
Abstract

Pemberton’s sign is a rare and underrecognized physical exam finding which can be seen in patients with a large goiter. When both arms are elevated above the head at 180°, this provocative maneuver causes facial congestion, cyanosis, and acute distress after a short moment due to compression in the thoracic inlet. Only a few clinical case reports have been published, and radiologic findings have not been well documented.1–5
A 69-year-old female presented with a peculiar complaint that had been present for many years. She felt completely normal when her arms were down. However, with the elevation of both arms above the head, the patient would develop facial redness, congestion, dyspnea, and dysphagia (Panels A-1 and A-2). The patient was referred to the vascular medicine clinic to rule out thoracic outlet syndrome. Past medical history revealed benign goiter with normal thyroid hormone levels under thyroid replacement therapy. Physical exam revealed a large thyroid with questionable retrosternal extension. Upper extremity pulses were equal on both arms with different maneuvers. A flow murmur was auscultated in the right supraclavicular and infraclavicular area when the arms were elevated. A neck computed tomography (CT) angiogram was ordered to rule out thoracic outlet syndrome.

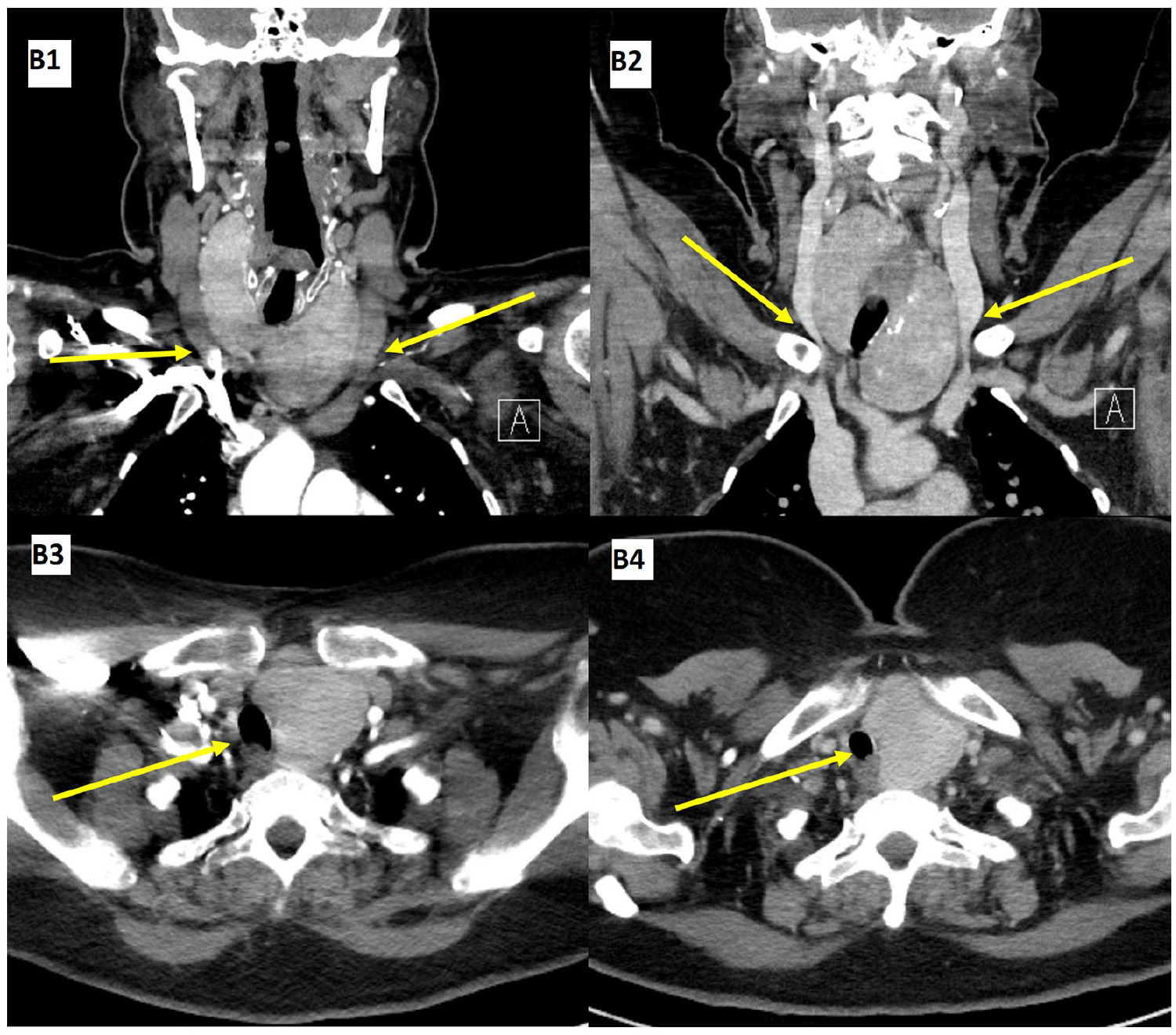
A CT angiogram with the patient’s arms down (Panels B-1 and B-3) and a CT venogram with both arms elevated above the head (Panels B-2 and B-4) were performed. CT demonstrated a markedly enlarged goiter with a subxiphoid component. Both internal jugular veins were severely narrowed and impinged between the enlarged thyroid gland and clavicles at the thoracic inlet, occurring with the arms up (arrows point to internal jugular veins in Panels B-1 and B-2), explaining the facial flushing and congestion. There was also mild to moderate narrowing of the proximal trachea and relatively increased compression of the esophagus when the arms were raised (arrows point to trachea, and esophagus is located immediately posterior to trachea in Panels B-3 and B-4), explaining the dyspnea.
After the radiologic findings, the patient was referred for total thyroidectomy. The patient underwent total thyroidectomy without any complications. Pathology revealed an enlarged thyroid gland with features of Hashimoto’s thyroiditis. No malignancy was identified. Based on a phone interview, the patient’s complaints were resolved entirely following surgery. This case demonstrates radiologic confirmation of clinical Pemberton’s sign, which is severe, reversible compression of the distal internal jugular veins by a large goiter and clavicles when both arms are elevated. Reversible compression of the trachea and esophagus was also visualized, correlating with the patient’s reversible dyspnea and dysphagia. Collaboration between the ordering clinician, the radiologists, and the radiologic technicians was necessary to obtain dual-phase dynamic CT images to confirm the diagnosis.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Acknowledgements
The patient described herein gave full consent for the publication of identifiable details, including photographs, radiologic images, and case history relevant to the purpose of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.