
Abstract

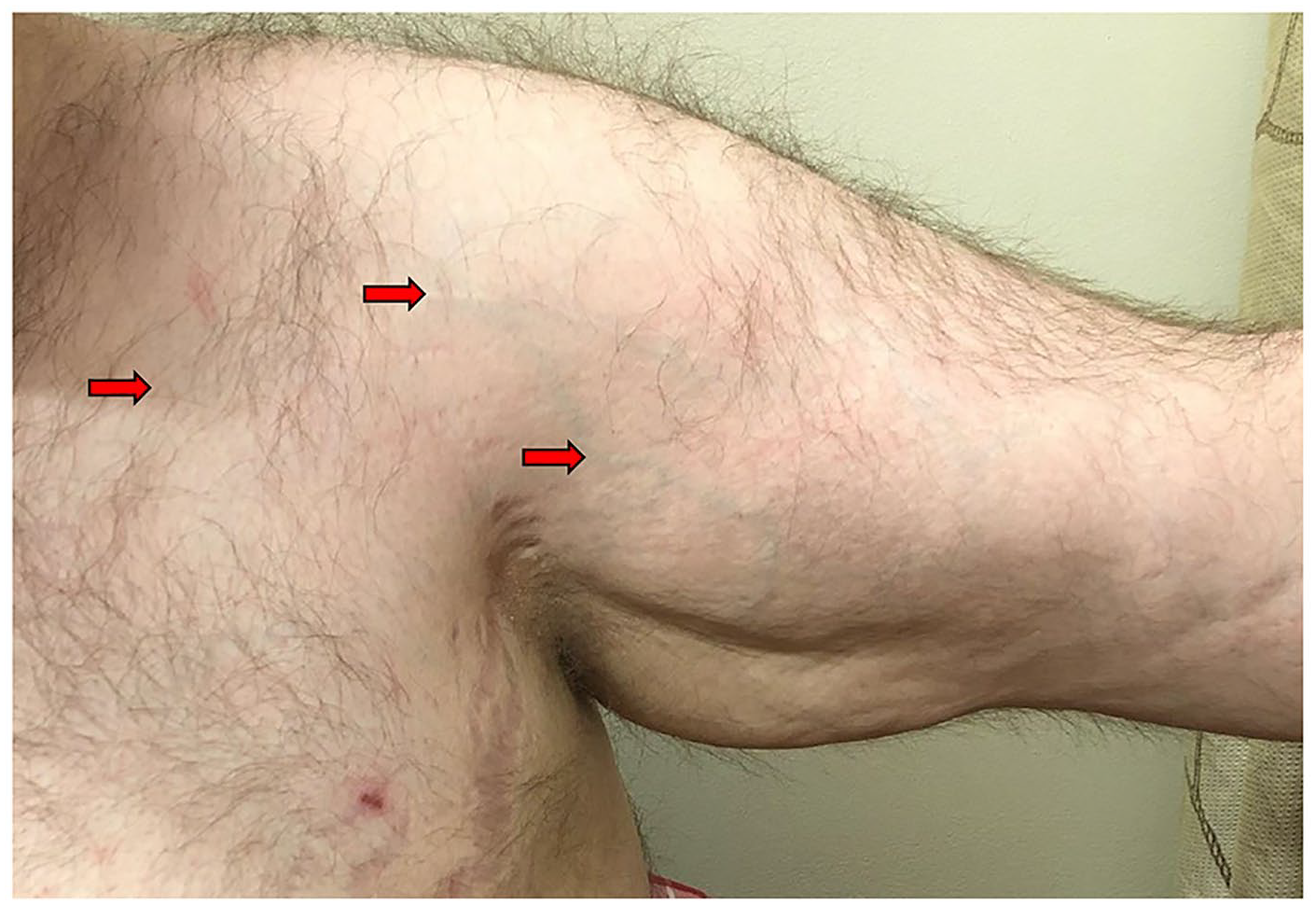
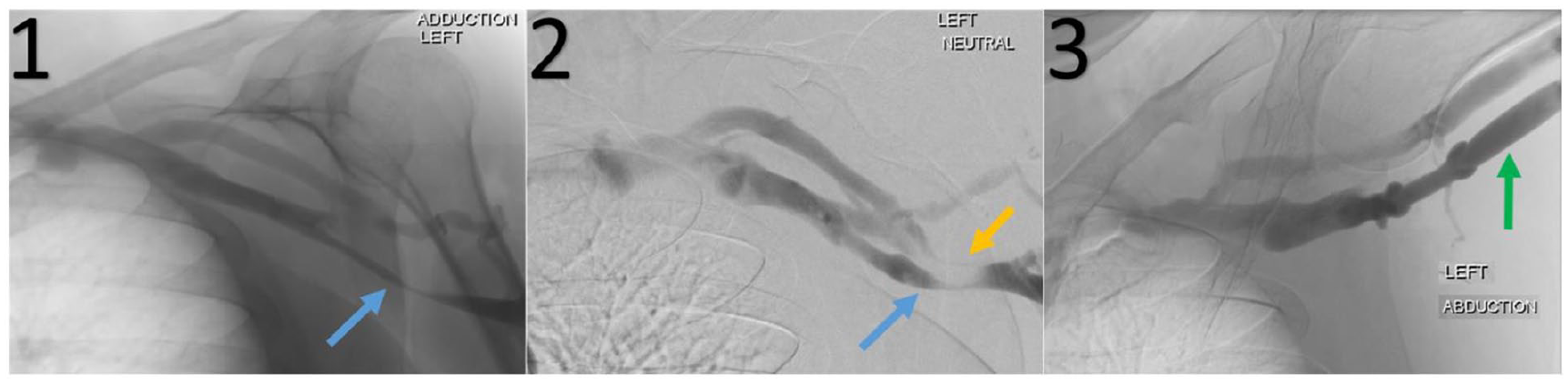
Patient A is a 38-year-old male with left arm pain, swelling, and discoloration for 6 months. Exam was notable for prominent superficial venous collaterals over the left upper arm and shoulder extending into his chest (Urschel’s sign; Panel A, arrows). Symptoms worsened with an elevated arm stress test (EAST) maneuver. Duplex displayed a dampened respirophasic waveform in the left subclavian vein. Venography showed axillary vein obstruction in adducted (Panel B-1, blue arrow) and neutral positions with collateral flow (Panel B-2, blue and yellow arrows). With abduction, axillary vein obstruction was released with improved flow (Panel B-3, green arrow).
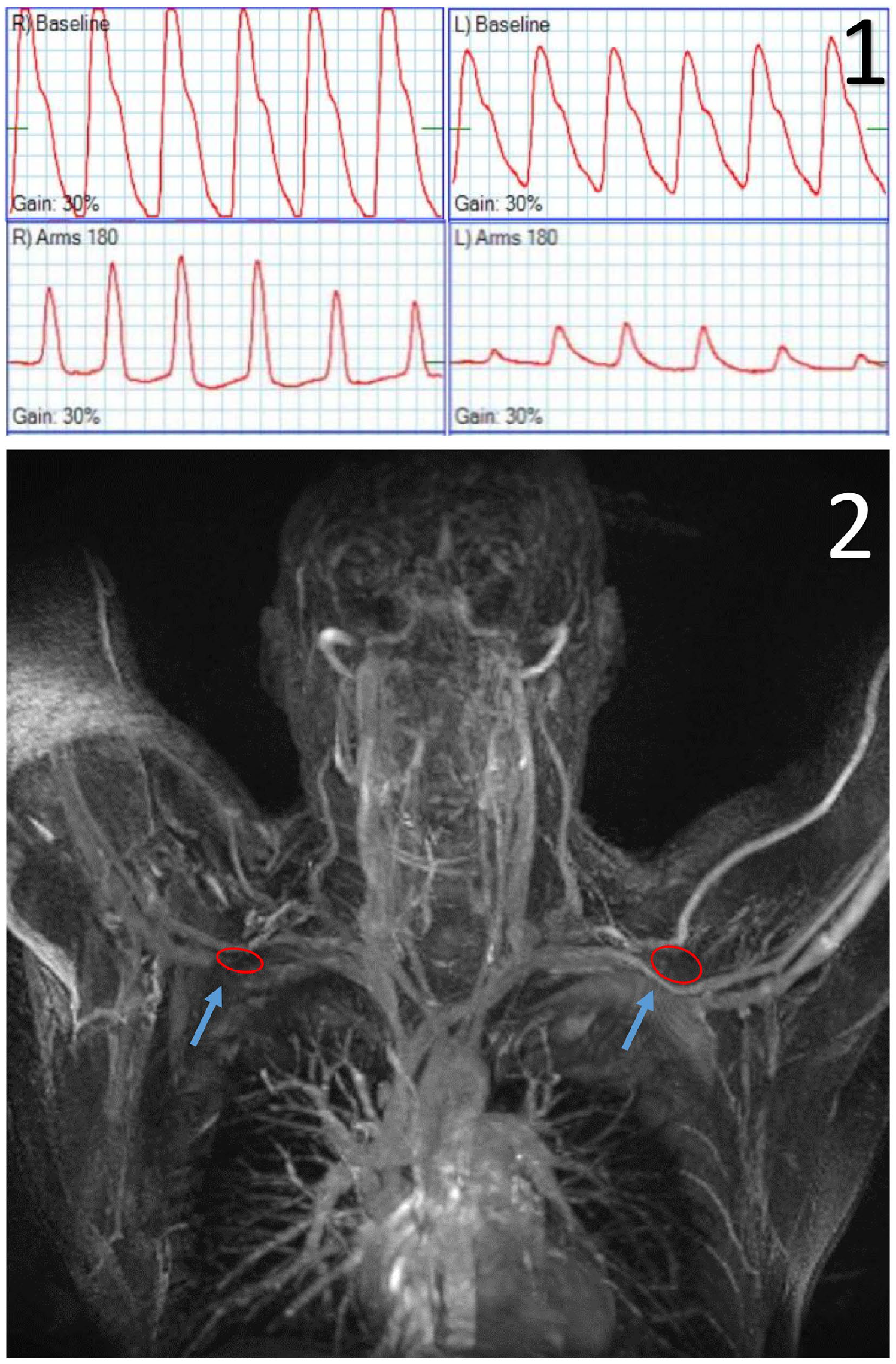
Patient B is a 36-year-old male with progressive bilateral arm erythema and claudication for 1 year. Arm elevation elicited a left subclavian bruit and improved bilateral blanching arm erythema. The EAST maneuver elicited pain in both arms. The wrist–brachial index (WBI) showed dampened waveforms with both arms in 180 degrees and military positions compared to baseline (Panel C-1). Duplex showed continuous waveforms in subclavian and axillary veins at 90 and 180 degrees. A magnetic resonance venogram (MRV) confirmed focal compression of axillary veins (Panel C-2, blue arrows) by pectoralis minor (PM) muscles (Panel C-2, red ovals).
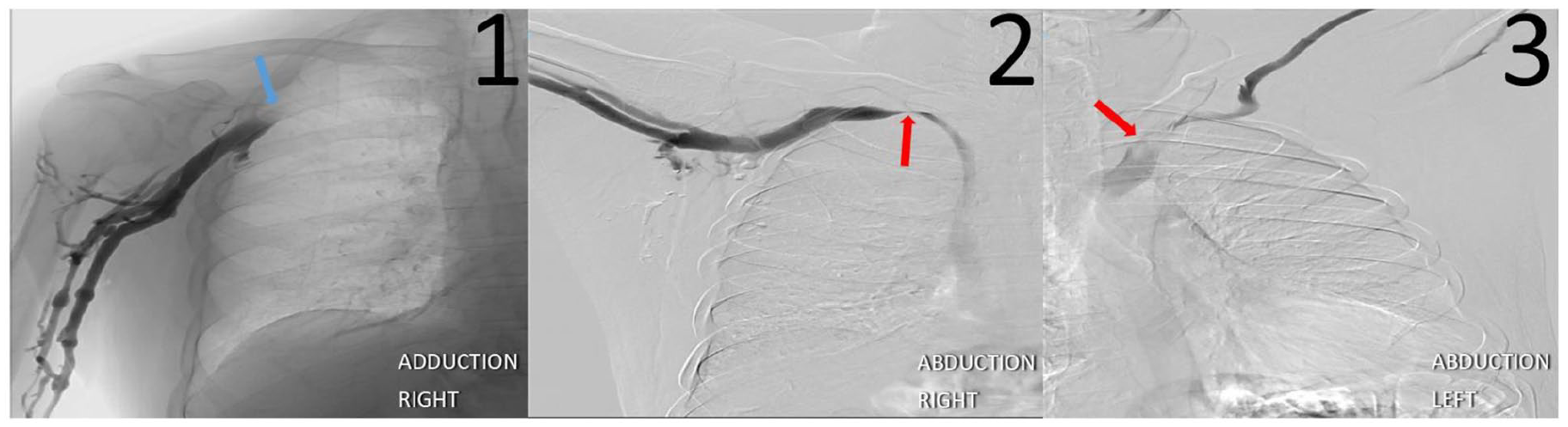
Patient C is a 65-year-old male with bilateral arm paresthesias, erythema, weakness, and swelling that worsened with activity. Exam demonstrated decreased right radial pulse and bilateral subclavian bruits with an EAST maneuver. The WBI showed abnormal right waveforms in the 180 degrees position. Venography showed right axillary/subclavian vein junction stenosis with arm adduction (Panel D-1, blue arrow). Narrowed bilateral subclavian veins at the thoracic outlet on abduction were also noted (Panels D-2 and D-3, red arrows).
Pectoralis minor syndrome (PMS) is a rare condition caused by compression of the axillary neurovascular bundle by the PM muscle. 1 Patients can present with arm/chest pain, paresthesia, weakness, cyanosis, swelling, or a combination of these. 1 Nerve block, WBI with maneuvers, and dynamic venography will often confirm nerve, artery, or vein involvement. About 82% of PMS cases are secondary to trauma and 70% of patients evaluated for neurogenic thoracic outlet syndrome (TOS) also have PMS.1,2
PMS is often thought to be a subset of TOS, but they must be distinguished as treatment for TOS does not relieve symptoms due to compression of the axillary neurovascular bundle. Conservative management with physical therapy can be pursued for those with only neurogenic PMS. Those who fail physical therapy or have vascular compression can be successfully treated with relatively risk-free nerve blocks or PM tenotomies, thereby avoiding more invasive thoracic outlet operations and their potential complications.1–3 Over 90% of patients with isolated PMS have resolution of symptoms with tenotomy, whereas about 35% of patients with PMS and TOS require both tenotomy and thoracic outlet surgery. 2 Patients A and B underwent PM tenotomy with symptom improvement. Management for Patient C is ongoing.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.