
Abstract

An 83-year-old man presented with skin lesions. He had a history of mechanical replacement of the aortic and mitral valves with St Jude valves, atrial fibrillation, mixed ischemic/nonischemic cardiomyopathy with a left ventricular ejection fraction of 28%, transient ischemic attack, chronic obstructive pulmonary disease, Paget’s disease, and prostate cancer (in remission).
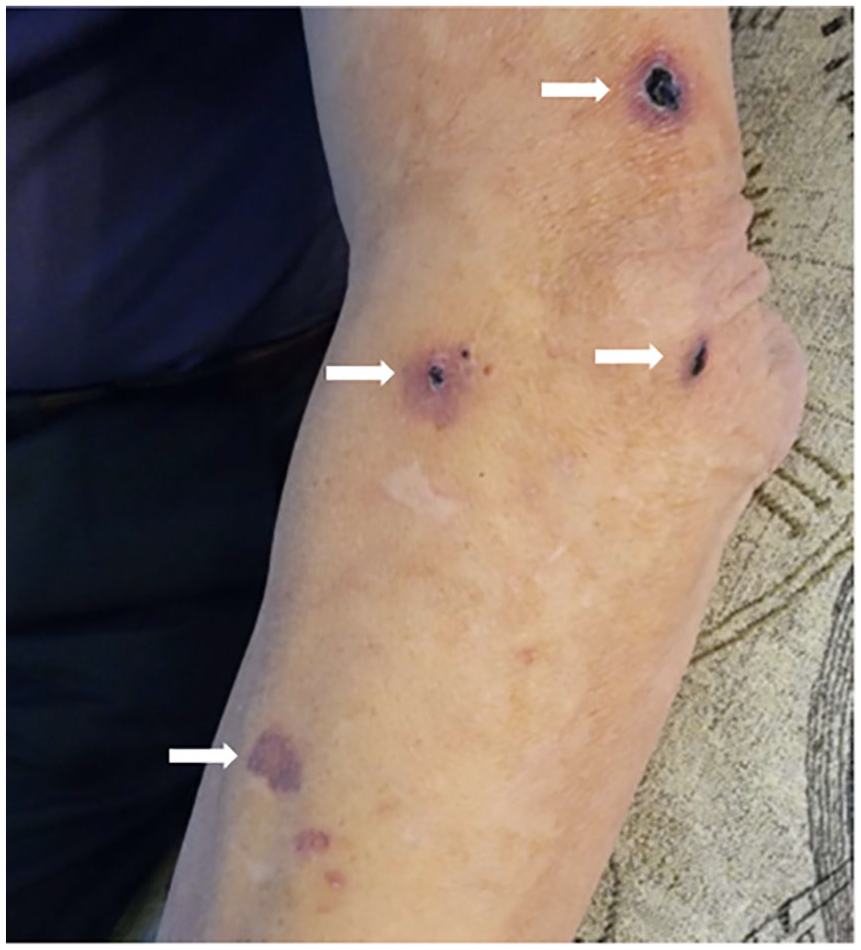
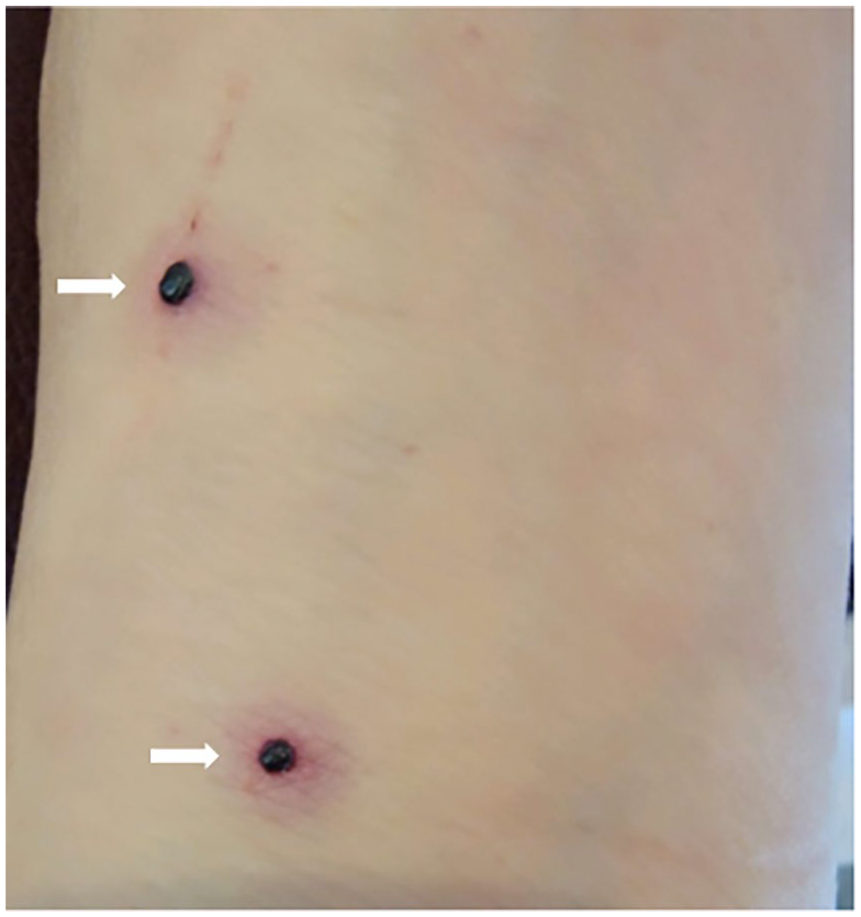
The patient had taken warfarin (target international normalized ratio [INR] 2.5–3.5) due to cardiac valve surgery for over 2 decades. Two years prior to his current presentation, he needed enoxaparin for a subtherapeutic INR. After receiving five injections of 100 mg of enoxaparin, he developed lesions all over his body (Panel A). Accordingly, he was advised to avoid using all forms of heparin due to concern about heparin-induced skin necrosis (there was no thrombosis or thrombocytopenia). Two years later, the patient had another subtherapeutic INR of 1.90 and was prescribed fondaparinux sodium 7.5 mg subcutaneously. Unfortunately, he immediately developed recurrent tense hemorrhagic bullae on the left arm, elbow, and shin, which were neither painful nor pruritic (Panel B). These lesions were like those observed after the prior enoxaparin administration. Apart from these findings, no petechiae or other bleeding signs occurred. The coagulation profile, platelet count, heparin platelet factor 4 (HPF-4), and serotonin release assay were normal 2 days after the lesions appeared. Both incidents resolved once the medication was stopped.
Bullous hemorrhagic dermatosis is a rare, nonimmune reaction mostly to unfractionated heparin (UFH) and low-molecular-weight heparins (LMWH), but it can also occur with other anticoagulants, such as fondaparinux.1,2 Uceda-Martin et al. 3 described 94 cases of postanticoagulant bullous hemorrhagic dermatosis distant from the injection sites which developed after LMWH in 73 (77.6%) patients, UFH in 11 (11.7%) patients, and fondaparinux in 10 (10.6%) patients.
The pathophysiologic relationship between heparins and these hemorrhagic lesions is unclear, and to our knowledge has not been reported with direct oral anticoagulants or vitamin K antagonists. Treatment typically involves monitoring and supportive care until the lesions resolve. Although hemorrhagic blisters cause discomfort and alarm, the condition is otherwise benign, does not affect coagulation tests or platelet counts, and should not be confused with heparin-induced skin necrosis.
Footnotes
Note - Images are in color online.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.