
Abstract

Arterial stiffness (AS) is a recognized predictor of cardiovascular and all-cause mortality.1,2 AS can be assessed by different noninvasive measurement methods, of which carotid–femoral pulse wave velocity (cfPWV) (the gold standard method) and pulse pressure (PP) are officially recognized. 1 In this context, among modifiable cardiovascular risk factors, cigarette smoking is one of the factors evaluated by several studies. 3 Experimental evidence showed a direct detrimental effect of cigarette smoking on arterial compliance. 4 Despite this evidence, observational studies found no univocal results on chronic and consistent smoking.5,6 These controversial results may be due to the different methods of AS assessment, different features of participants, cross-sectional design or the short duration of observation. Moreover, a recent meta-analysis, including studies with a short length of observation, found that the chronic effect of smoking was not significantly associated with AS. 6 Therefore, the aim of our study was to prospectively analyse the effect of chronic and consistent smoking in respect to never smoking in an 8-year follow-up study in relation to the development of AS, in a relatively large sample of apparently healthy men participating in the Olivetti Heart Study (OHS).
The OHS was an occupational investigation of the male workforce of the Olivetti factories in Southern Italy, and its study procedures have been described previously.7,8 The Ethics Committee of “Federico II” University in Naples approved the OHS study protocol and the participants provided their informed written consent to participate.
Cigarette smoking status at baseline and at follow-up was investigated by a previously validated questionnaire comprising 11 questions. 7 Physical activity level was expressed according to whether the participant habitually engaged in at least 30 minutes per day of aerobic exercise. Regarding alcohol consumption, the participants were classified into two groups: those who consumed at least one glass of wine (or an equivalent amount of other alcoholic beverages) per day, or no alcohol consumption.
The diagnosis of hypertension was defined as systolic blood pressure (BP) > 140 and/or diastolic BP > 90 mmHg. 1 PP was calculated using the following formula: systolic BP – diastolic BP. A PP > 60 mmHg was considered the cut-off value for AS. 1 Body mass index (BMI) was measured according to the formula: weight (kg)/height2 (m). The homeostasis model assessment (HOMA index) was estimated using the formula: fasting plasma insulin [μU/mL] × fasting plasma glucose [mmol/L]/22.5. A HOMA index > 2.77 U was considered the cut-off value for insulin resistance. The estimated glomerular filtration rate (eGFR) was evaluated by the standard formula (CKD-EPI creatinine equation: eGFRcr = 142 × min(Scr/κ, 1)α × max(Scr/κ, 1)–1.200 × 0.9938Age).
To evaluate the net effect of chronic and consistent smoking without confounding of smoking habit changes over the years, we sequentially excluded: (a) participants whose information on smoking habit was not available (n = 49); (b) participants with antihypertensive therapy at baseline and at follow-up (n = 344); (c) participants with AS at baseline (n = 37); and (d) participants who changed their smoking habit (n = 54). Finally, the evaluation of AS risk was performed on 427 participants (smokers and never smokers).
The baseline characteristics of the whole sample, and stratified by smoking habits, are reported in online Supplemental Table 1. For the smokers’ group, the mean pack-years was 7.4 at baseline (median: 8.0 [25th – 75th: 4.0–9.2]) and 6.9 at follow-up (median: 8.0 [25th – 75th: 4.0–8.0]) (p for comparison > 0.05). At baseline, the mean duration of smoking habit was 30 years (median: 30 years [25th – 75th: 27–35]).
The smokers’ group had significantly higher C-reactive protein, and lower body weight, diastolic BP and insulin resistance than the never smokers’ group (online Supplemental Table 1).
At the 8-year follow-up, an overall incidence of AS of 7.3% was detected. The percentage of participants who developed AS was greater in the smokers’ group in comparison with the never smokers (10.5% vs 5.1%, p = 0.036). Moreover, there was a significant increase in weight and BP in the whole sample, though only a significant increase in diastolic BP in smokers than never smokers was found (online Supplemental Table 2). The logistic regression analysis confirmed the significant direct association between smokers and development of AS over time, also after adjustment for main confounders (Table 1). The results were not substantially modified, including changes in body weight over the years, or (systolic or diastolic) BP or diastolic changes over the years, or hypertension status in the models (Table 1).
The 8-year risk of incident arterial stiffening for smokers compared to never smokers (n = 427).
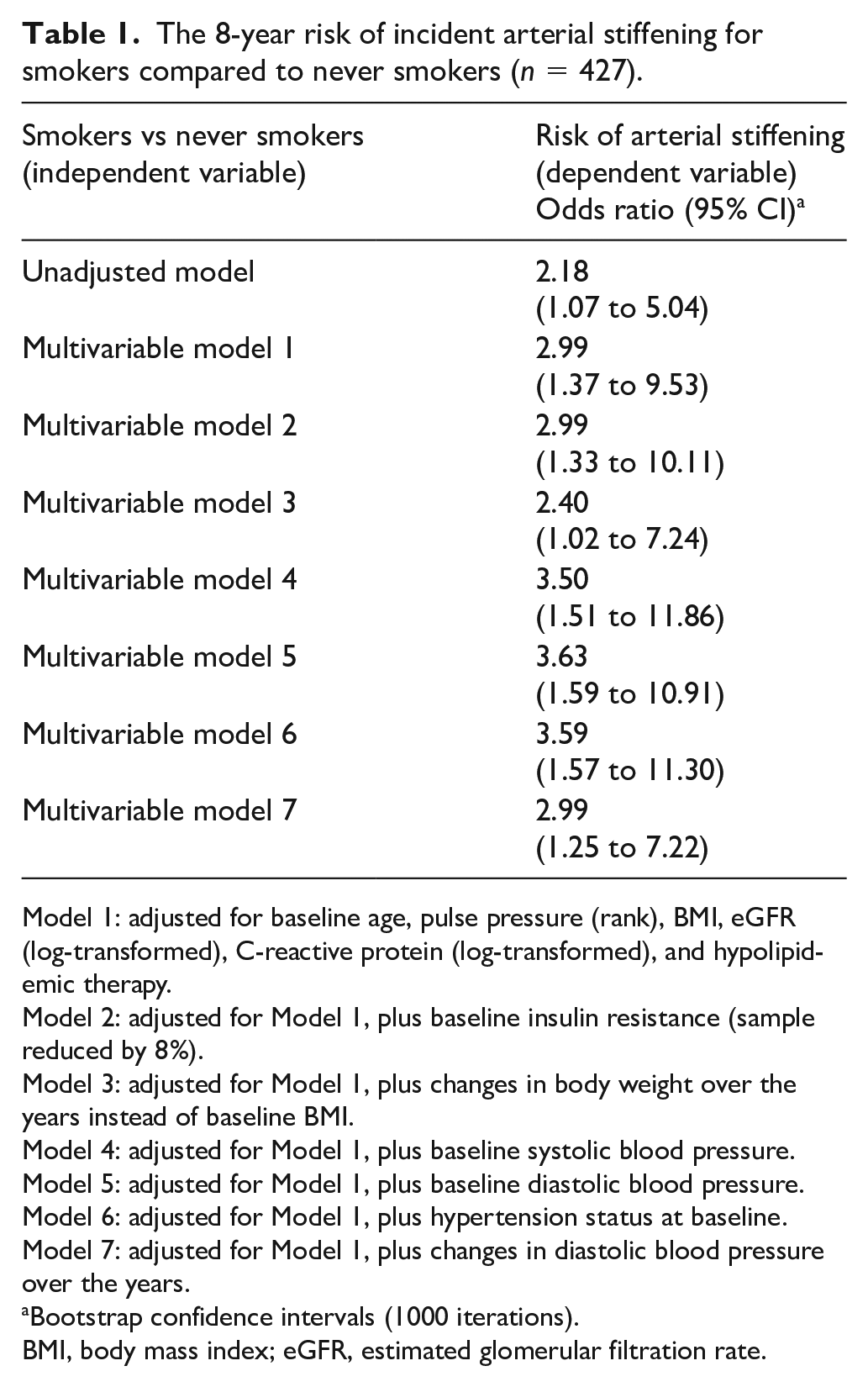
Model 1: adjusted for baseline age, pulse pressure (rank), BMI, eGFR (log-transformed), C-reactive protein (log-transformed), and hypolipidemic therapy.
Model 2: adjusted for Model 1, plus baseline insulin resistance (sample reduced by 8%).
Model 3: adjusted for Model 1, plus changes in body weight over the years instead of baseline BMI.
Model 4: adjusted for Model 1, plus baseline systolic blood pressure.
Model 5: adjusted for Model 1, plus baseline diastolic blood pressure.
Model 6: adjusted for Model 1, plus hypertension status at baseline.
Model 7: adjusted for Model 1, plus changes in diastolic blood pressure over the years.
Bootstrap confidence intervals (1000 iterations).
BMI, body mass index; eGFR, estimated glomerular filtration rate.
Moreover, we carried out separate analyses on the possible relationship between the number of pack-years or duration of smoking habit before the baseline visit and risk of AS, within the group of smokers. The number of pack-years at baseline, at follow-up, and its change during the observation did not affect the risk of AS (p > 0.05). By contrast, there was a significant and direct association between duration of smoking habit before the baseline visit and risk of AS (for 1-year increase, odds ratio: 1.09, 95% CI: 1.02 to 1.16).
To our knowledge, this is the first study directly relating chronic and consistent cigarette smoking to risk of AS, in a middle-aged sample selected from a general population, observed for a reasonably long period. In particular, our results indicate that consistent cigarette smoking is associated with a threefold increased risk of AS than never smokers, independently of potential confounders. Moreover, additional analyses on smokers show that the duration of smoking is directly associated with the risk of AS, with an increased risk of 9% for each 1-year increment. By contrast, the number of pack-years during follow-up does not seem to affect this risk.
This association between smoking and AS is in line with our previous analyses on the development of both hypertension and kidney damage, despite the different selected sample included in this analysis (participants without AS at baseline, and without antihypertensive therapy at baseline and at follow-up). In particular, these results indicate a detrimental effect on the risk to develop vascular damage independently of BP in different settings.
This study has several strengths: (i) the prospective design with the relatively long follow-up period; (ii) the large number of included participants from a general population without AS at baseline and without BP treatment; (iii) the careful standardization of data collection at both baseline and follow-up examination; and (iv) the association between consistent smoking habit and AS, independent of the main potential confounders.
Nonetheless, the study has some limitations: the first one is the participation of only adult white male individuals, which makes our results only generalizable to male Caucasian people.
Next, the assessment of AS by PP may be a limit of the study. Indeed, PP is influenced by the compliance of the large arteries and the stroke volume. However, also in consideration of the prospective design of the study, the contribution of the stroke volume could be neglected in this context. Of note, PP values greater than 60 mmHg are a recognized expression of AS, as well as values of more than 10 m/s of cfPWV, which is the gold standard of AS noninvasive measurement methods, 1 and an important cardiovascular risk factor.1,2 On the other hand, some classes of drugs could affect the relationship between smoking habit and AS, modulating and interacting with organ damage. 9 Notwithstanding this consideration, the risk of AS in our sample seems to be unaffected by therapy.
The association detected in this study significantly adds to the recognized importance of cigarette smoking in cardiovascular risk accumulated through the years. In particular, it can contribute to cardiovascular prevention through supporting the campaign to not start smoking or smoking cessation as early as possible in life. Further studies are needed to support our conclusions and to better clarify the mechanisms involved.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221130378 – Supplemental material for Consistent smoking and development of arterial stiffening in adult men: Results of the Olivetti Heart Study
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221130378 for Consistent smoking and development of arterial stiffening in adult men: Results of the Olivetti Heart Study by Lanfranco D’Elia, Maria Masulli, Roberto Iacone, Ornella Russo, Pasquale Strazzullo and Ferruccio Galletti in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.