
Abstract

A 71-year-old woman with a history of polymyalgia rheumatica presented to the vascular medicine clinic with long-standing bilateral proximal anterolateral calf lesions and a diagnosis of venous insufficiency, stasis dermatitis, and ‘lipodermatosclerosis’. She was evaluated by venous and dermatology specialists years before her current presentation and was managed with bilateral great saphenous vein (GSV) ablations and clobetasol cream with little symptom relief. A venous insufficiency test was negative for venous reflux and demonstrated successful GSV ablation. At the time of presentation, she reported mild pain and itch, but the persistence of the skin lesions was the most bothersome complaint. She denied new or worsening fatigue, weight loss, appetite loss, low-grade fevers, chills, and night sweats. Physical examination revealed erythematous and slightly pigmented indurated plaques on the anterolateral aspects of the bilateral calves (Panel A).

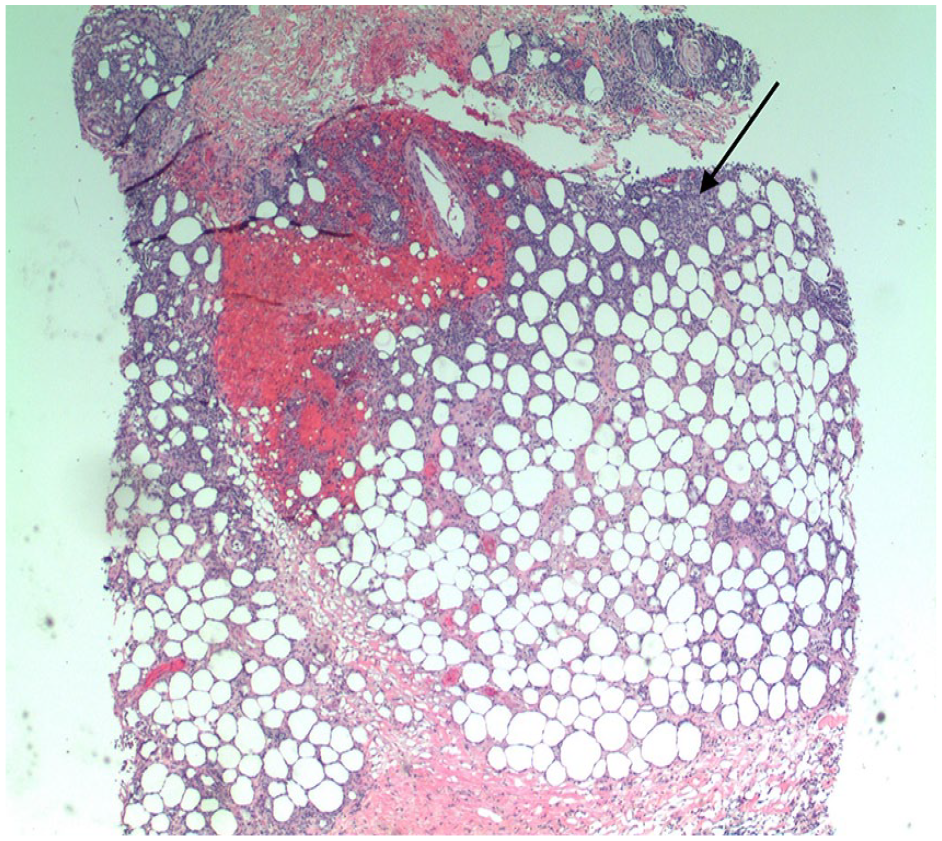
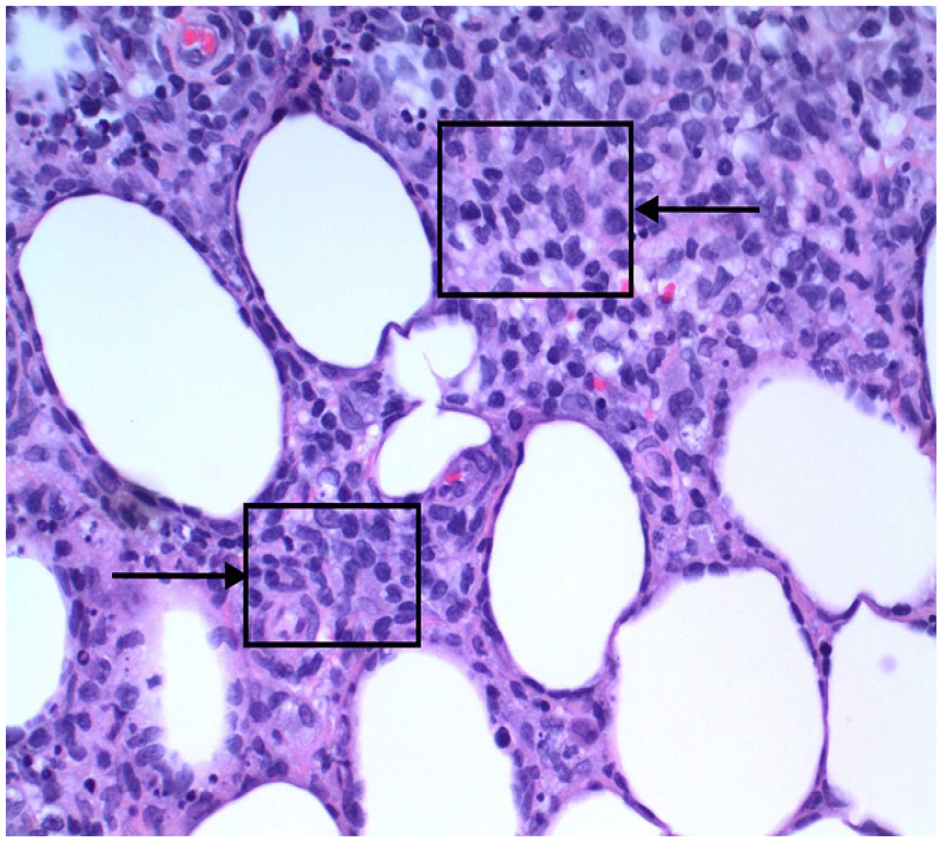
Although a provisional diagnosis of lipodermatosclerosis was the reason for the referral, another process was suspected, given the atypical proximal anterolateral predominance of the lesions and the lack of venous reflux on duplex ultrasound. She was therefore referred to dermatology. A biopsy revealed infiltration of the lower reticular dermis and subcutaneous adipose tissue (Panel B: H&E, 4×, arrow) with lymphohistiocy-tic inflammation and scattered enlarged, hyperchromatic lymphocytes with prominent CD8+ rimming of lipocytes (Panel C: H&E, 40×, boxes and arrow). Findings were consistent with subcutaneous panniculitis-like T-cell lymphoma (SPTCL).
SPTCL is an uncommon form of cutaneous lymphoma involving lymphocytic invasion primarily of the subcutaneous tissue. The disease typically presents as one or more erythematous subcutaneous plaques of the lower extremities. Less common presentations involve ulcerative lesions and distribution on the upper extremities, trunk, and head.1,2 Differential diagnosis includes morphea, lipodermatosclerosis, and the full spectrum of panniculitides. Approximately 20% of SPTCL cases are associated with autoimmune disease, most commonly lupus erythematosus.3,4
SPTCL has a good outcome with a 5-year overall survival rate of over 80%. 4 Systemic corticosteroids alone have shown success in limited disease.1,4 Extensive or refractory cases can be treated with systemic chemotherapy. 1
This dermatologic manifestation mimics a vascular manifestation in a patient who underwent unnecessary venous interventions. We show the importance of pursuing nonvascular etiologies for these atypical clinical findings, and of collaborating accordingly. Although other case reports have been published on SPTCL, we herein highlight the potential of misdiagnosis as lipodermatosclerosis by vascular specialists.
Footnotes
Note - Images are in color online.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.