of combination therapy in achieving LDL-C goals. We therefore examined use of combination therapy in OPTIMIZE PAD-1.
Methods: OPTIMIZE PAD-1 randomized patients with vascular disease cared for at a tertiary referral center with an LDL-C >70 mg/dl to lipid management via an interprofessional vascular care team using an intensive lipid reduction algorithm versus usual care supplemented with provider education. Use of combination lipid lowering therapy, a prespecified outcome, was defined as treatment with ⩾2 of the following medications: statin, ezetimibe, or PCSK9 inhibitor. Combination therapy use was examined at baseline, 6 months, and 12 months overall and according to treatment assignment.
Results: A total of 114 patients were randomized in OPTIMIZE PAD-1 (median age 65 years, 36% female, 16% Black). All patients had vascular disease including lower extremity PAD (77%), cerebrovascular disease (19%), or other arterial vascular disease (30%); 35% of patients had polyvascular involvement with coronary artery disease. At baseline, 69% were on statin (52% high intensity), 8% were on ezetimibe, and 1.8% were on combination therapy. As shown in the Figure, use of combination therapy among patients assigned to usual care was low and did not change throughout the study (3.5% at baseline and throughout follow up). In the vascular care team group, use of combination therapy increased from 0% at baseline to 62.3% at 6 months and 12 months and was significantly greater compared with usual care.
Conclusion: Among patients enrolled in OPTIMIZE PAD-1, baseline use of combination lipid lowering therapy was low overall. Interprofessional, algorithm-based care was associated with significantly greater utilization of combination therapy, and this greater use persisted throughout follow up.
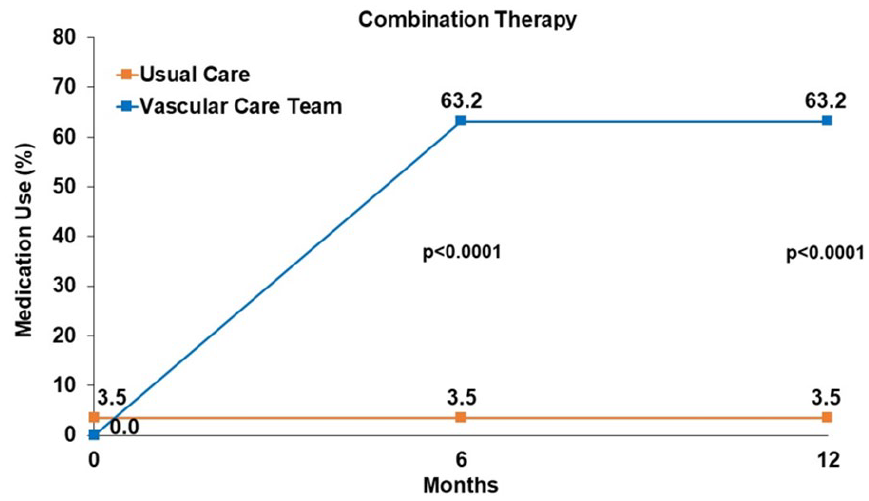
Temporal trend in combination therapy lipid management in the OPTIMIZE PAD-1 trial.
Poster No. 37
Abstract ID No.1497296
Prevalence and factors of venous thromboembolism among COVID-19 patients in a tertiary private hospital in the Philippines
Jonathan Moses C. Jadloc, Jose Bernardo Calatrava
St Luke's Medical Center, QC, Dr HB Calleja Heart and Vascular Institute
Background: COVID-19’s systemic activation of blood coagulation and pulmonary thrombi-inflammation with local vascular damage may increase the risk of venous thromboembolism (VTE) and pulmonary artery thrombosis and subsequent death
Methods: A retrospective, analytical, and cross-sectional study of adult patients (18yo and above) admitted for moderate, severe, (or critical), COVID 19 at St. Luke’s Medical Center Quezon, Philippines from April 2020 to December 2021. The outcomes of interest were prevalence of VTE, mortality and factors associated with VTE or mortality.
Results: With 216 patients, the prevalence was 10.65 and 12.04 for DVT and PE respectively. There were significantly more patients with BMI of 25 kg/m2 or higher (p < .001) and proportion of patients with severe (25.53% vs 25.44%, p = .023) and critical (46.81% vs 27.22%, p = .023) COVID-19 among those with VTE. Those with VTE had higher values for WBC (p < .001), neutrophil (p < .001), NLR (p < .001) and D-dimer (p = .002). Most of the patients had received anticoagulants (72.7%). Among VTE patients, the case fatality rate was 53.19% (95% CI 38.08% to 67.89%), for DVT it was at 39.13% (95 CI% 19.71% to 61.46%) and for PE it was at 65.38% (95% CI 44.33% to 82.79%). Other factors found to be significant are critical COVID-19 status, hemoglobin level, and hospital biological treatment. With VTE, patients were 7.5 times more likely to die (aOR = 7.55; p < 0.001). Those with critical COVID-19 status are 18 times as likely to die compared to moderate COVID-19 status (aOR 17.91, 95% CI 4.46-71.95, p < 0.001). For patients who had required biological treatment, they were about 6 times as likely to die (aOR 5.71, 95% CI 1.39-23.50, p = 0.016), however, for every unit increase in hemoglobin, the adjusted odds of dying is approximately 56% less, (aOR 0.66, 95% CI 0.52-0.85, p = 0.001).
Conclusion: The prevalence for DVT was 10.65 and 12.04 for PE. The case fatality rate for VTE was more than half, higher for PE than DVT. Key predictors of venous thromboembolism (VTE) included BMI >25 kg/m2 or higher, severe or critical covid, higher WBC, neutrophils, NLR, and D-dimer levels. Critical covid-19 status and use of biological treatments increased the odds of dying while the increase in hemoglobin level was protective.
Poster No. 38
Abstract ID No.1492131
JAK2V617F prevalence study: associations in the general population and vascular disease populations
Hannah Kaizer, MD1, Rakhi Naik, MD2, Katie Lobner, MLIS3, Shruti Chaturvedi, MD2, Elizabeth Ratchford, MD4, Michael Streiff, MD2, Alison Moliterno, MD2
1Johns Hopkins Sidney Kimmel Comprehensive Cancer Center, 2Johns Hopkins Hospital, 3Johns Hopkins University Welch Medical Library, 4Johns Hopkins School of Medicine
Background: JAK2V617F is not only the most common mutation associated with myeloproliferative neoplasms (MPN), it is the fifth most common lesion in clonal hematopoiesis (CH), which is defined as an expansion of blood stem cell clones that bear advantageous somatic mutations. JAK2V617F CH carriers, similar to MPN patients, are at increased risk of developing arterial and venous thromboses. While many large-scale general population studies have examined prevalence of JAK2V617F CH, a comprehensive assessment of associations to vascular disease phenotypes has not been performed.
Methods: We identified all published studies that evaluated the prevalence of the JAK2V617F mutation in the general population and in vascular disease cohorts of at least 40 subjects.
Results: 3776 studies met our initial search criteria and 105 eligible were included in the final meta-analysis (Figure). Fourteen studies examined the prevalence of JAK2V617F in unselected populations. Among 644,195 participants, 1,850 (0.29%) were positive for the JAK2V617F mutation. In all studies where vascular disease was also ascertained, JAK2 CH was an independent risk factor for either MI or venous thrombosis. Ninety-one studies examined the prevalence of JAK2V617F in patients with venous or arterial vasculopathy, 26,279 of which had a history of thrombotic disease and 8,944 controls. Among these individuals with vascular disease, 1,279 (4.9%) were positive for the JAK2V617F mutation. Those with splanchnic vein thrombosis had the highest prevalence (18.7%) followed by patients with ischemic stroke (8.5%) and cerebral vein thrombosis (6.0%) (Table). The prevalence of the JAK2V617F mutation in patients with DVT/PE and peripheral artery disease (PAD) was 1.6% and 3.1% respectively. The prevalence of JAK2V617F among vascular disease subsets was substantially higher than the control populations.
Conclusion: The JAK2V617F mutation is associated with alterations of blood counts and increased thrombosis risk. Even at very low variant allele frequency (VAF), JAK2V617F is a thrombosis risk factor in the general population and is over-represented in populations with thrombosis.
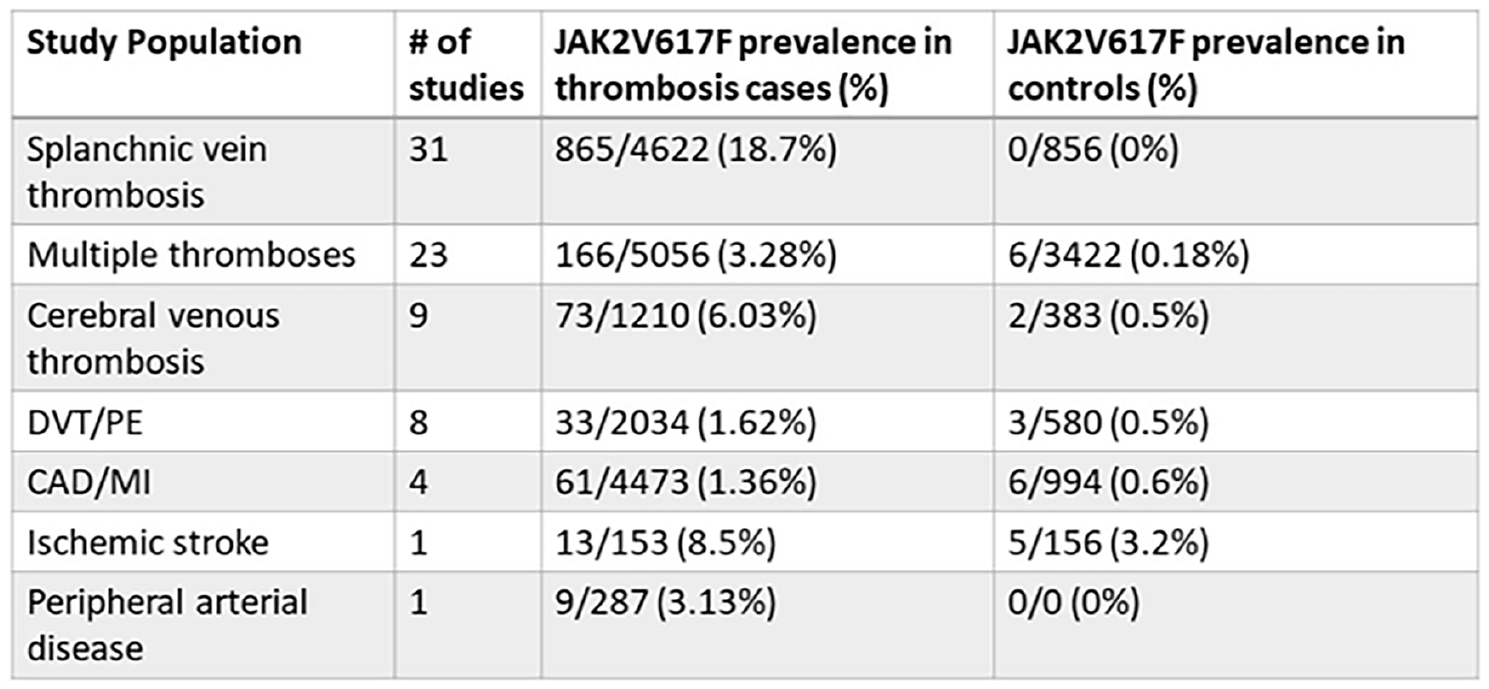
JAK2V617F in thrombosis groups.
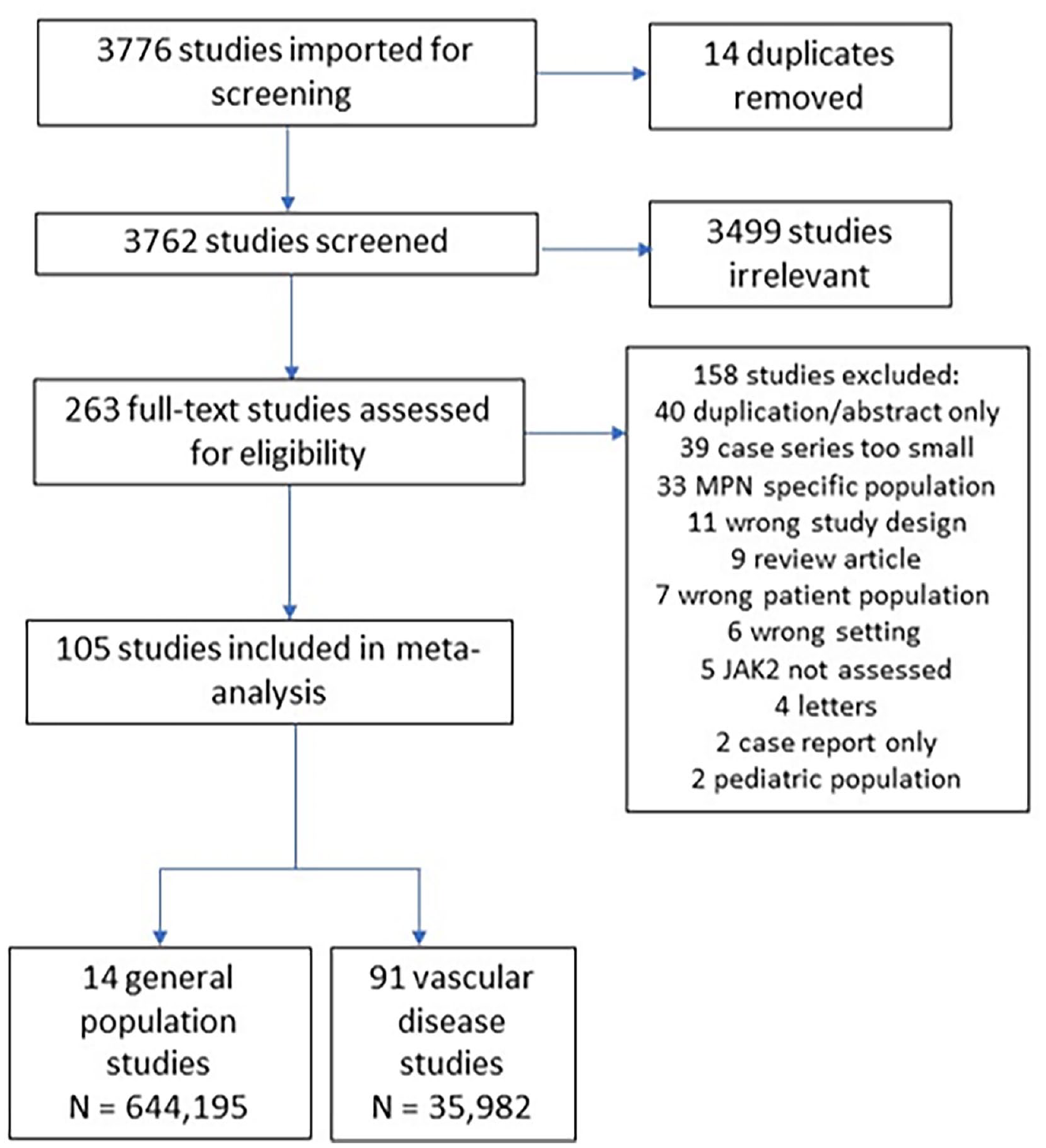
Study selection progression.
Poster No. 39
Abstract ID No.1498634
Magneto eTrieve™ PE System – a novel therapeutic concept for endovascular thrombectomy
Vladimir Lakhter DO, FSVM
Temple University Hospital - Lewis Katz School of Medicine
Background: The Magneto eTrieve PE Kit brings a novel therapeutic concept to the field of endovascular thrombectomy. It comprises the eTrieve catheter, which utilizes electric forces to create bonding with the clot, and an Aspiration System, a large bore aspiration system. The device is intended for the non-surgical removal of emboli and thrombi from the pulmonary arteries in subjects experiencing pulmonary embolism (PE) and deemed to be at an intermediate risk for mortality.
Methods: The first documented case for observing electro-thrombosis was reported in 1824, when it was observed that blood thrombosed at a positive but not a negative electrode. This concept was further investigated with various research groups who assessed the phenomenon for the treatment of aneurisms. In the 1950s and 60s, it was demonstrated that use of direct current may also aid in cases of uncontrolled bleeding. The dominant components of blood clots are fibrin and Red Blood Cells (RBC), and clots are classified as either RBC rich or fibrin rich. The more mature the clot, the higher the fibrin content, which is the typical case for pulmonary embolism. Both fibrin and RBC have an inherent negative surface charge.
Results: The eTrieve Catheter is an over-the-wire thrombectomy device. It is constructed of a positively charged electrode at its distal end, intended to be in direct contact with the target clot. The unique combination between a large bore aspiration system and an electrical retriever allows for a comprehensive solution and optimal retrieval of clots for a wide variety of PE patients.
Conclusion: The Magneto eTrieve PE Kit was tested in a FIH study and demonstrated promising results. It is now being studied in a pivotal trial in the US, Europe, and Israel. The trial, eTrieve II, aims to evaluate the safety and effectiveness of the device in the treatment of acute pulmonary embolism. A total of 130 subjects will be enrolled at 25 sites. Subjects are being followed for 30 days post index thrombectomy procedure. Primary endpoints include Major Adverse Events at 48 hours for safety and change in RV/LV ratio at 48 hours for efficacy. Secondary endpoints and other observational measures include functionality, safety and quality of life assessments.
eTrieve PE Kit.
Poster No. 40 - Withdrawn
Poster No. 41
Abstract ID No.1491844
Optimizing platelet inhibition in peripheral artery disease: a comparison of mono-antiplatelet therapy and dual-antiplatelet therapy using thromboelastography
Ivy Lee, BS, Sasha Suarez Ferreira, BS., Ryan P. Hall, MD, Monica Majumdar, MD, Tiffany Bellomo, MD, Samuel Jessula, MD, Kathryn Nuzzolo, BS, Nikolaos Zacharias, MD, Anahita Dua, MBChB, MBS, MSC
Massachusetts General Hospital
Background: Antiplatelet therapy is used to prevent thrombosis in patients with peripheral artery disease (PAD) following revascularization. However, the current standard of care for these patients remains at the physician’s discretion, varying from mono-antiplatelet therapy (MAPT) to dual-antiplatelet therapy (DAPT). Viscoelastic assays such as Thromboelastography with Platelet Mapping (TEG-PM) provide insight into individual coagulation profiles and measure real-time platelet function. This prospective, observational study looks at the differences in platelet function for patients on MAPT versus DAPT using TEG-PM.
Methods: Patients with PAD undergoing revascularization from 2020 - 2022 were prospectively evaluated. TEG-PM analysis compared platelet function for patients prescribed MAPT (aspirin or clopidogrel) at the initial encounter and DAPT (aspirin and clopidogrel) at the next visit. Platelet function measured in percent arachidonic acid (AA) and adenosine diphosphate (ADP) inhibition was evaluated that these visits, and within-group t-tests were performed.
Results: Of the 195 patients enrolled, 486 samples were analyzed by TEG-PM. Thirty-five patients met the study criteria. For patients initially prescribed Aspirin MAPT, an increase of 69.8% in mean ADP inhibition was exhibited when transitioning to DAPT [23.1% vs. 39.1%, p=.02], as well as an increase of 23.8% in mean AA inhibition when transitioning to DAPT [63.0% vs. 77.8%, p=.02]. For patients prescribed initial clopidogrel MAPT, an increase of 40.9% in antiplatelet inhibition was exhibited on DAPT compared to the MAPT state [72.1% vs. 51.1%, p = .38].
Conclusion: Patients on DAPT showed a significant increase in platelet inhibition when compared to initial aspirin MAPT. No significant difference in platelet inhibition was shown for patients on DAPT when compared to initial Clopidogrel MAPT. The results show that patients may benefit from DAPT post-revascularization. Personalizing antiplatelet therapy with objective viscoelastic testing to confirm adequate treatment may be the next step in optimizing patient outcomes to reduce thrombosis in PAD patients.
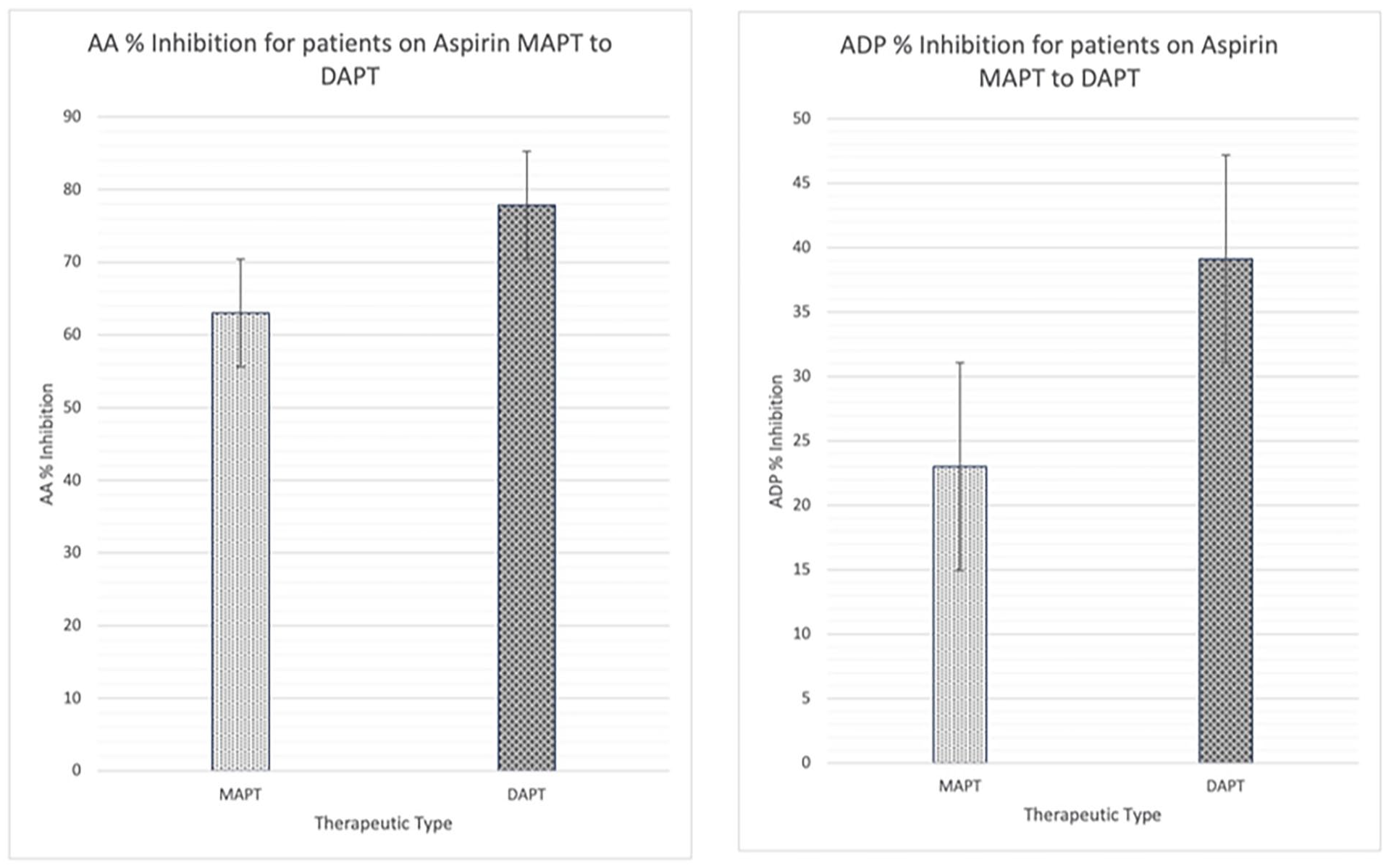
Platelet inhibition with aspirin MAPT and DAPT.
Poster No. 42
Abstract ID No.1498501
Effect of metabolic cardiovascular diseases risk factors on post-thrombotic syndrome outcomes in proximal deep vein thrombosis in the analysis of ATTRACT trial
Wenzhu Li, MD, FSVM1, Fangqin Wu, MD, PhD2, Qifang Huang, MD, PhD3, Yi Yang, MD4, Gaurav Parmar, MD, MPH, FSVM5.6, Ido Weiberg, MD, FSVM5, Peter Henke, MD7, Farouc Jaffer, MD, PhD5, Jiguang Wang, MD, PhD1
1Ruijin Hospital, 2The Second Affiliated Hospital of Nanchang University, 3Shanghai Institute of Hypertension, 4Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, 5Massachusetts General Hospital, 6Harvard Medical School, 7University of Michigan
Background: Despite anticoagulation (AC) and catheter-directed intervention (CDI), up to 50% of patients with proximal deep venous thrombosis (DVT) will develop the post-thrombotic syndrome (PTS). Whether metabolic cardiovascular disease risk factors (CVDRFs) like arterial hypertension (AHTN), diabetes and obesity influence PTS outcomes remains unclear.
Methods: We conducted a post-hoc analysis of DVT patients (N=692) of the NIH ATTRACT trial. The primary efficacy outcome was the PTS incidence rate, and the secondary efficacy outcome was the average Villalta score. The incidence rates were estimated by logistic regression and the average Villalta scores were estimated by linear regression, with adjustments for treatment (CDI+AC vs AC alone), DVT extent (iliofemoral vs femoropopliteal DVT) and baseline covariates (age, gender, Villalta score). To assess the effects of CVDRFs on PTS, baseline single RF or combined RFs (AHTN, high cholesterol, diabetes, and obesity) were included as additional covariates in the regression models.
Results: For the regression models with single RF, the PTS incidence rates and average Villalta scores were both significantly affected by AHTN [OR=1.48, 95% CI (1.05, 2.08), p=0.024; OR=2.35, 95% CI (1.17, 4.76), p=0.017; respectively], diabetes [OR=1.73, 95% CI (1.12, 2.68), p=0.014; OR=7.44, 95% CI (3.03, 18.29), p< 0.001; respectively] and obesity [OR=1.53, 95% CI (1.09, 2.14), p=0.014; OR=3.91, 95% CI (1.97, 7.75), p< 0.001; respectively]. For the logistic model with combined CVDRFs, the effects of AHTN, diabetes and obesity on PTS incidence rates were non-significant (p>0.05). Notably, the average Villalta scores were significantly affected by diabetes and obesity [OR=5.97, 95% CI (2.26, 15.76), p< 0.001; OR=3.03, 95% CI (1.50, 6.07), p=0.002; respectively] but not AHTN (p>0.05) in the linear regression model
Conclusion: The association of CVDRF with incidence and severity of PTS is complex. Baseline AHTN, diabetes and obesity are associated with a higher PTS incidence and worse Villalta scores based on single RF adjustment. When adjusting for multiple RFs, diabetes and obesity are associated with worse PTS. Mechanisms underlying these findings warrant further investigation.
Poster No. 43
Abstract ID No.1498335
In-hospital outcomes of catheter-directed intervention versus systemic thrombolysis in acute high-risk saddle pulmonary embolism patients: insights from Nationwide Inpatient Sample
Wenzhu Li, MD, FSVM1, Fangqin Wu, MD, PhD2, Rahul Sakhuja, MD3, Ido Weiberg, MD, FSVM3, Gaurav Parmar, MD, MPH, FSVM3,4
1Ruijin Hospital, 2The Second Affiliated Hospital of Nanchang University, 3Massachusetts General Hospital, 4Harvard Medical School
Background: While acute saddle pulmonary embolism (ASPE) can be asymptomatic, it can also cause sudden hemodynamic collapse and death. Systemic thrombolysis (ST) improves early hemodynamic status but is associated with a high incidence rate of major bleeding. Whether catheter-directed intervention (CDI) like catheter-directed thrombolysis and thrombectomy is superior to ST in ASPE patients with high-risk PE in-hospital is unclear.
Methods: The study cohort was derived from the HUCP’s Nationwide Inpatient Sample (NIS) from 2016-2019, according to ICD-10 code system to identify the ASPE patients and related procedures. We used multivariate logistic regression and linear regression to explore the impact of the types of treatment on all-cause mortality, length of stay and total charges in-hospital. The models were adjusted for treatment (ST only vs CDI only), implantation of inferior vena cava filter, age, gender, race, hypertension, dyslipidemia, obesity, and diabetes.
Results: We identified 4136 ASPE patients in NIS datasets from 2016-2019. Among them, 2404 patients did not receive CDI nor ST; 476 patients received ST only; 1201 patients received CDI only; 55 patients received both ST and CDT. And only 47 patients received therapy of extra-corporeal membrane oxygenation (ECMO). In the patients with CDI only (N=1201) and ST only (N=476), the in-hospital mortality rate was significantly affected by the treatments [ST/CDI, OR=1.97, 95% CI (1.30, 2.99), p=0.001]. The length of stay was also significantly affected by the treatments [ST/CDI, OR=2.78, 95% CI (1.39, 5.55), p=0.004]. Notably, the total in-hospital charges were not affected by the treatments (p>0.05).
Conclusion: Compared to ST, ASPE patients with CDI therapy experienced a lower mortality rate and shorter length of stay in-hospital, without an increase in total in-hospital charges. Whether selection bias is a contributing factor requires further study.
Poster No. 44
Abstract ID No.1497282
Clinicodemographic profiles and outcomes of complex lymphatic therapy among patients with lymphedema: a single-center, descriptive-analytic study
Queenette Blaise D. Mateo, Diana Jean Roxas, Jonathan James Bernardo, Roi Joseph Mendoza, Jason Francis Roxas
St. Luke's Medical Center-Bonifacio Global City Philippines
Background: Lymphedema is a chronic, progressive vascular disease entailing lifelong management. Awareness of the clinicodemographic characteristics of patients with lymphedema is imperative in optimizing conservative, first-line management through complex lymphatic therapy (CLT).
Methods: Utilizing a retrospective-cohort design, 153 records of purposively-sampled adult in- and out-patients with lymphedema and received CLT from the Lymphedema Clinic of a tertiary referral hospital were examined. Alongside demographic and clinical data, baseline and post-CLT limb measurements were extracted and recorded. Limb volumes and circumferences and post-CLT lymphedema status were analyzed using Wilcoxon Signed-Rank test and polynomial logistic regression.
Results: Most patients had secondary lymphedema (96.73 %) attributed to cancer treatment (47.97%), and the upper extremities were commonly affected (67.30%; RUE=46.73%, LUE=49.53%, BUE=3.74%). Majority had Stage I lymphedema (58.82%), had lymphedema for less than 12 months (62.09%), and had undergone surgery (92.81%), chemotherapy (61.44%), and radiotherapy (55.56%). With a median of five CLT sessions, baseline limb volumes (UE: MD=2,550.43mL; LE: MD=998.98mL) and circumferences (UE: MD=0.71cm; LE: MD=1.85cm) significantly decreased (p=0.001), and 78.57% had improved lymphedema. The percentage change in upper and lower limb volumes were –7.01% and –1.19%, respectively, while percentage change in upper and lower limb circumferences were –2.88% and –4.15%. Moreover, higher completed CLT sessions increased the likelihood of improved lymphedema by 35% (OR=1.35, p=0.044).
Conclusion: Complex lymphatic therapy is effective against lymphedema, with substantial reduction in limb volumes and circumferences. Cognizant of its benefits, clinicians should encourage patients to adhere with CLT schedule to increase completed sessions and reduce lymphedema.
Poster No. 45
Abstract ID No.1511555
Attenuation of calf pain using ankle-foot orthoses during walking performance testing in patients with peripheral artery disease
Ryan J. Mays, PhD, MPH, MS1, Ashley A. Mays, MD2, Ryan L. Mizner, PhD3
1University of Minnesota, 2North Memorial Health Hospital, 3University of Montana
Background: Walking assistive devices called ankle-foot orthoses (AFO) have been shown to improve functional ability and quality of life in patients with peripheral artery disease (PAD). However, the acute effects of AFO used during submaximal exercise testing is unknown. The aim of this study was to evaluate the impact of AFO on perceptual and walking performance outcomes of patients with calf claudication during graded treadmill testing and the 6-minute walk test (6MWT).
Methods: This was a post-hoc, cross-sectional analysis of a previous open-label interventional study evaluating AFO in patients with PAD following an unstructured community-based walking exercise program. Patients (n=15) completed separate graded treadmill and 6MWTs at baseline using AFO and without AFO within one week. The current study primary outcome was ratings of calf pain using the Claudication Symptom Rating Scale with and without AFO during each stage of graded treadmill testing. Secondary outcomes included ratings of perceived exertion (RPE) and oxygen consumption (VO2) at each stage and number of stops during the 6MWT between the two conditions.
Results: Calf pain was significantly lower for patients (n=7) when using AFO compared to not using the devices only at Stage 5 (mean±SD: 3.0±1.5 vs. 4.3±0.5 min, p=0.049). Additionally, VO2 was lower when the devices were used by patients (n=3) vs. not using the AFO at Stage 7 of the graded treadmill test (18.0±1.8 vs. 19.9±0.6 ml·kg-1·min-1, p=0.02). The number of stops during the 6MWT demonstrated a near significant difference when using AFO compared to not using AFO (0.6±1.4 vs. 1.0±1.9 stops, p=0.05). Positive numerical trends were also observed during the graded treadmill test as patients on average had lower calf pain (6 of 7 stages), RPE (5 of 7 stages), and VO2 (5 of 7 stages) while using the AFO compared to without.
Conclusion: The use of AFO demonstrated a potential signal of benefit for reducing perceptions of pain and exertion during walking performance testing. Despite the other non-significant findings in this small sample, AFO is an intriguing area of exploration to attenuate calf pain, thereby increasing physical activity duration to improve outcomes in patients with PAD.
Poster No. 46
Abstract ID No.1508712
A descriptive analysis of a single center's multi-disciplinary lymphedema program
Shantum Misra, MD, Aaron Fleishman, MPH, Weiliang Sun, BA, Kevin Donohoe, MD, Leo L. Tsai, MD, PhD, Kathleen Shillue, PT, DPT, Dhruv Singhal, MD, Brett J. Carroll, MD
Beth Israel Deaconess Medical Center
Background: Lymphedema is a persistent, debilitating state of chronic edema and inflammation that affects over 250 million individuals worldwide. There are evolving treatment options for lymphedema and understanding the characteristics of patients who receive care at a multi-disciplinary lymphatic center may help guide evaluation and management strategies.
Methods: Patients with chronic lymphedema who presented for initial evaluation from 2016 to 2022 and were included in a prospective institutional lymphatic database were analyzed. Patients were divided into cancer-related lymphedema, primary lymphedema, and multifactorial edema with lymphedema (MEL). Demographic, descriptive, imaging, and therapeutic characteristics were assessed.
Results: Of the 911 patients with chronic lymphedema, 511 (56.1%) were cancer-related, 294 (32.3%) had primary lymphedema, and 106 (11.6%) had multifactorial edema with lymphedema (Table). In all three groups, the majority of patients were white women between the ages of 50 to 60 years old. Breast cancer (29.9%) was the leading cause of malignancy among patients with cancer-related lymphedema. Primary lymphedema patients had the highest rate of infections (39.8%). The primary goal of treatment was to reduce associated symptoms in all groups, with improvement in appearance being a rare goal. Cancer-related and primary patients had similar rates of lymphoscintigraphy performed. Overall, 12.8% of patients evaluated underwent a lymphatic surgery; cancer-related patients more frequently than primary patients (17% vs. 9.86%). Cancer-related patients who underwent surgery had an average of 18 lymph nodes removed at the time of their initial cancer treatment compared to 13 in those that did not receive surgery.
Conclusion: A wide variety of patients present to a multidisciplinary lymphedema program. Only a small subset receive lymphatic specific imaging and lymphatic surgery. A team-based approach may offer a more comprehensive evaluation and management given only a minority are ultimately deemed appropriate for surgery.
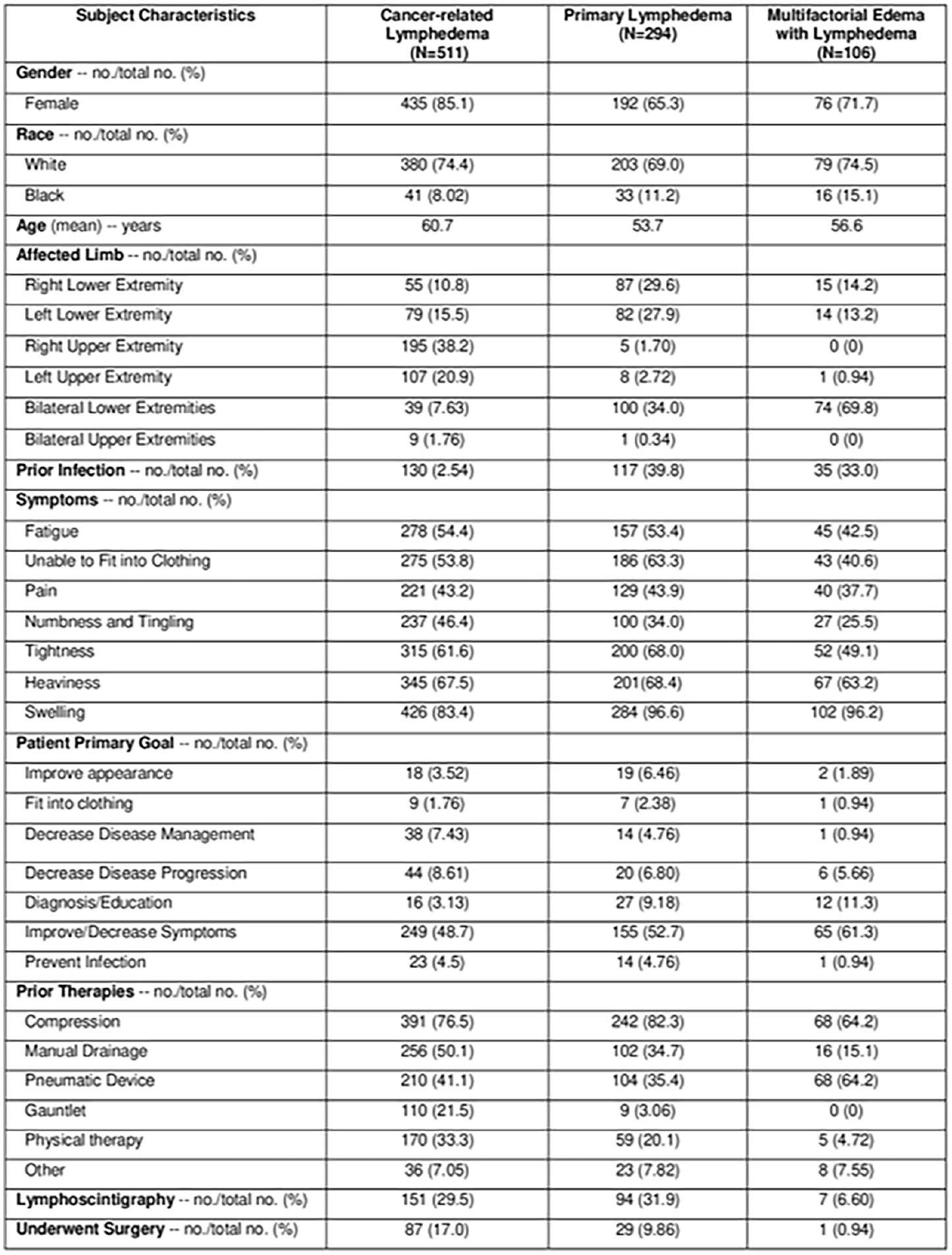
Poster No. 47
Abstract ID No.1494119
Death certificate validity in patients with acute pulmonary embolism
William Earle, MD, Milan Kaushik, MD, Shantum Misra, MD, Brett J. Carroll, MD, Eric A. Secemsky, MD, MSc
Harvard Medical School, Beth Israel Deaconess Medical Center
Background: Pulmonary embolism (PE) associated mortality has risen over the past decade, but definitions vary in the literature. This variability can impact mortality measures. Prior studies have found discordance between cause of death reported on death certificates and expert adjudication, but this has not been assessed in contemporary patients with acute PE.
Methods: We included patients admitted to a tertiary care hospital with an acute PE diagnosis between August 1, 2012 and July 1, 2018. A retrospective chart review was performed to identify patients who died prior to discharge. Cause of death was adjudicated by 2 independent investigators and compared with death certificate documentation.
Results: Of 2,052 patients admitted with acute PE (53.1% women, 65.5% white, average age 63.1±16.3 years), 6.3% (n=130) died before discharge. Of those who died, PE-related mortality was adjudicated as the cause of death in 22.1%, compared with 19.2% based on death certificates (p < .001). Chief causes of death differed between sources in 64.6% of cases. The adjudicated cause of death was not mentioned on 20.0% of death certificates, of these, 15% were adjudicated as PE-related.
Conclusion: We found that the cause of death recorded on death certificates in patients with acute PE is often inconsistent. Reliance on death certificates alone for identifying PE-related mortality could introduce significant bias into studies. Additional interventions are needed to increase the accuracy of outcome measures if relying on death certificates.
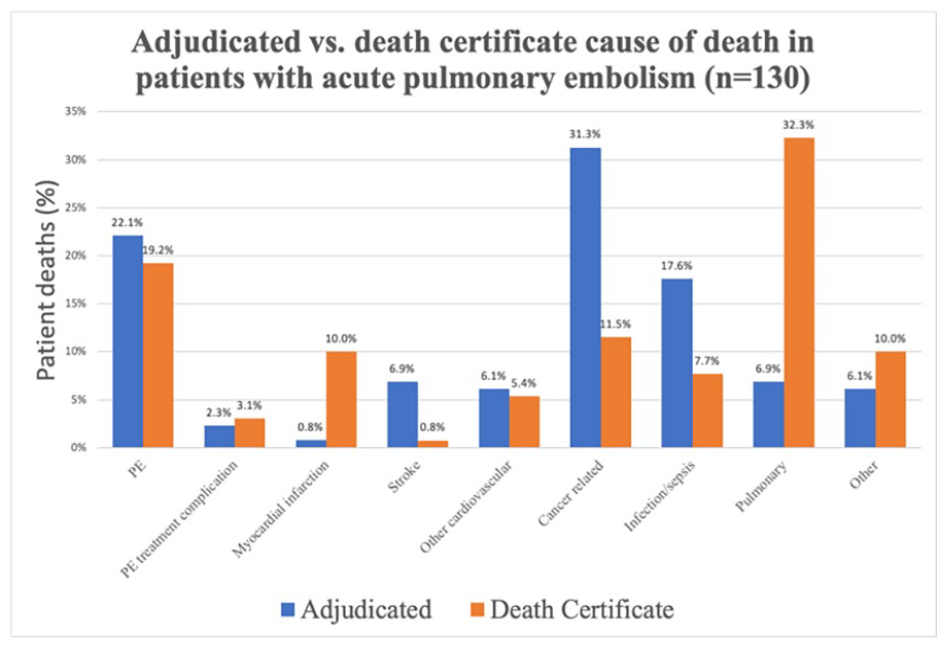
Adjudicated vs. death certificate cause of death in patients with acute pulmonary embolism (n=130).
Poster No. 48
Abstract ID No.1464584
Low-intensity pulsed ultrasound improves symptoms in peripheral arterial disease: a double-blinded, randomized, and placebo-controlled study
Farina Mohamad Yusoff, MBBS, PhD, FSVM, Masato Kajikawa, MD, PhD, Shinji Kishimoto, MD, PhD, Tatsuya Maruhashi, MD, PhD, Ayumu Nakashima, MD, PhD, Toshio Tsuji, PhD, Yukihito Higashi, MD, PhD, FAHA
Hiroshima University
Background: Pre-clinical studies have shown that low-intensity pulsed ultrasound (LIPUS) exposure induces angiogenesis through activation of the ERK/Akt/endothelial nitric oxide synthase (eNOS)/vascular endothelial growth factor (VEGF) signaling pathway. LIPUS irradiation may has beneficial effects on limb ischemia by inducing angiogenesis.
Methods: This was a prospective, double-blinded and randomized LIPUS study on patients with Peripheral Artery Disease (PAD). Eligible patients were randomly assigned to receive treatment with either active LIPUS equipment or dummy LIPUS equipment (ratio 1:1). The ultrasound irradiation was applied over the skin of the ischemic area of the thigh region at home 20 minutes every day for 24 weeks. Symptoms in affected leg were assessed during a 24-week period of LIPUS irradiation in 25 patients with PAD, including 12 patients with Buerger disease and 13 patients with atherosclerotic PAD, and twenty-five patients who did not receive LIPUS irradiation as controls.
Results: In Buerger disease and atherosclerotic PAD patients, rest pain intensity on visual analog score (VAS) was significantly decreased after 24-week LIPUS treatment. Skin perfusion pressure (SPP) was significantly increased in patients with Buerger disease but not in patients with PAD. LIPUS treatment had a tendency to increase ankle brachial pressure index (ABPI) and transcutaneous oxygen pressure (TcPO2), but not significantly during the 24-week period both in patients with Buerger disease and patients with PAD. There was no significant difference between ABPI, TcO2, SPP, and VAS in the control group. LIPUS increased the number of and migration of circulating progenitor cells in patients with Buerger disease and patients with PAD.
Conclusion: LIPUS is noninvasive, safe and effective in improving symptoms in patients with PAD.
Poster No. 49
Abstract ID No.1496249
Development of a high throughput CD73 enzymatic assay to measure extracellular adenosine generation in endothelial cells and to screen CD73 inhibitors
Jaideep Moitra, Natalia Dmitrieva, Robin Schwartzbeck, Bretagne Cowling, Elisa A. Ferrante, PhD, Cornelia Cudrici, Alessandra Brofferio, Manfred Boehm, Yogen Kanthi
NIH, NHLBI
Background: Over the past few years, CD73, the adenosine-generating 5’-ectonucleotidase, has attracted a lot of interest as a promising target for anti-cancer therapy. However, prolonged inhibition of CD73 may have adverse vascular effects. Thus, patients with ACDC, a rare, monogenic (NT5E) deficiency of CD73, develop premature arterial calcification and severe peripheral artery disease in the 2nd and 3rd decade of life.
Methods: To better understand the influence of CD73 inhibitors on vascular homeostasis, we developed a high throughput assay to assess the on-cell enzymatic activity of CD73 in vascular and hematopoietic cells, using AMP as the substrate for the CD73 enzyme.
Results: A sigmoidal cell-dependent increase in inorganic phosphate (Pi) generation was observed in the positive control cell line MDA-MB-231 and primary endothelial cells (human aortic (HAEC) and umbilical vein (HUVEC) endothelial cells). The limit of quantification was cell type dependent and varied between 150-625 cells/well; with a highly sensitive limit of detection as low as 35 cells/well. Using Pi generated per cell (qP) as a measure of adenosine generation, we found densities of cells in 96-well plates where they were maximally efficient in Pi generation (MDA-MB-231: 5,000 cells; HAEC and HUVEC: 2,500 cells). By varying input cell numbers around these optimal densities and AMP concentrations, we validated the Michaelis-Menten constants and increased the assay sensitivity for use in primary human endothelial cells compared with previous reports using cancer cell lines.
Conclusion: We then utilized this assay to quantify CD73 enzymatic activity in dermal fibroblasts from patients (n=8) with novel NT5E mutations for functional diagnosis of ACDC.
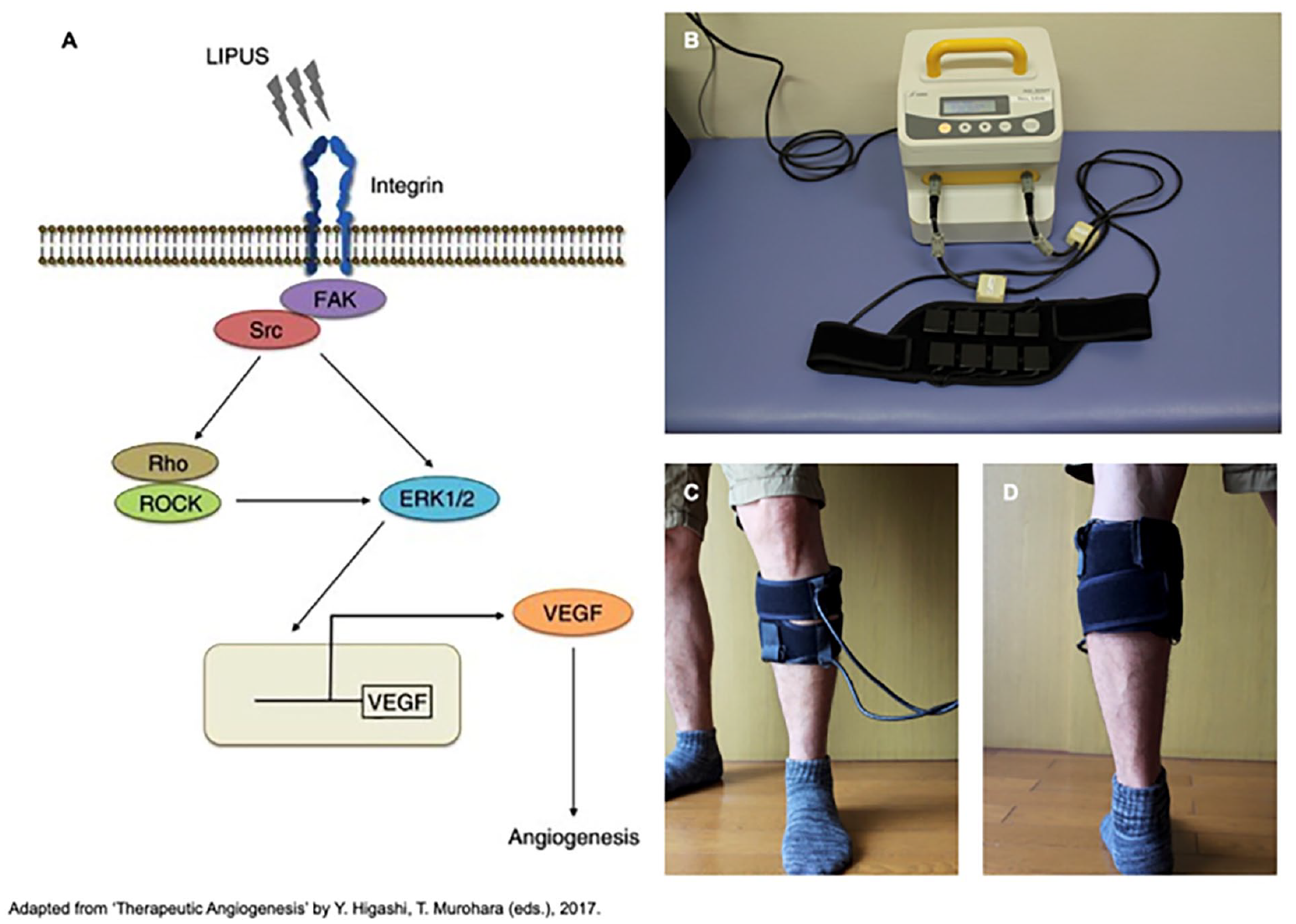
Putative mechanism of the low-intensity pulsed ultrasound (LIPUS) for therapeutic angiogenesis (A), appearance of device (B) and application of transducers for LIPUS irradiation in the gastrocnemius of the leg (C, D).
Poster No. 50
Abstract ID No.1509078
Yield of clinical genetic testing in patients with bicuspid aortic valve
Hunter Mwansa, MBBS, Mohamed Zghouzi, MD, Aroosa Malik, MD, Rajani Aatre, MS, MSc, LCGC, Lauren Humphrey-Stark, BS, Vikas Aggarwal, MBBS, MPH, Geoffrey Barnes, MD, MSc, James Froehlich, MD, MPH, Kim Eagle, MD, MS, Marion Hofmann Bowman, MD, PHD
University of Michigan
Background: Bicuspid aortic valve (BAV) has complex genetic underpinnings. The paucity of data on genetic yield in patients with BAV limits guideline recommendations on genetic testing. We aimed to assess the yield of clinical genetic testing in patients with BAV.
Methods: The Cardiovascular Health Improvement Project (CHIP), registry of aortic diseases, was screened for patients with BAV who underwent multigene aortic panel testing. Identified patients were assessed for the presence of a pathogenic or likely pathogenic gene variant for a heritable aortopathy to ascertain the genetic yield (Fig. 1).
Results: Of the 6147 patients in the CHIP, 1354 (22.0%) had BAV. 50 (0.8%) of the 1354 patients underwent genetic testing and 49 (0.8%) met the 2022 ACC/AHA criteria for genetic testing and were included in the analysis (Fig 1A). All 49 patients had HTAD-associated conditions including 6 (12.2%) with mitral valve disease (MVD), 9 (18.4%) had pathogenic or likely pathogenic gene variants, 11 (22.5%) had variants of uncertain significance and 29 (59.2%) had negative results (Fig 1B). 20 (40.8%) of the 49 patients with BAV had genetic results that led to further counseling or were directly relevant to patient care. 2 (33.3%) of the 6 patients with BAV, HTAD and MVD had pathogenic or likely pathogenic gene variants.
Conclusion: The study demonstrated high genetic yield (18.4%) for aortopathy genes in patients with BAV and HTAD. The higher genetic yield (33.3%) in patients with MVD requires further research.
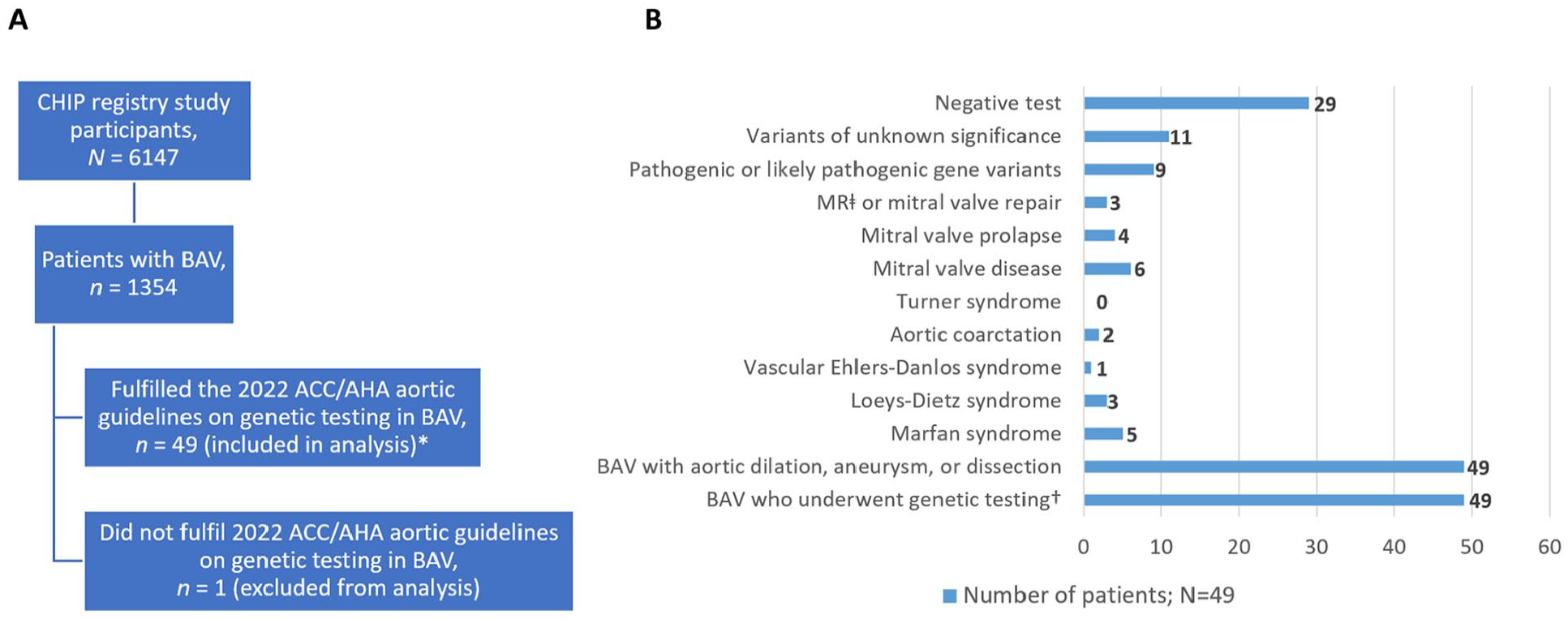
Flowchart of CHIP study participants and outcomes of clinical multigene aortic panel testing. A: *Demographic characteristics: mean (SD) age, 46 (13) years; mean (SD) height, 180 (10) cm; female sex, 9 (18%); non-Hispanic White, 48 (98%); other race/ethnicity, 1 (2%). B: †Patients with bicuspid aortic valve who fulfilled the 2022 ACC/AHA aortic guidelines on genetic testing; MRⱡ, moderate or severe mitral regurgitation; CHIP, Cardiovascular Health Improvement study.
Poster No. 51
Abstract ID No.1486565
Atrial fibrillation increases mortality risk following peripheral vascular intervention
Pradeep Nadeswaran, MD1, Li Ding, MD, MPH, PHD1, Gregory Magee, MD2, Parveen Garg, MD, MPH2
University of Southern California1, Keck Medicine of USC2
Background: The association of prevalent atrial fibrillation/flutter (AF) on adverse perioperative outcomes following peripheral vascular intervention (PVI) is not well known. Compared to lower extremity bypass surgery, PVI is performed more frequently and is oftentimes performed in individuals who may be deemed to high-risk for surgery. As these individuals are usually older with more comorbidities, AF is common in this population. We investigated the association of prevalent AF with the risk of inpatient mortality, myocardial infarction (MI), and hospital length of stay (LOS) in patients undergoing PVI.
Methods: Eligible individuals were those undergoing PVI between the years 2016 and 2022 in the Vascular Quality Initiative, a nationwide retrospective cohort study. Individuals undergoing PVI as part of the Vascular Quality Initiative between the years 2016 and 2022. Patients with a documented preoperative atrial dysrhythmia history and completed covariate data were included in the analysis. Multivariate logistic regression analysis was performed to determine the risk of AF on inpatient mortality, MI, and LOS, controlling for age, race, BMI, tobacco use, COPD, coronary heart disease, heart failure, cerebrovascular disease, hypertension, diabetes, renal function, statin use, anticoagulant use, and antiplatelet use.
Results: The analysis included 200,620 procedures (mean age=68.3 years, 60% male, 72% white), of which 28,136 (14%) had baseline AF. In fully adjusted analyses, patients with AF were at increased risk for inpatient mortality (odds ratio (OR): 1.69, confidence interval (CI): 1.37-2.074) and longer hospital LOS (incidence rate ration (IRR): 1.23, CI: 1.13-1.34). There was no observed risk of increased MI (OR: 0.89, CI: 0.67-1.18).
Conclusion: For individuals undergoing PVI, prevalent AF is associated with an increased risk of inpatient mortality and a longer hospital LOS. The presence of AF should be accounted for when risk stratifying patients being considered for PVI.
Poster No. 52
Abstract ID No.1509651
PAD diagnosed but lost to follow-up: a simple initiative to improve patient care
Tamra Parker-Davis, NP, Melinda Ryan, NP, Debra Puffenberger, PA, Aravinda Nanjundappa, MD, Schirron Campbell, PA, Natalia Fendrikova-Mahlay, MD, Scott Cameron, MD, PhD
Cleveland Clinic Foundation
Background: The ankle brachial index (ABI) is diagnostic for peripheral artery disease (PAD). Interpretation of the ABI is less well understood by clinicians not trained in vascular medicine. By evaluating abnormal ABI results over a defined capture period, we hypothesized that many patients with an abnormal ABI are not referred to a vascular specialist. Our goal was to determine if the addition of a simple quality assurance statement in the final ABI report could trigger vascular specialist referral.
Methods: We firstly targeted clinical specialties more commonly requesting ABI studies: cardiology, podiatry, cardiac surgery. An abnormal ABI (< 0.90) was used in a query of vascular lab over a 5 month period. The following narrative was added to the final paragraph of every abnormal ABI report and outcomes of the intervention were evaluated over 3 months: "The patient has an ABI consistent with a diagnosis of peripheral artery disease. Consider referral to a vascular specialist for evaluation."
Results: 80 patients were identified from 3 specialties for which actionable ABIs were never followed up (right leg, mean ABI 0.78 +/- 0.02; left leg mean ABI 0.79 +/- 0.03, n=80) and 37% of those patient had decreased ABI in the moderate or severe range. For abnormal ABIs, the following specialties referred for follow up to a vascular specialist: podiatry (61%), cardiology (17%), cardiac surgery (11%). After the intervention, 112 patients with an ABI < 0.9 were identified of which 65 were already cared for by a vascular specialist. Of 47 remaining patients, 26 (55%) were referred to a vascular specialist (62% to vascular surgery and 38% to vascular medicine) and some required revascularization. The following departments failed to refer, even with the formal prompt in the vascular lab report: cardiac surgery,, cardiology, and internal medicine.
Conclusion: A prompt in an ABI interpretation to make a diagnosis of PAD clear and suggesting referral to a vascular specialist was successful in 55% of patients with PAD. This was a brief and cost-effective mechanism to ensure specialized referral for patients with PAD. We identified several specialties that will be targeted for education on PAD to further increase quality of patient care.
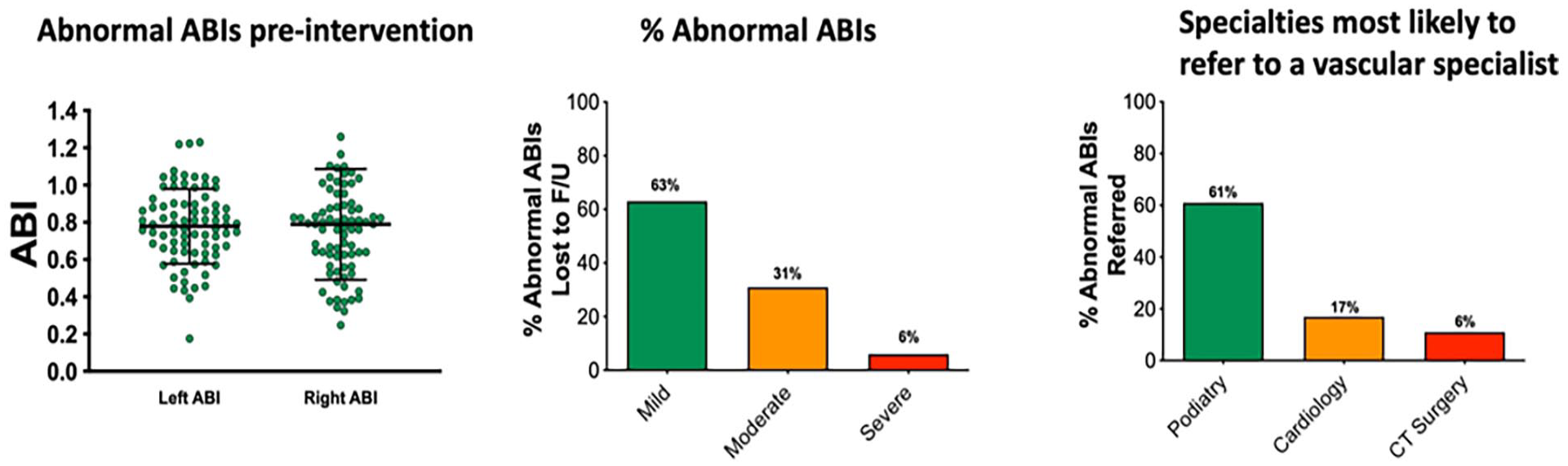
Pre-Intervention data on patients with PAD not referred.
Poster No. 53
Abstract ID No.1511620
Impact of risk factors control in polyvascular disease on long-term mortality amongst community-dwelling adults
Gaurav Parmar, MD, MPH, FSVM1,2, Rajasekhar Tanikella, MD, MPH3, Anahita Dua, MBChB, MBS, MSC1, Robert Schainfeld, DO1, Rahul Sakhuja, MD1, Ido Weiberg, MD, FSVM1
1Massachusetts General Hospital, 2Harvard Medical School, 3Beth Israel Deaconess Hospital-Needham
Background: Clinical atherosclerosis of multiple vascular beds has been associated with higher mortality. However, it is unclear if appropriate control of risk factors could mitigate this risk. We studied polyvascular disease at baseline with all-cause mortality for 20 years of follow-up in the National Health and Nutrition Examination Survey (NHANES).
Methods: We identified participants of age>40 years with information on the involvement of at least 3 vascular beds for survey years 1999-2004. Peripheral artery disease (PAD) was defined as ABI< 0.9. Involvement of other vascular beds (coronary and cerebrovascular) was self-reported by participants in a questionnaire. All-cause mortality was linked to all NHANES participants for follow-up through December 21, 2019, from the centers for disease control and prevention. Optimal risk factor control was defined when participants’ baseline evaluation showed blood pressure, low-density lipoprotein, and glycosylated hemoglobin were at goal for their disease state. Survival analysis was performed by Kaplan-Meier plots.
Results: Participants without any vascular disease (n=6063) had the lowest long-term mortality, followed by single vascular disease without (n=832) and with PAD (n=451). The highest mortality was observed in polyvascular disease without (n=85) and with PAD (n=196) (p< 0.0001) (Figure).
Conclusion: The presence of PAD as a component of polyvascular disease has a greater impact on long-term mortality compared to other vascular beds. Optimal risk factor control may not eliminate but mitigates some of the excess risks in polyvascular disease
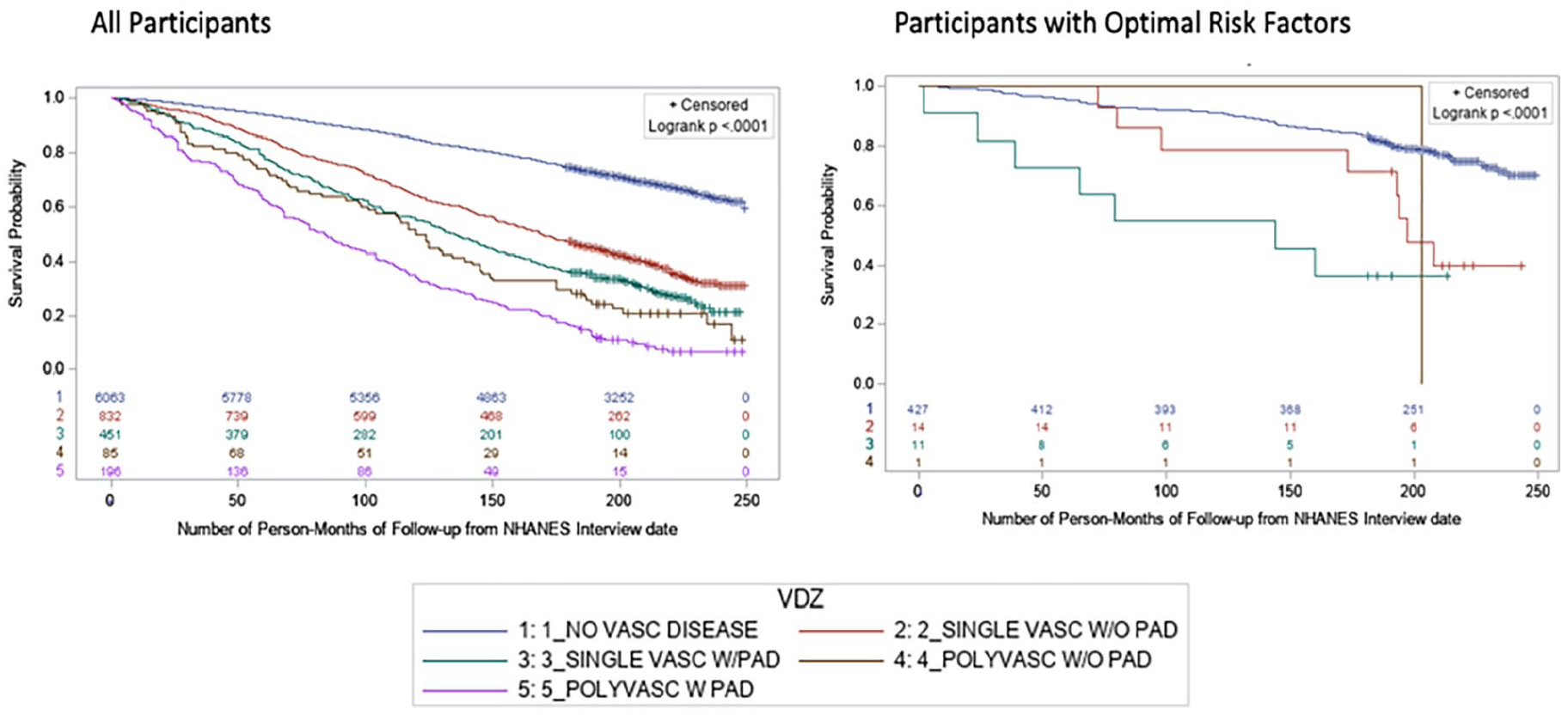
Poster No. 54
Abstract ID No.1511603
Lower baseline low-density lipoprotein cholesterol levels improved 20-year mortality in peripheral artery disease
Gaurav Parmar, MD, MPH, FSVM1,2, Arijeet Gattu, MBBS3, Rajasekhar Tanikella, MD, MPH4, Rahul Sakhuja, MD1, Robert Schainfeld, DO1, Anahita Dua, MBChB, MBS, MSC1, Ido Weiberg, MD, FSVM1
1Massachusetts General Hospital, 2Harvard Medical School, 3Brigham and Women's Hospital, 4Beth Israel Deaconess Hospital-Needham
Background: Aggressive lowering of low-density lipoprotein cholesterol (LDL) reduces cardiovascular risk in patients with peripheral artery disease (PAD). However, the impact of baseline low LDL is unclear. We studied the impact of baseline LDL on mortality in patients with and without PAD in the National Health and Nutrition Examination Survey (NHANES).
Methods: We identified participants age>40 years in whom ankle-brachial index (ABI) and a fasting lipid panel were available for survey years 1999-2004. LDL was calculated from total cholesterol, triglycerides, and high-density lipoprotein according to the Friedewald calculation. All-cause mortality was linked to all NHANES participants for follow-up through December 21, 2019, from the centers for disease control and prevention. Hazard ratios (HR) and 95% confidence intervals (CI) were calculated by multivariable cox-proportional regression.
Results: Of 3068 patients with available ABI and LDL, 261 (8.5%) had PAD (ABI< 0.9). Compared to the highest LDL (>191), the next lower LDL (161-190) had significantly reduced mortality (HR=0.22, p=0.022), and this benefit was maximum at the lowest LDL (41-55) (HR=0.10, p=0.003) in participants with PAD, after adjusting for other covariates such as age, sex, race, hypertension, diabetes, and smoking. This relationship did not exist in the absence of PAD (Table).
Conclusion: Lower LDL levels at baseline were associated with improved all-cause mortality in participants with PAD. Such a relationship was not present in the absence of PAD.
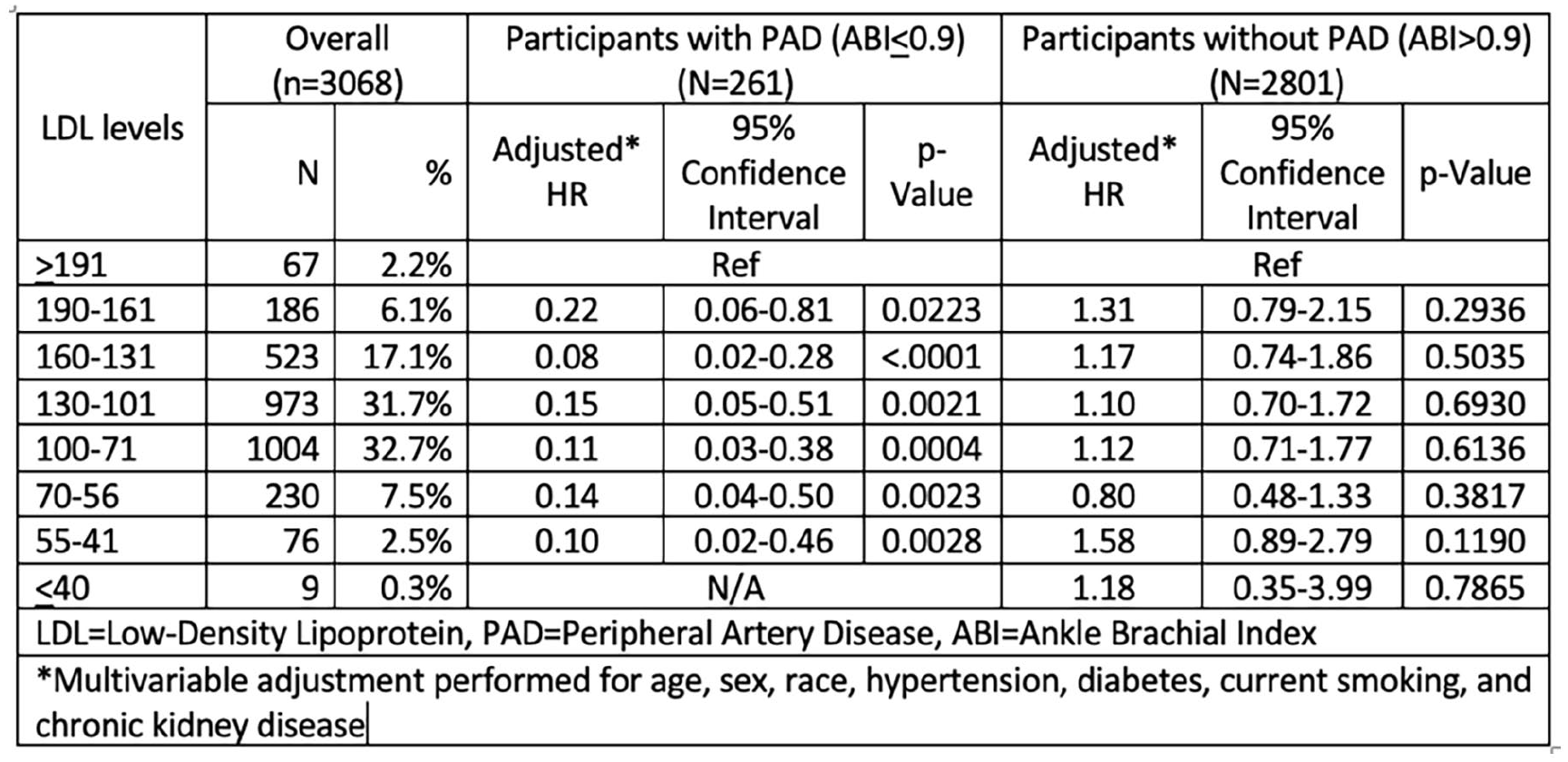
LDL and mortality in PAD.
Poster No. 55
Abstract ID No.1495051
Nonatherosclerotic renal arteriopathy - case study and review of literature
Nedaa Skeik, MD1, Johanna J. Theeler, BS2, Julia G. Wang, BS2, Aaron M. Bae, AB2, Mansoo Cho, BS2, Jesse M. Manunga, Jr., MD1
1Minneapolis Heart Institute, 2Minneapolis Heart Institute Foundation
Background: Non-atherosclerotic renal artery aneurysm, dissection, stenosis, vasculitis, and thromboembolism are rare vasculopathies with great clinical significance but scarce literature describing appropriate management and surveillance plans. We present our center’s experiences with renal arteriopathies to describe the incidence of underlying etiologies, presenting symptoms, diagnosis, management, and outcomes.
Methods: The charts of 2987 patients who presented to Abbott Northwestern Hospital in Minneapolis, MN between January 2000 to April 2022 were retrospectively reviewed for diagnoses of non-atherosclerotic renal artery vasculopathy. 227 patients met inclusion criteria and were analyzed. Patients were categorized according to demographics, symptoms, etiology, comorbidities, management strategies, imaging modality, symptom relief, and survival.
Results: The median age of included patients was 56 years with the majority being female (59%). We identified 91 patients with renal infarction (40%), 70 with renal artery dissection (31%), 69 with aneurysm (30%), 33 with stenosis (15%), and 32 with thrombosis (14%). The most common diagnoses were fibromuscular dysplasia (FMD) (n=86), thromboembolism (n=38), isolated aneurysm (n=33), and extension of thoracoabdominal aortic dissection (AD) (n=29). Patients most frequently presented with abdominal or flank pain (61%), though 30% remained asymptomatic. Prevalent comorbidities included hypertension (59%), tobacco use (49%), and hyperlipidemia (34%). CT angiogram was the most frequently used imaging modality (65%). Management strategies included antithrombotic therapy (70%), conservative (17%), endovascular (11%), and/or surgical repair (10%) with high survival (90%) and symptom relief (72%). Of those with follow-up imaging, 96% exhibited improved or stable imaging results at follow-up.
Conclusion: Renal arteriopathies are rare and can be caused by different etiologies.
Poster No. 56
Abstract ID No.1496784
Impact of antiplatelet medication dose on platelet inhibition in patients with peripheral artery disease
Sasha Suarez Ferreira, BS1, Ryan P. Hall, MD1, Monica Majumdar, MD1, Samuel Jessula, MD1, Tiffany Bellomo, MD1, Ivy Lee, BS1, Kathryn Nuzzolo, BS1, Gaurav Parmar, MD, MPH, FSVM1,2, Anahita Dua, MBChB, MBS, MSC1
1Massachusetts General Hospital, 2Harvard Medical School
Background: Antiplatelet therapy is a cornerstone of medical therapy in patients with peripheral artery disease (PAD) and is frequently dosed with a “one size fits all” approach. Our lab previously identified a platelet inhibition threshold that decreased thrombotic risk post revascularization using thromboelastography with platelet mapping (TEG-PM), a point of care test that quantifies the level of platelet inhibition in a patient blood sample. This study aimed to delineate the impact of various doses of antiplatelet medications on patient platelet inhibition.
Methods: All patients undergoing revascularization between December 2020 and February 2023 were enrolled prospectively. Patients on antiplatelet therapy (Aspirin, Clopidogrel and Ticagrelor) were divided in groups according to their current dose and drug regimen. Serial perioperative TEG-PM analysis was performed monthly up to six months postoperatively and the platelet function (percent of inhibition) was reviewed in the different groups. Statistical analysis was performed using unpaired t-test to compare platelet function.
Results: Over the study period, a total of 234 patients were enrolled. Of this cohort 165 patients met study criteria. 163 patients were on Aspirin from which 395 samples were analyzed (303 samples at 81mg, 11 samples at 300mg 78 samples at 325 mg, 3 samples at 600mg); 105 patients were on Clopidogrel (from which 223 samples were analyzed (200 samples at 75mg, 23 samples at 300mg); 3 patients were on Ticagrelor (90mg) from which 7 samples were analyzed. In the Aspirin cohort, the platelet inhibition was not different at 81mg, 300mg, 325mg and 600mg was 64.2%, 76.5%, 69.6% and 63.7% respectively (Figure). In the Clopidogrel cohort, the platelet inhibition at 75mg and 300mg was also not different at 45.2% and 42.7% respectively. In the Ticagrelor cohort, the platelet inhibition at 90mg was 33.8%. There were no bleeding events recorded in this cohort.
Conclusion: There was no difference in platelet inhibition at lower or higher doses in patients on Aspirin, Clopidogrel or Ticagrelor. Patients on lower doses may be able to get similar antithrombotic effect than patients on higher doses of antiplatelets.
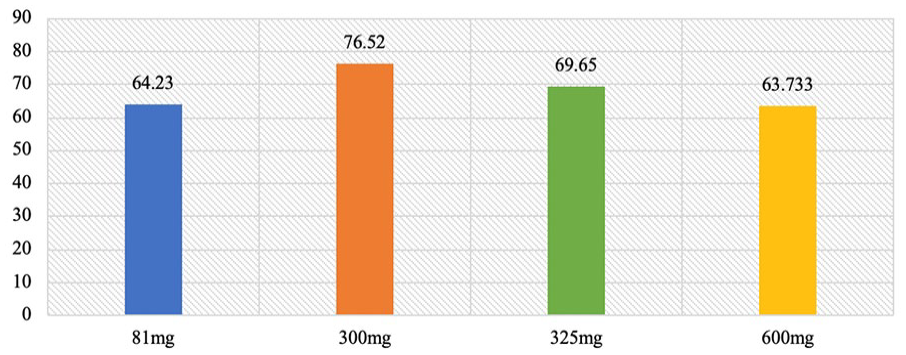
Platelet inhibition with aspirin.
Poster No. 57
Abstract ID No.1498482
Chemical adhesive embolization and risk of endovenous glue induced thrombosis meta-analysis
Nedaa Skeik, MD1, Kiahltone R. Thao2, Rami Musallam, MD3,4, Mahdi Hurreh2, Evan Walser-Kuntz, MS2, Jesse M. Manunga, Jr., MD1
1Minneapolis Heart Institute, 2Minneapolis Heart Institute Foundation, 3Case Western Reverse University, 4University Hospitals Cleveland Medical Center
Background: Chemical adhesive closure (CAC) is a more recent vein closure technique in patients with chronic venous insufficiency (CVI), with comparable efficacy to thermal ablation but with faster recovery. Although endovenous glue-induced thrombosis (EGIT) is a rare complication after CAC, more research on the clinical features of this phenomenon including prevalence and potential associations with deep vein thrombosis (DVT) and pulmonary embolism (PE), are needed to make informed decisions regarding the safety and efficacy of this technique.
Methods: A retrospective chart analysis of patients treated with CAC at our institution between January 2018 to May 2022 was completed. Patient records were reviewed to assess demographics, site and severity of CVI, procedure details and outcomes at follow up visit. A comprehensive literature search of PubMed/Medline, Embase, and Cochrane was then conducted on December 2022, to include all studies that reported EGIT cases among patients undergoing CAC. The outcomes of our meta-analysis included the prevalence of EGIT, DVT, and PE.
Results: A total of 20 studies (11 retrospective cohort, 6 prospective, and 3 randomized clinical trials) where 2,393 patients were included. The pooled prevalence rate of EGIT was 1.2 % (95% CI 0.005 - 0.019, I2=44.47%). There were 4 cases of EGIT Grade 3 or higher. There were two reported cases of CAC related DVT and no related cases of PE. In our patients’ cohort, age, treated vein size or procedure complexity were not significantly associated with increased risk of EGIT. There is insufficient data from the pooled analysis to determine strong risk factors for the development of EGIT.
Conclusion: Chemical adhesive closure is an effective treatment for CVI with a low prevalence of EGIT. There were two reported cases of CAC related DVT and no PE. Prospective, large-scale, multicenter studies are needed to further investigate significant risk factors, development, and significance of EGIT.
Poster No. 58
Abstract ID No.1498253
Thrombolytic and endovascular intervention for proximal deep vein thrombosis: clinical outcomes and demographics
Danielle Vlazny, PA-C, MS1, Damon Houghton, MD, MS2, Ana Casanegra, MD2, David Hodge, MS2, Teresa Lang, PA-C2, Shelly Keller, APRN, CNP2, Waldemar Wysokinski, MD, PhD2
1Mayo Clinic Rochester, 2Mayo Clinic
Background: Describe demographics and outcomes of patients with intervention for proximal deep vein thrombosis (DVT) given concerns about bleeding and venous thromboembolus (VTE) recurrence.
Methods: Using the Mayo Clinic VTE Registry, patients with proximal DVT enrolled between March 2013 and September 2022 had demographics, anticoagulation therapy, and outcomes compared between those with intervention versus not.
Results: Of 1,448 patients with proximal DVT 98 (6.8%) had intervention: 43 (3.0%) had thrombolytic therapy only, 24 (1.7%) endovascular only, and 31 (2.1%) with combined intervention. Patients with intervention were younger (57.9 v. 62.3 years, p=0.004), had more pulmonary embolus (51.0% v. 41.0%, p=0.053) and less underlying cancer (15.3% v. 37.6%, p< 0.001). Average duration of anticoagulation was similar in both groups (7.2 v. 6.7 months, p=0.723). Outpatient anticoagulation was not different between groups and no difference in antiplatelet use (p=0.311). VTE recurrence (7.06 v. 5.11, p=0.139), major bleeding (4.35 v. 5.56, p=0.856) and clinically relevant non-major bleeding (6.04 v. 8.25, p=0.938) were the same despite intervention (see Figure). Death was significantly lower in patients treated with intervention (12.30 v. 30.41, p< 0.001).
Conclusion: Patients undergoing intervention did not have higher VTE recurrence or bleeding compared to those treated with anticoagulation only. Better survival with intervention reflects younger age and lower incidence of cancer.
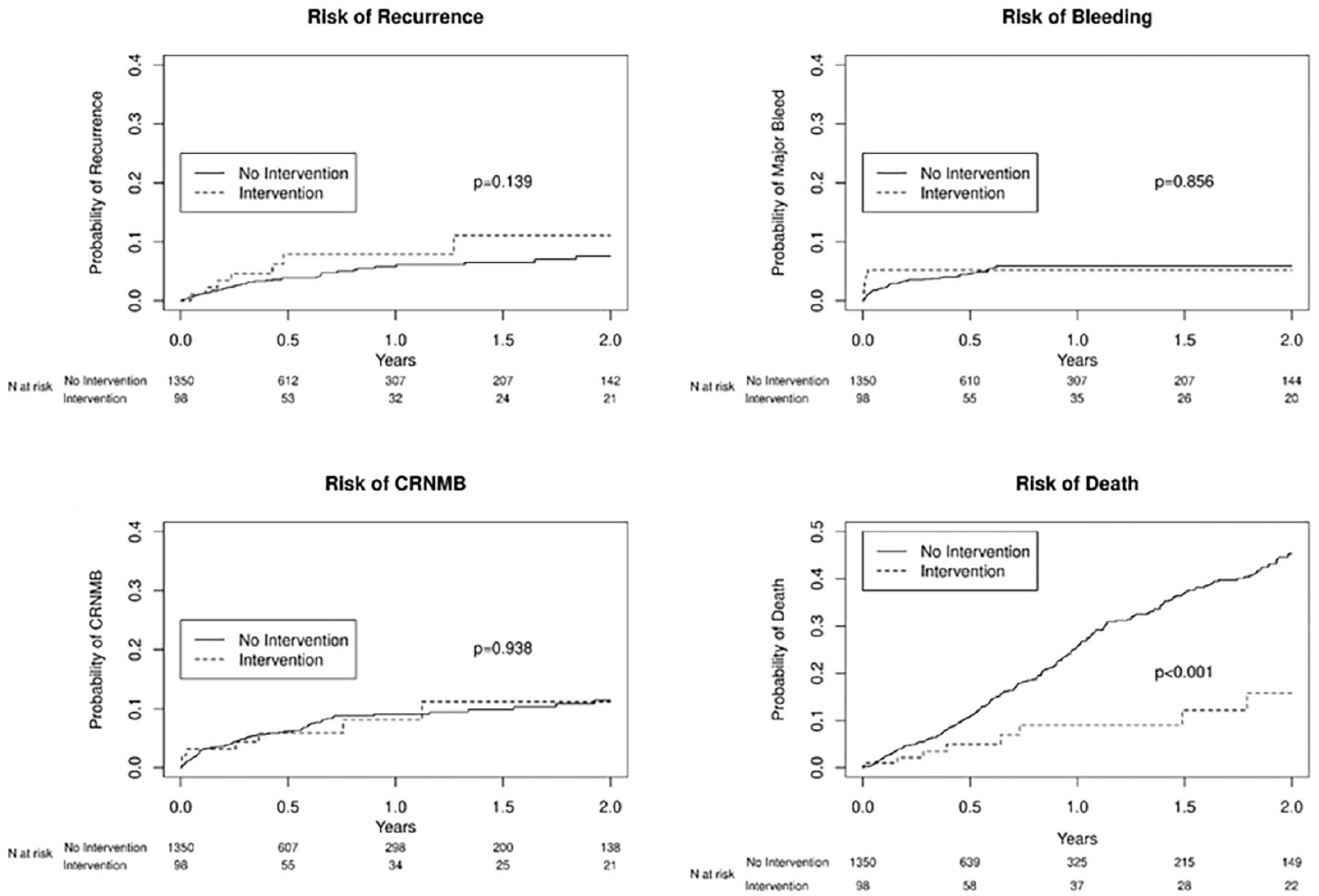
Kaplan-Meier curves depicting outcomes in patients undergoing intervention versus those treated with anticoagulation alone.
Poster No. 59
Abstract ID No.1494236
Diffuse genetalized venulitis as the primary pathology of Behcet's disease: a comprehensive magnetic resonance venography study
Hazan Karadeniz1, Murat Ucar1, Tunjay Mammadov1, Leyla Salimli Mirzayeva1, Abdurrahman Tufan2
1Gazi University Faculty of Medicine, 2National Human Genome Research Institute/NIH
Background: Behçet’s Disease (BD) is a chronic multisystem vasculitis that manifests with destructive inflammation affecting the eyes, central nervous system, and blood vessels. The pathology of vein involvement in BD is poorly characterized. Magnetic resonance (MR) venography gives more comprehensive information about deep veins and adjacent tissues. In this study, we aimed to characterize vein involvement and evaluate the diagnostic utility of MR venography in BD.
Methods: Sixty-five BD patients who fulfilled the International Study Group (ISG) criteria and 20 healthy control subjects were enrolled. BD patients were separated into two groups based on their previous history of vascular involvement. Inferior vena cava (IVC), common iliac veins (CIV), external (EIV) and internal iliac veins (IVV), common femoral veins (CFV), femoral veins (FV), and greater saphenous veins (GSV) of BD patients and healthy controls were evaluated with MR venography and ultrasonography for the presence pathologic features, luminal thrombi, vessel wall changes, and perivascular abnormalities.
Results: 33 vascular and 32 non-vascular BD patients (mean age 39.3±11.3 years and 48 [73.8%] male) were enrolled. MR venography revealed diffuse concentric thickening of the walls of IVC, CIV, EIV, IIV, CFV, FV, and GSV in BD (healthy controls vs. BD p< 0.05 for all vein segments). There was no significant difference between vascular and non-vascular BD groups regarding vein diameter and wall thicknesses, while both groups had significantly thicker veins than healthy controls (p< 0.05). US examination revealed similar results. MR venography provided additional information about veins and perivascular tissues like contrast enhancement, enlarged lymph nodes, and seminal vesicle vascularization, which were remarkably more frequent in vascular BD than non-vascular BD and healthy controls.
Conclusion: The results of our study suggest that the involvement of the venous system is diffuse and generalized in BD, and demonstration of venulitis might help diagnose the disease. Further studies are needed to elucidate the prognostic role of wall thickening, venulitis, in anticipation of future thrombosis and treatment response
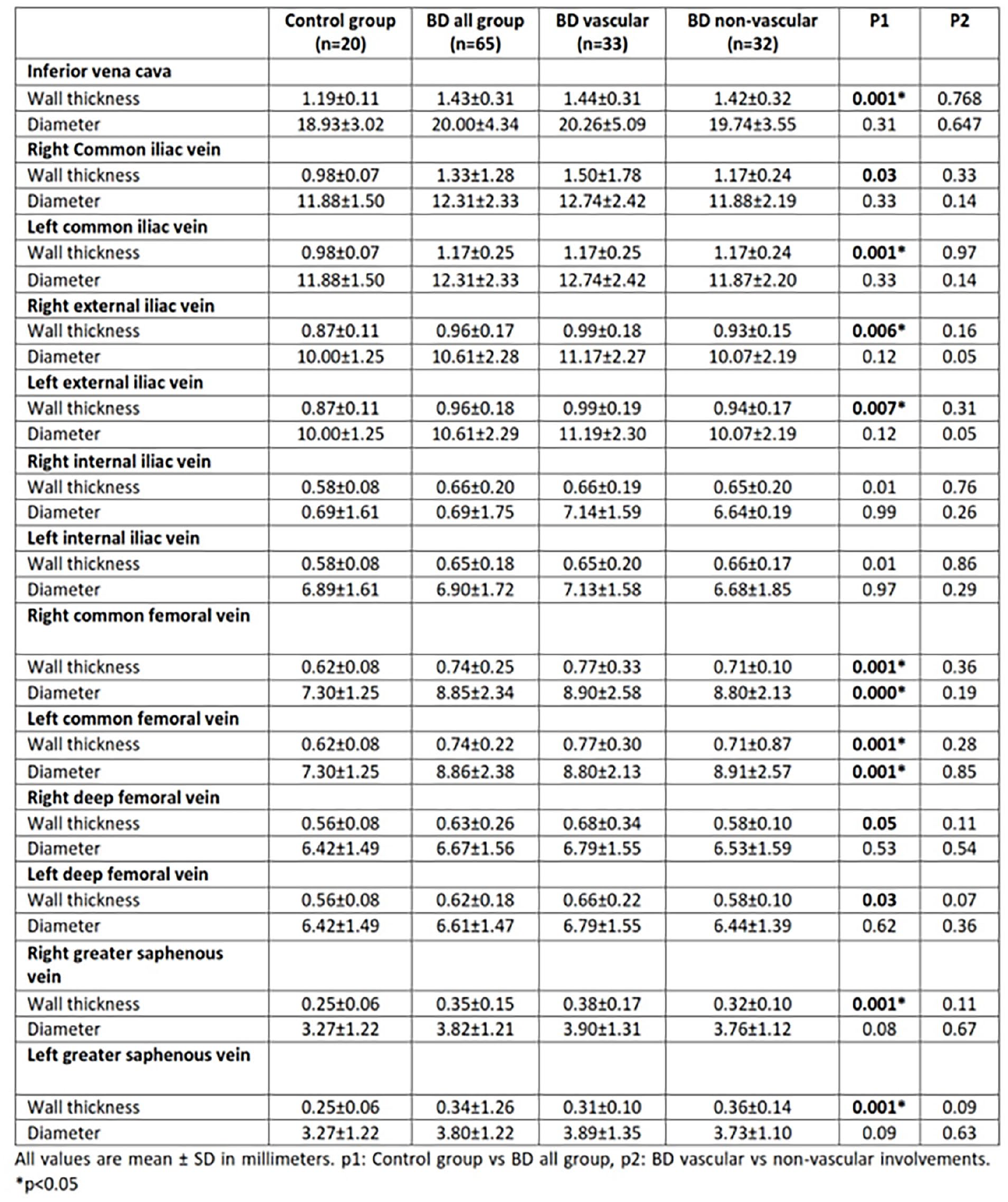
Comparison of magnetic resonance (MR) venography findings with respect to vascular and non-vascular involvements of Behçet’s disease.