
Abstract

The transient perivascular inflammation of the carotid artery (TIPIC) syndrome, formerly known as idiopathic carotidynia, is a rare vascular disease typically presenting with pain in the area of the carotid triangle accompanied with distinct radiologic features. TIPIC syndrome is characterized by a local inflammation of the surrounding carotid tissue; the underlying pathophysiology is unknown.1,2 Current knowledge of TIPIC syndrome derives mainly from case reports, as larger cohort studies are rare. In 2017, Lecler et al. established diagnostic criteria including the following features: acute pain overlying the carotid artery; eccentric perivascular infiltration on imaging; exclusion of another vascular or nonvascular diagnosis with imaging; improvement within 14 days either spontaneously or with antiinflammatory treatment. 1 Treatment mainly consists of nonsteroidal antirheumatic drugs, with glucocorticoids given infrequently. However, several diagnostic and therapeutic aspects are still unclear. The aim of this study was to investigate the clinical and diagnostic parameters on disease progression as well as outcome data of patients with TIPIC syndrome.
The study was approved by the local institutional review board. An electronic search of patients, who had been diagnosed from 2001 to 2020 with predefined International Classification of Diseases, 10th Revision (ICD-10) codes (G90.0, G90.01, I77.6, I77.8) or with the terms ‘carotidynia’ and ‘TIPIC syndrome’, was performed using the database of a fully electronic patient information system, which is installed in the province of Styria, Austria to provide electronic health data from all public Styrian hospitals and hospital alliances. 3 Every matched patient was individually analyzed by chart review to confirm the diagnosis of TIPIC syndrome and to extract epidemiologic, clinical, diagnostic, and outcome data.
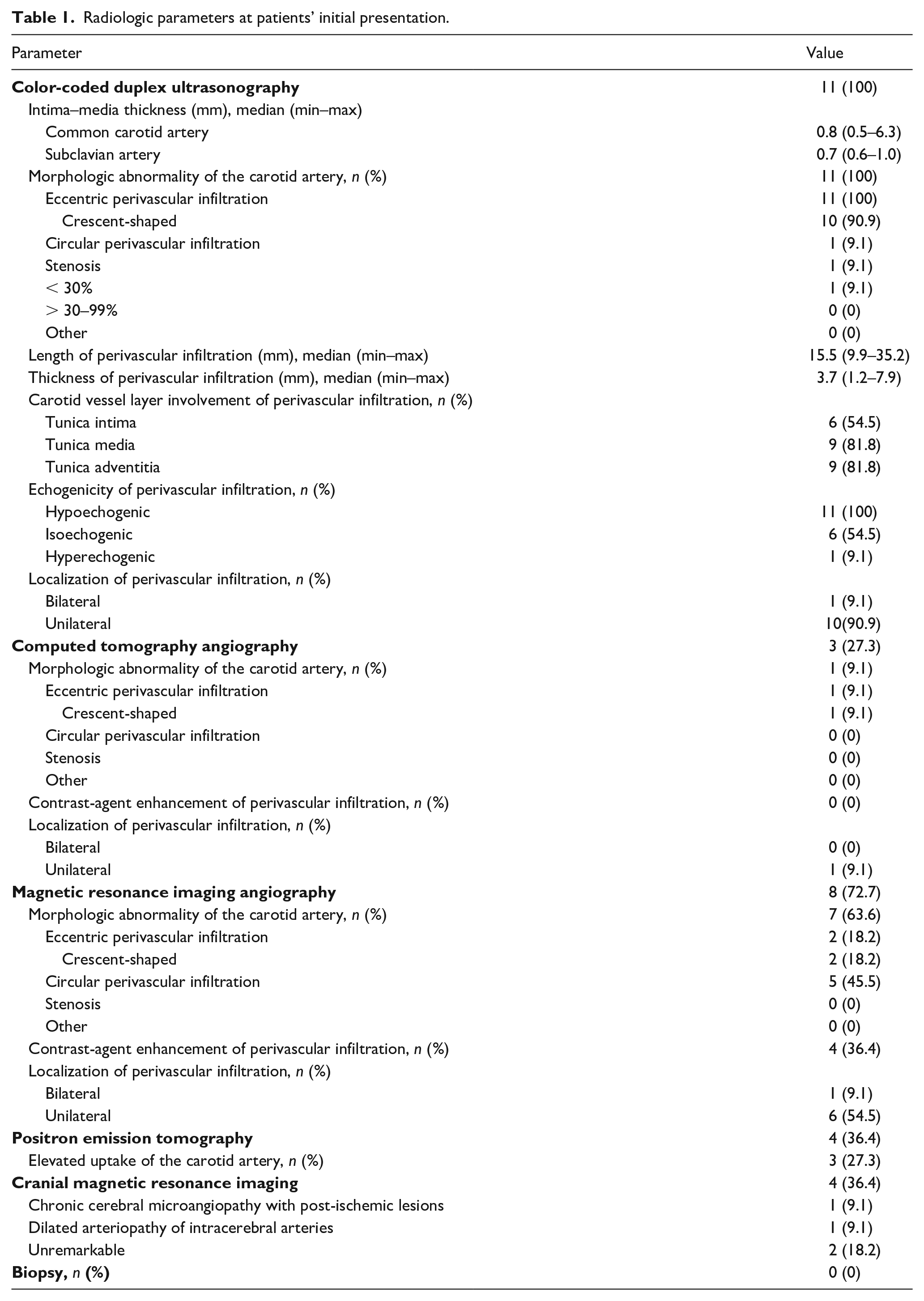
A total of 536 patients were identified by the electronic search using ICD-10 codes and free text diagnoses. After chart review and removal of duplicate patients, a total of 11 patients with idiopathic carotidynia or TIPIC syndrome were included: eight patients fulfilled retrospectively the diagnostic criteria of Lecler et al., two patients fulfilled three criteria, and one patient fulfilled two criteria. 1 Radiologic parameters at initial presentation are listed in Table 1. Otorhinolaryngological examination at initial presentation was performed in six patients, with enlarged lymph nodes detected in three patients but without further abnormalities. All patients with immunosuppressive agents due to initially suspected vasculitis were immediately tapered of their dosages as soon as TIPIC syndrome was definitively diagnosed. Epidemiological, clinical, laboratory, and therapeutic data at the patients’ initial presentation are listed in online Supplemental Table 1.
Radiologic parameters at patients’ initial presentation.
Mean (SD) and median (min–max) follow-up periods of patients with TIPIC syndrome were 44.4 (± 36.5) and 29 (3–100) months. Amelioration of symptoms was present in all patients after a median of 12 (min–max 4–90) days without any reported deterioration of initial symptoms. Complete remission of symptoms was achieved in nine patients after 6 months; two patients reported slight intermittent carotidynia over the whole follow-up period. Sonographic perivascular infiltration was detectable in three patients up to 12 months after initial presentation (online Supplemental Figure 1). In two patients, residual carotid perivascular changes were detected on follow-up magnetic resonance imaging 1 month and 22 months after initial presentation, but no residual carotid perivascular changes were detected by follow-up computed tomography or positron emission tomography. Intermittent slightly elevated C-reactive protein and erythrocyte sedimentation rate were observed up to 1 month after initial presentation in two patients with normal ranges in subsequent follow-up visits. Relapse of TIPIC syndrome was reported in three female patients after 5, 8, and 85 weeks, respectively, and all three patients had a detectable perivascular infiltration on carotid ultrasound. No patient exhibited more than one relapse. None of the patients revealed elevated inflammatory parameters at the time of relapse. All patients presenting with a relapse were treated with glucocorticoids (7.5 mg, 50 mg, and 60 mg, respectively) with consecutive tapering, and diclofenac 75 mg bid was additionally initiated in two patients. Follow-up ultrasound up to 12 months after the relapse revealed residual perivascular infiltration in all patients. One patient developed carotid artery disease with a moderate-grade atherosclerotic stenosis (50%) of the external carotid artery 27 months after diagnosis of TIPIC syndrome. During the follow-up period, no patient required revascularization of the carotid artery and no further cardiovascular events, vasculitis, other autoimmune diseases, neurological disorders, or death have been observed.
Although the present study is limited by a small sample size, demographic and clinical findings of our case series are comparable to other recent studies, but with some differences, such as higher rates of preexisting autoimmune disorders, cardiovascular risk factors, posttraumatic events, or local neck swelling.1,2,4 Additionally, all of our investigated patients had hypercholesterolemia at disease onset. Those findings may support (auto-) inflammatory but also atherosclerotic implications in the development of TIPIC syndrome, as previously reported.1,5–8 Finally, as only one moderate-grade atherosclerotic stenosis of the external carotid artery was observed during follow-up, we assume that TIPIC syndrome is a rather benign vascular disease. Nevertheless, further studies are needed to investigate the pathophysiology, optimal treatment strategies, and outcome of TIPIC syndrome.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231155303 – Supplemental material for Retrospective analysis of long-term clinical, diagnostic and outcome parameters in patients with TIPIC syndrome
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231155303 for Retrospective analysis of long-term clinical, diagnostic and outcome parameters in patients with TIPIC syndrome by Philipp Jud, Jan Struger, Thomas Gattringer, Gerit Wünsch, Marianne Brodmann and Franz Hafner in Vascular Medicine
Supplemental Material
sj-pdf-2-vmj-10.1177_1358863X231155303 – Supplemental material for Retrospective analysis of long-term clinical, diagnostic and outcome parameters in patients with TIPIC syndrome
Supplemental material, sj-pdf-2-vmj-10.1177_1358863X231155303 for Retrospective analysis of long-term clinical, diagnostic and outcome parameters in patients with TIPIC syndrome by Philipp Jud, Jan Struger, Thomas Gattringer, Gerit Wünsch, Marianne Brodmann and Franz Hafner in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.