
Abstract
Data on the characteristics and outcomes of hospitalized patients with aortic aneurysms (AA) and HIV remain scarce. This is a cohort study of hospitalized adult patients with a diagnosis of AA from 2013 to 2019 using the US National Inpatient Readmission Database. Patients with a diagnosis of HIV were identified. Our outcomes included trends in hospitalizations and comparison of clinical characteristics, complications, and mortality in patients with AA and HIV compared to those without HIV. Among 1,905,837 hospitalized patients with AA, 4416 (0.23%) were living with HIV. There was an overall age-adjusted increase in the rate of HIV among patients hospitalized with AA over the years (14–29 per 10,000 person-years; age-adjusted p-trend < 0.001). Patients with AA and HIV were younger than those without HIV (median age: 60 vs 76 years, p < 0.001) and were less likely to have a history of smoking, hypertension, dyslipidemia, diabetes mellitus, and obesity. Thoracic aortic aneurysms were more prevalent in those with HIV (37.5% vs 26.7%, p < 0.001). On multivariable logistic regression, HIV was not associated with increased risk of aortic rupture (OR: 0.79; 95% CI: 0.61–1.01, p = 0.06), acute aortic dissection (OR: 0.73; 95% CI: 0.51–1.06, p = 0.3), readmissions (OR: 1.04; 95% CI: 0.95–1.13, p = 0.4), or aortic repair (OR: 0.89; 95% CI: 0.79–1.00, p = 0.05). Hospitalized patients with AA and HIV had a lower crude mortality rate compared to those without HIV (OR: 0.75 (0.63–0.91), p = 0.003). Hospitalized patients with AA and HIV likely constitute a distinct group of patients with AA; they are younger, have fewer traditional cardiovascular risk factors, and a higher rate of thoracic aorta involvement. Differences in clinical features may account for the lower mortality rate observed in patients with AA and HIV compared to those without HIV.
Introduction
With advances in antiretroviral therapies (ART), life expectancy for people living with HIV has significantly increased.1,2 This increase in longevity has been associated with a greater incidence and burden of cardiovascular diseases (CVD). 2 The main characteristics of atherosclerosis among individuals living with HIV include endothelial dysfunction and chronic inflammation. 3 Clinically, in a systematic review and meta-analysis on the global burden of atherosclerotic cardiovascular disease in HIV, Shah et al. reported a twofold increase in risk of cardiovascular diseases compared to the general population. 4 However, there are limited studies on the association of HIV with other vascular diseases, with most studies highlighting the increased risk in peripheral arterial disease, which increases with higher viral load and lower CD4 counts.5,6 We recently reported larger aortic root and ascending aorta diameters among HIV seropositive men compared to HIV seronegative referents. 7 Recent analysis of a prospective cohort from Copenhagen showed a fourfold increased risk of aortic aneurysms (AA) among people living with HIV compared with HIV seronegative cohort participants (OR: 4.51; 95% CI: 2.56–8.08, p < 0.001). 8 Given the higher prevalence of AA with advancing age and the increased longevity of people living with HIV, it would be expected that the incidence of AA will subsequently increase in this population.8,9 Moreover, advancing age is an independent risk factor for aortic rupture and mortality. 10 Nevertheless, studies on patients living with HIV and AA have been limited to case series and little is known about the rate of hospitalization, clinical profile, inpatient outcomes, and types of surgical repair rate of people living with HIV diagnosed with AA in the United States.
The US National Inpatient Readmission Database (USNRD) was created as a comprehensive repository of information to facilitate investigation of correlates of hospital admissions and readmission across the US. We used USNRD to determine the hospitalization rate of HIV in patients with AA, and compare the clinical characteristics and outcomes of aortic aneurysms in patients with and without HIV. We hypothesized that patients with AA and HIV will have different risk factors (smoking, dyslipidemia, hypertension, diabetes mellitus, etc.) and worse clinical outcomes (aortic rupture, hospital readmission, and death) than those without HIV.
Methods
Data source and study population
We utilized the USNRD created as part of the Healthcare Cost and Utilization Project (HCUP) – the USNRD is a subset of large inpatient databases for the HCUP. An added benefit to the NRD is its ability to study both primary index admissions and readmissions for other reasons. The NRD provides records of hospitalization discharges from 30 states in the US, which accounts to around 60% of the total US hospitalizations. Analysis from the NRD can be utilized to study various kinds of admissions and readmissions based on regions, states, or specific types of hospitals (urban vs rural hospitals, teaching vs nonteaching hospitals, etc.). 11 The NRD does not capture individual patients but rather provides information for a given hospitalization. It relies on the International Classification of Diseases (ICD) codes to identify comorbidities and procedures performed during each hospitalization. Each patient has an identifier allowing them to be followed across readmissions within the same state. The NRD provides details related to the hospitalization such as length of hospital stay, total charges, patient-specific insurances, discharge disposition, and hospital-level variables such as teaching status and bed capacity.
The NRD is a publicly owned database with no identified patient information, and as such, the study was exempt from institutional board review. 12
AA was defined using ICD-9 codes 441.1, 441.2, 441.3, 441.4, 441.5, 441.6, 441.7, 441.9 and ICD-10 codes I71.1, I71.2, I71.3, I71.4, I71.5, I71.6, I71.8, I71.9.13 –15 (online Supplementary Table 1). Hospitalizations with any diagnosis of AA were identified between the years 2013 and 2019. Hospitalizations with discharges in December were excluded as 30-day readmission information was not readily available. 11 Those with missing variables and outcomes, and patients under 18 years of age, were also excluded. Hospitalizations with a secondary diagnosis of HIV were identified using respective ICD codes. Readmissions were analyzed and causes of 30-day readmissions were described using system-based etiologies. Online Supplementary Figure 1 shows the study population derivation. Out-of-hospital outcomes were not available. The ICD-9/10 codes that were used to identify our study variables and comorbidities are detailed in online Supplementary Table 1.
Statistical analysis
Hospitalizations with AA were divided into those involving people with HIV and those without. Patient demographics, location of aneurysms, and underlying risk factors and comorbidities were compared between groups. Our outcomes included inhospital mortality, incidence of aortic rupture (defined as AA with rupture as the primary discharge diagnosis), incidence of aortic dissection (defined as AA with dissection as the primary discharge diagnosis), rates of aortic repair, and readmission-related outcomes within a 30-day follow-up. Mortality rates for those hospitalized with aortic rupture, aortic dissection, and those who underwent aortic repair were also compared across both patients living with HIV and patients who are HIV-uninfected. Multivariable logistic regression, using variables that are commonly linked to vasculitis and aortic aneurysm rupture, such as cardiovascular risk factors (age, sex, hypertension, diabetes, smoking, dyslipidemia, obesity, history of coronary artery disease, and history of peripheral vascular disease) and common bacterial/viral infections (syphilis and hepatitis B and C), was performed to determine the association of HIV serostatus with outcomes among patients with AA. In addition, multiplicative interaction between age and HIV was performed to adjust for the effect of HIV and age on outcomes.
Categorical variables were expressed as frequency or percentage and continuous variables were measured using median value and IQR. The chi-squared test was used to compare two or more categorical variables, and Fisher’s exact test was utilized if one of the cells contained < five counts. Univariate linear regression was used to assess the difference between two continuous variables. Multivariable logistic regression with backward conditional method was performed to address the association between HIV serostatus and inhospital mortality, aortic rupture, and readmissions. To conduct a trend analysis for categorical variables like annual hospitalizations of AA with HIV, we used a Poisson regression model that included a variable representing the time of the year and adjusted for age. Results were statistically significant for p < 0.05. Statistical analysis was performed using STATA 17 (StataCorp LLC, College Station, TX, USA).
Results
There were 1,905,837 AA hospitalizations between 2013 and 2019, of which 4416 (0.23%) included a diagnosis of HIV. Baseline characteristics of all people hospitalized with AA stratified by HIV serostatus are described in Table 1. On univariate analysis among hospitalized patients with AA, those living with HIV were younger (median [IQR] age in years: 60 [54–67] vs 76 [68–83], p < 0.001) and had higher rates of thoracic (35.4% vs 24.7%, p < 0.001) and thoracoabdominal AA (3.2% vs 1.7%, p < 0.001) compared to HIV-uninfected AA patients. Major cardiovascular risk factors were more common in the HIV-uninfected group who had a higher proportion of smoking (42.6% vs 39%, p < 0.001), obesity (12.6% vs 9.2%, p < 0.001), hypertension (72.5% vs 67.9%, p < 0.001), dyslipidemia (57.7% vs 40.7%, p < 0.001), and diabetes (24% vs 19.3%, p < 0.001), as well as higher rates of peripheral vascular diseases, history of stroke, and coronary artery disease. On the other hand, hepatitis B (4.6% vs 0.2%, p = 0.001), hepatitis C (14.5% vs 1.1%, p < 0.001), and syphilis (1.3% vs 0.02%, p < 0.001) were more common in the HIV seropositive versus HIV seronegative groups. Patients hospitalized with AA and HIV were mostly treated at teaching hospitals (80.4% vs 68%, p < 0.001) and had a higher proportion of Medicaid coverage (19.8% vs 4.0%, p < 0.001).
Baseline characteristics of patients admitted with aortic aneurysm, stratified by presence or absence of HIV.
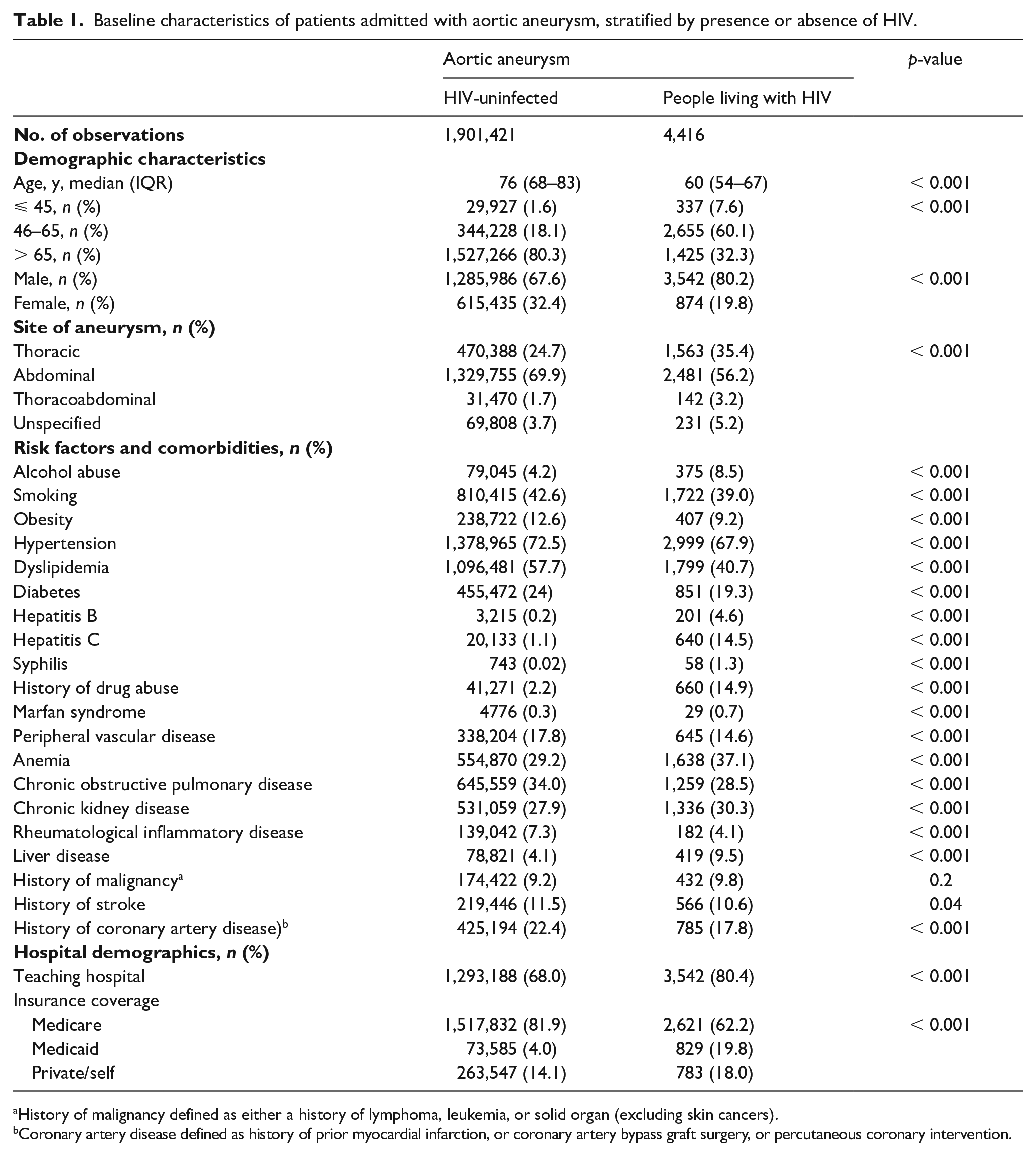
History of malignancy defined as either a history of lymphoma, leukemia, or solid organ (excluding skin cancers).
Coronary artery disease defined as history of prior myocardial infarction, or coronary artery bypass graft surgery, or percutaneous coronary intervention.
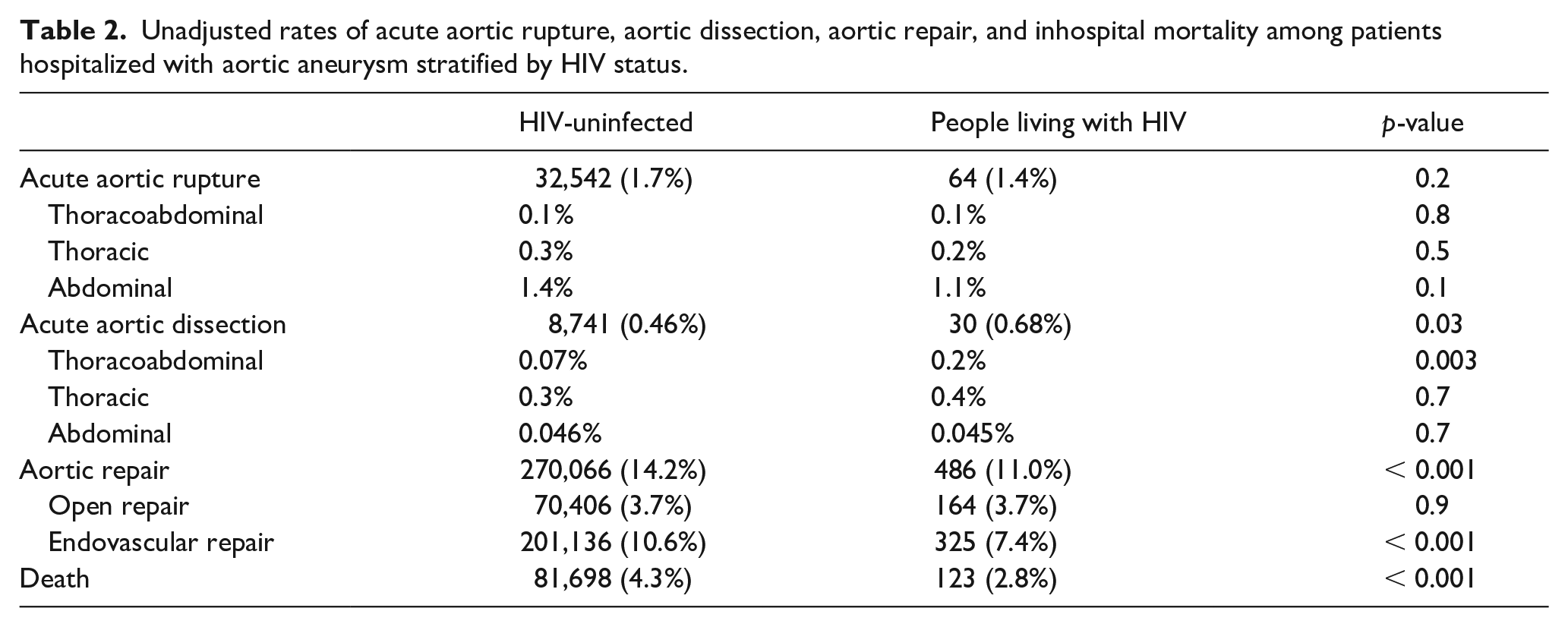
There was a total of 81,698 inpatient hospital deaths among AA patients; moreover, 299,179 were readmitted within 30 days postdischarge. In an unadjusted analysis, patients hospitalized with AA and HIV had lower inhospital mortality (2.8% vs 4.3%, p < 0.001), lower rates of aortic repair (11% vs 14.2%, p < 0.001), but had higher rates of acute aortic dissection (0.68% vs 0.46%, p = 0.03) compared to patients hospitalized with AA without HIV (Table 2). There was no difference in incidence of aortic rupture between HIV seropositive and HIV seronegative patients with AA (1.7% vs 1.4%, p = 0.2), nor in the anatomic distribution of the aortic rupture.
Unadjusted rates of acute aortic rupture, aortic dissection, aortic repair, and inhospital mortality among patients hospitalized with aortic aneurysm stratified by HIV status.
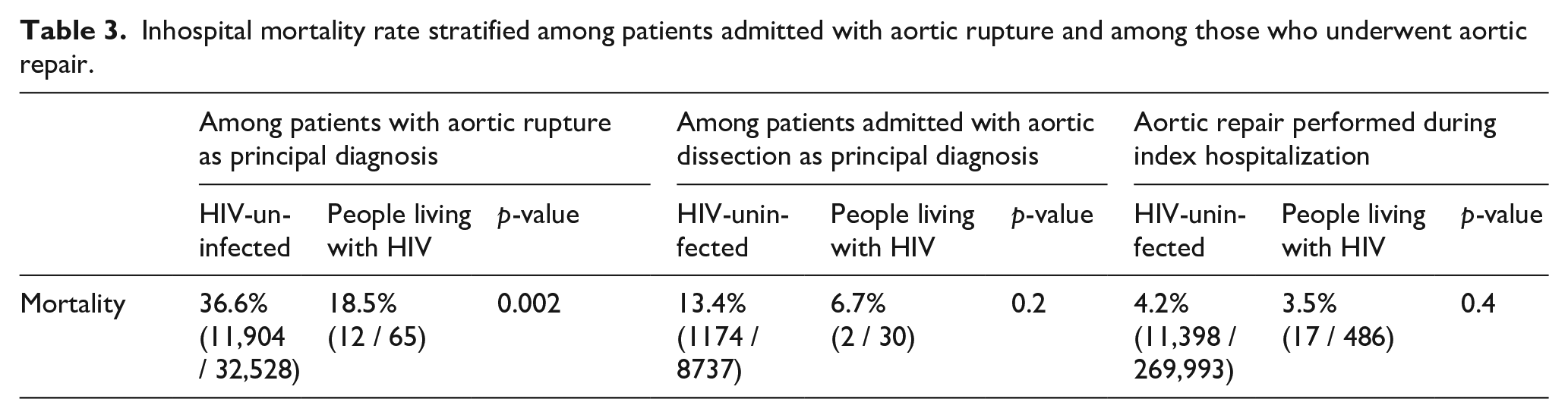
Further subgroup analysis showed that HIV seronegative people hospitalized for aortic rupture had higher inhospital mortality rates compared to those living with HIV (36.6% vs 18.5%, p = 0.002). However, there was no difference in mortality rates between those who underwent aortic repair (HIV seropositive, 3.5% vs HIV seronegative, 4.2%, p = 0.4) or had an aortic dissection (HIV seropositive, 6.7% vs HIV seronegative, 13.4%, p = 0.2) (Table 3).
Inhospital mortality rate stratified among patients admitted with aortic rupture and among those who underwent aortic repair.
When stratified by age groups, there was no difference in the incidence of aortic rupture among those hospitalized with and without HIV, except for a higher rate in HIV seropositive people in the 45–65 years age group (1.4% vs 1.9%, p = 0.045). Those hospitalized without HIV had higher rates of aortic repair across all age groups. However, there was no difference in inhospital mortality rate across all age groups (Figure 1). Online Supplementary Table 2 highlights the demographics and clinical characteristics of patients hospitalized with thoracic and abdominal aortic aneurysms stratified by HIV status.
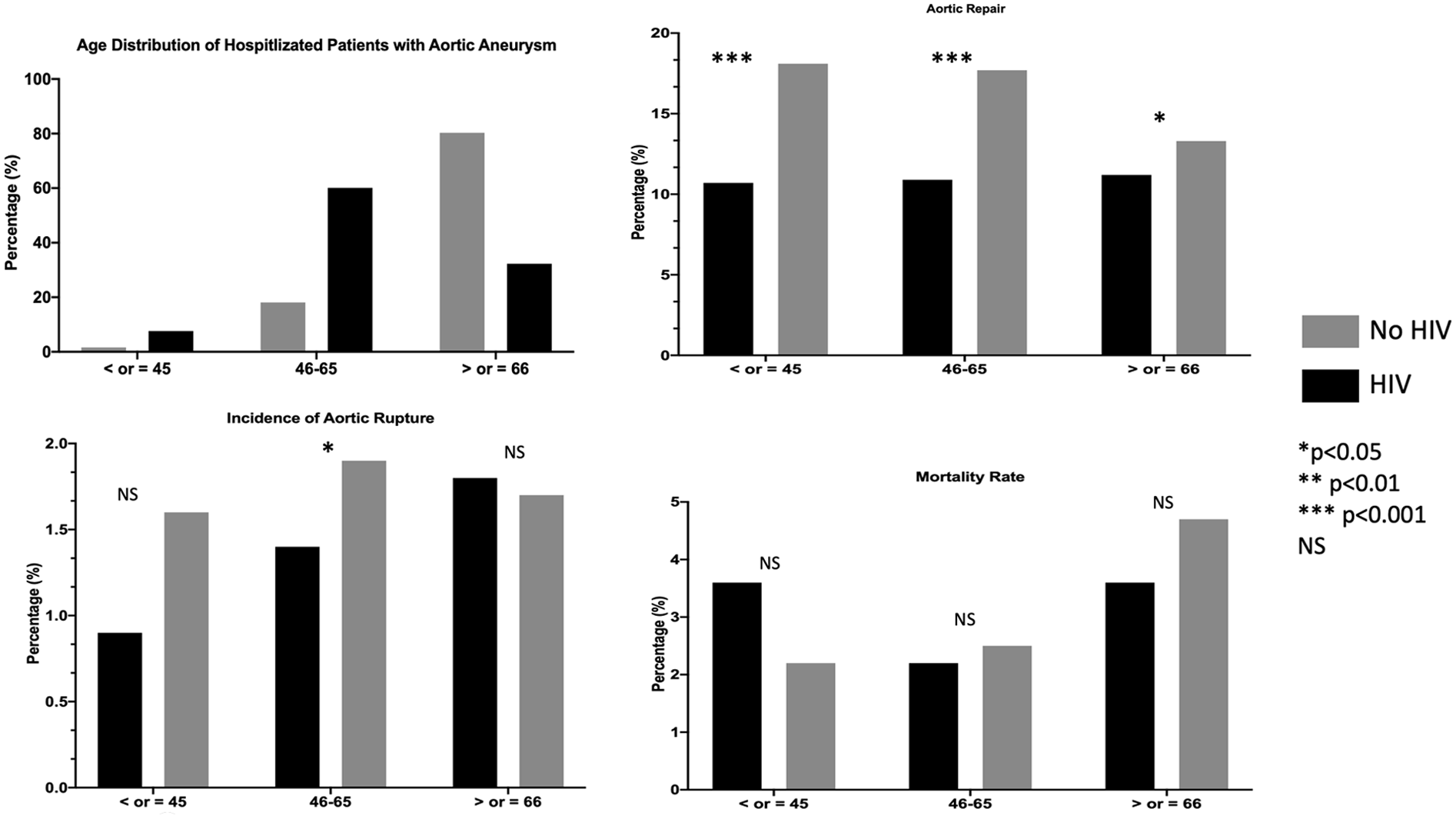
Hospitalization rates and clinical outcomes of patients with aortic aneurysm among HIV-uninfected patients and people living with HIV stratified by age.
In an unadjusted analysis, HIV seropositive patients hospitalized with AA were associated with higher risk of acute aortic dissection (OR: 1.48; 95% CI: 1.03–2.12) but no difference was observed in risk of aortic rupture (OR: 0.84; 95% CI: 0.66–1.08). However, after controlling for age, other covariates, and site of AA, HIV serostatus was associated with neither increased risk of aortic rupture (OR: 0.79; 95% CI: 0.61–1.01, p = 0.06) nor acute aortic dissection (OR: 0.73; 95% CI: 0.51–1.20, p = 0.1). When addressing the association between HIV serostatus and rates of aortic repair, in a univariate analysis of HIV, and after adjusting for age, comorbidities, and site of aortic aneurysm, seropositive patients hospitalized with AA had lower rates of aortic repair (OR: 0.65; 95% CI: 0.59–0.72, p < 0.001). However, this association decreased significantly after adjusting for acute aortic complications and type of admissions (OR: 0.89; 95% CI: 0.79–1.00, p = 0.05). In addition, in an unadjusted and fully adjusted model, patients hospitalized with HIV and AA had lower mortality rates compared to patients without HIV (OR: 0.75; 95% CI: 0.63–0.91, p = 0.003) (Table 4).
Multivariable association between having a secondary diagnosis of HIV and incidence of aortic rupture, aortic dissection, aortic repair, and inhospital mortality.
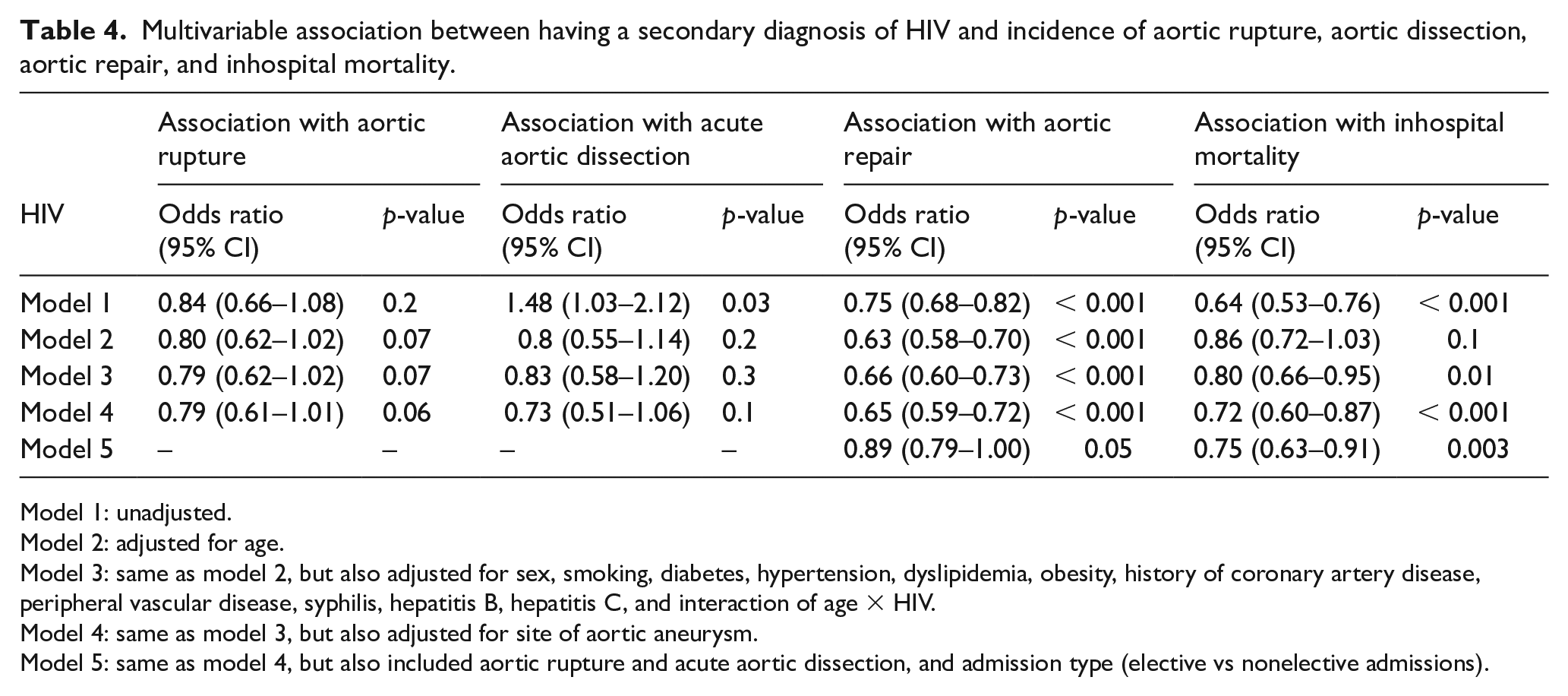
Model 1: unadjusted.
Model 2: adjusted for age.
Model 3: same as model 2, but also adjusted for sex, smoking, diabetes, hypertension, dyslipidemia, obesity, history of coronary artery disease, peripheral vascular disease, syphilis, hepatitis B, hepatitis C, and interaction of age × HIV.
Model 4: same as model 3, but also adjusted for site of aortic aneurysm.
Model 5: same as model 4, but also included aortic rupture and acute aortic dissection, and admission type (elective vs nonelective admissions).
There were 299,179 30-day readmissions among patients with AA. The most common reasons for readmission among those with HIV were cardiovascular-related causes, followed by infectious-related causes (online Supplementary Figure 2). Among HIV seronegative patients, the most common reasons for readmissions were cardiovascular and pulmonary-related causes. There was no significant difference between the HIV seropositive and the HIV seronegative groups in regard to cardiovascular-related causes of readmission (28% vs 32.1%, p = 0.08), but HIV seropositive people had higher infectious-related causes of readmission compared to the HIV seronegative group (18% vs 10%, p < 0.001). On a univariate analysis, having a secondary diagnosis of HIV was associated with a higher rate of AA readmissions, but that association was lost when controlling for confounding variables such as age and traditional cardiovascular risk factors (OR: 1.08; 95% CI: 0.95–1.13) (online Supplementary Table 3).
Finally, with regard to the temporal trend of hospitalizations, there was a twofold age-adjusted increase in the rates of HIV among hospitalized patients with AA from 2013 to 2019 (14–29 per 10,000 person-year; age-adjusted p-trend < 0.001) (Figure 2).
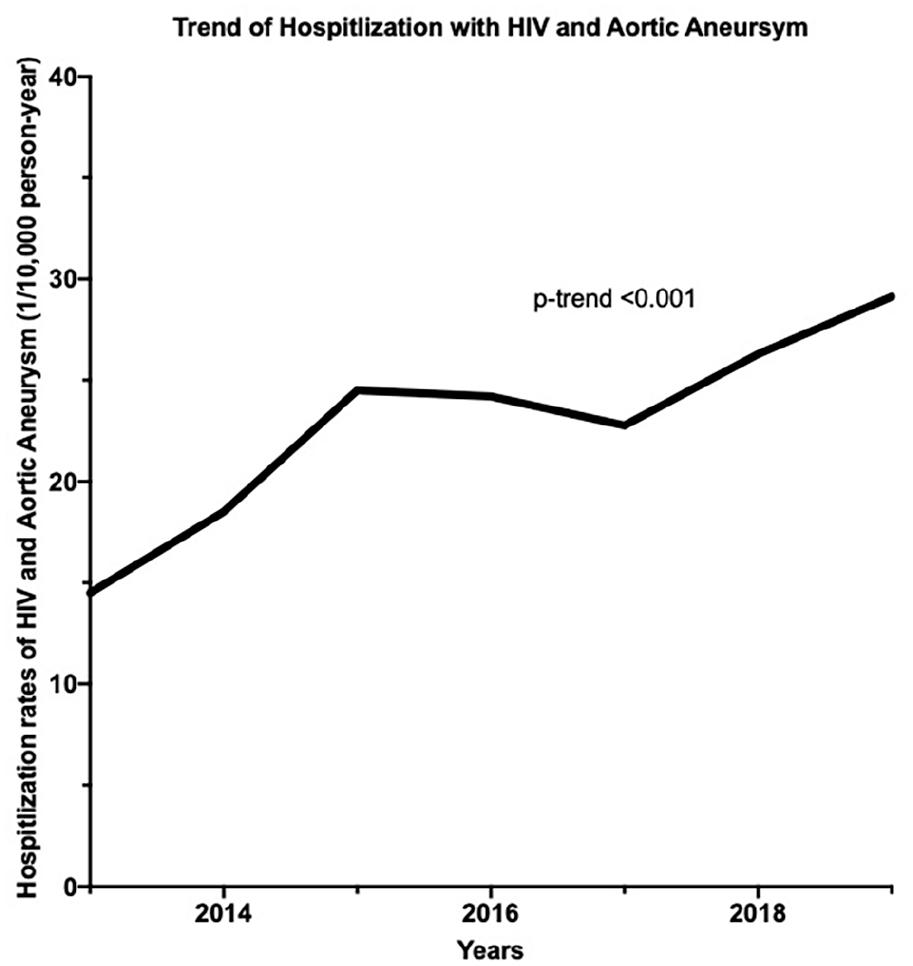
Temporal trend for hospitalizations of people living with HIV and aortic aneurysm.
Discussion
Our study highlights a number of novel findings. We observed an increased rate of HIV among hospitalized patients with AA between 2013 and 2019. Patients with AA and HIV likely constitute a distinct group when compared to those without HIV; they were younger, more likely to have aneurysmal involvement of their thoracic aorta, and had lower rates of traditional cardiovascular risk factors. Outcomes did not markedly differ across groups. In fact, aortic rupture and mortality were slightly higher in the HIV seronegative group; this may be due to the increased prevalence of atherosclerotic cardiovascular diseases and older age in this group.
Several mechanisms have been proposed for the pathogenesis of aortic aneurysms in the setting of HIV infection. Vasculitis is recognized as the hallmark pathologic feature of HIV-associated aneurysms, with several phenotypes reported in the literature. Autopsies from children with AIDS have demonstrated that small and medium-sized arteries are mostly affected, with features of intimal fibrosis, fibrosis and calcification of the media, luminal narrowing, and perivasculitis. 16 Pathology studies in older adolescents and adults have shown a systemic necrotizing vasculitis with lymphocytic infiltration mostly affecting small vessels, and others have shown a peri-arteritic fibroproliferative granulomatous inflammation of the aortic and iliac vessels.17–19 Histology of the aneurysmal wall demonstrated occlusion of the vasa vasorum by an inflammatory cell infiltrate which contributes to weakening of the vessel wall, in the setting of leukocytoclastic vasculitis.17,19 Another mechanism hypothesized to play a role in the pathogenesis of HIV-related aneurysms was molecular mimicry, but Tilson et al. later showed that the viral envelope proteins gp120 and gp41 do not in fact share common ligands with the artery-specific matrix cell adhesion molecule-1 (Mat-CAM-1) as was previously believed. 20 They additionally hypothesized that the more likely mechanism was a direct infection of arterial matrix fibroblasts by HIV. 20 With regards to coinfections, we found higher rates of hepatitis B and hepatitis C infections in patients with AA and HIV; both hepatitis B and C have been previously associated with aortic pathology in the setting of HIV.8,16,21 Syphilis coinfection, which we also found to be present in higher rates in hospitalized patients with HIV, has long been recognized as an important contributor to aneurysm development in HIV.17–19 Moreover, patients living with HIV are at increased risk of sustained immunosuppression, thus leading to an inability to remove infectious organisms that might accelerate the development of mycotic aneurysms. 20
We also found that in patients living with HIV, there were higher rates of thoracic and thoracoabdominal AA compared to HIV seronegative patients and higher rates of thoracoabdominal-related aortic dissection, which is consistent with previous studies that reported thoracic aneurysms as the most common anatomical location of involvement.21,22 Consistent with our results, Høgh et al. found that patients with HIV were more likely to have higher rates of ascending AA (30% vs 19%, p = 0.001).
8
Moreover, Subramanian et al. studied the mechanism of arterial inflammation using 18-fluorine-2-deoxy-
In patients hospitalized with AA, there was an increasing rate of HIV as a secondary discharge diagnosis over time (14–29 per 10,000 person-year: p-trend < 0.001). With the advancement of antiretroviral therapies, patients with HIV are living longer; however, this is offset by an increase in incidence of cardiovascular diseases. The increased awareness of various cardiovascular diseases among patients with HIV may have led to greater utilization of multimodality imaging techniques, such as echocardiography and computed tomography, and this might explain the increasing rates of HIV as a secondary diagnosis among those hospitalized with AA.24,25
Cardiovascular, cardiopulmonary, and neurovascular complications of HIV infection are recognized and well described in the literature,2,5,6,26 but evidence of the impact of HIV infection on clinical outcomes in the setting of comorbid conditions remains limited/unknown.21,22,27–29 We found that patients with AA and HIV were not at higher risk of aortic rupture, aortic dissection, aortic repairs, inhospital mortality, or readmissions. In addition, on a univariate analysis we found that patients with HIV were less likely to undergo aortic repair compared to those without HIV. However, after adjustment for admission type (elective vs nonelective) and acute aortic complications, there were no differences in the rates of aortic repair. This highlights that patients with HIV are less likely to undergo elective repair compared to those without HIV.
Additional interesting findings from our analysis were a lower rate of endovascular repair in HIV patients compared to those not living with HIV (7.4% vs 10.6%, p < 0.001) but no difference in the rate of open aortic repair (3.7% vs 3.7%, p = 0.9). To our knowledge, no study has evaluated the best surgical management (endovascular vs open repair) for AA among patients living with HIV. Studies on surgical outcomes have been limited to case reports and case series. 21 Currently, patients living with HIV and aortic aneurysms are managed according to the society for vascular surgery practice guidelines.30,31 However, there is no mention of differences in the surgical management of patients living with HIV and aortic aneurysms. Taking an endovascular approach to the surgical management of patients with AA and HIV is appealing to both the surgeon and the patient as it might be associated with a lower operator exposure to HIV transmission risk and is considered a less invasive approach in patients with complicated comorbidities.21,31,32 Nevertheless, endovascular aneurysm repair (EVAR) is associated with a greater need to undergo additional procedures, poses an increased risk of aortic rupture, and graft infection.33,34 Moreover, patients diagnosed with HIV and AA are younger. In an era of significant improvement in the life-expectancy of patients living with HIV, an open surgical repair might be a better long-term solution. 21
Previous case reports and case series have identified HIV-specific risk factors associated with worse outcomes. For example, low CD4 counts have been associated with higher odds of aneurysm rupture and mortality 20 and higher rates of postoperative complications after surgical repair.21,35 Interestingly, high viral load has been consistently shown not to be associated with the development of aneurysms or worse outcomes.17,21 Data on the contribution of antiretroviral therapy have been mixed, as ART has been shown to be associated with higher odds of CVD, but not with AA prevalence.8,36 Nevertheless, the literature on the effect of HIV infection on aortic rupture and dissection among those with AA is scarce and is based on case reports and case series. 21 Regarding aortic dilatation, however, a recent prospective epidemiologic study by Minhas et al. among 653 men living with HIV in the community from the MACS (Multicenter AIDS Cohort Study), showed a significantly larger aortic diameter at the levels of the aortic root and ascending aorta relative to HIV seronegative controls enrolled as participants in the same study. Moreover, patients with lower CD4 counts had significantly larger aortic dimensions; however, the prevalence of AA (> 5 cm) was relatively low at 0.15%. 7 In addition, similarly to Høgh et al. 8 and Subramanian et al., 23 viral load was not associated with increased aortic diameter.
Study limitations
The NRD database lacks variables of interest such as patient race, medications, CD4 T-cell counts, and HIV viral loads. Information on aortic dilatation rate and diameter were also not available. This plays a vital role in the decision time for surgical intervention. Whether HIV is associated with progression of aortic size diameter or complex aortic anatomy would warrant further prospective studies, which might explain the differences in rates of aortic repair. Our analysis relies on ICD-9/10 codes and is susceptible to coding errors. In addition, the NRD database does not provide information regarding time of diagnosis of HIV. Moreover, given this is a cross-sectional study, we could not assess for causation. This was counterbalanced using a large national database that addresses clinically relevant questions in a vulnerable patient population. When addressing outcomes such as aortic rupture or dissection, only hospitalizations with the principal discharge diagnosis were included to confirm that those admitted with aortic dissection or rupture is the main reason of admission and to further minimize selection bias of patients hospitalized for other reasons.
Conclusion
Hospitalized patients with HIV and AA constitute a distinct population of patients with AA. They are younger, have lower rates of traditional cardiovascular risk factors, and are more likely to have thoracic or thoracoabdominal AA. Proper understanding of the mechanisms of AA and their implications on the lives of patients with HIV will allow better care for this patient population as they age. Though outcomes in those with AA and HIV are not worse, further insights into the incidence and pathophysiology of AA in patients with HIV may offer clues on prevention of AA and its associated morbidities.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221122577 – Supplemental material for Association of HIV infection with clinical features and outcomes of patients with aortic aneurysms
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221122577 for Association of HIV infection with clinical features and outcomes of patients with aortic aneurysms by Omar Chehab, Amjad Kanj, Ralph Zeitoun, Tanveer Mir, Irfan Shafi, Mohit Pahuja, Alexandros Briasoulis, Henrique Doria de Vasconcellos, Anum Minhas, Vinithra Varadarajan, Colin Wu, Armin Arbab-Zadeh, Wendy S Post, Katherine C Wu and João AC Lima in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.