
Abstract

Patients with psoriasis have a higher prevalence of cardiovascular diseases, diabetes mellitus, hypertension, and obesity.1,2 What is more, the course of cardiovascular disease is more severe in patients with more severe psoriasis. 3 Therefore, we present the images of an uncommon case of a young patient with psoriasis suffering from critical lower limb ischemia (CLI).
A 27-year-old, non-smoking male with a history of poorly controlled psoriasis and without other comorbidities was admitted to the Angiology Department due to critical ischemia of the left lower limb. The patient manifested a painful and nonhealing ulcer within the left forefoot (WIfI Scale: W3-I3-fI1; Panel A1). The ankle–brachial index (ABI) values were R: 0.29 and L: 0.42. Laboratory analysis showed a moderately elevated level of serum C-reactive protein (CRP). The glucose level, and kidney and lipid parameters were within the normal range. At admission, color duplex ultrasound of the left leg arteries showed total occlusion of the superficial femoral artery, popliteal artery, tibiofibular trunk, and posterior tibial artery.

The patient was diagnosed with psoriasis 8 years earlier and was treated with moderate methotrexate doses (10–15 mg/week) and phototherapy. Shortly after diagnosis, the first episode of short-distance right-calf claudication appeared. Right popliteal artery catheter-directed thrombolysis was performed. Owing to the recurrence of symptoms, right-sided sympathectomy was performed, resulting only in extended claudication distance. In 2017, the patient reported left lower limb claudication, which was treated by left-sided sympathectomy without any clinical improvement.
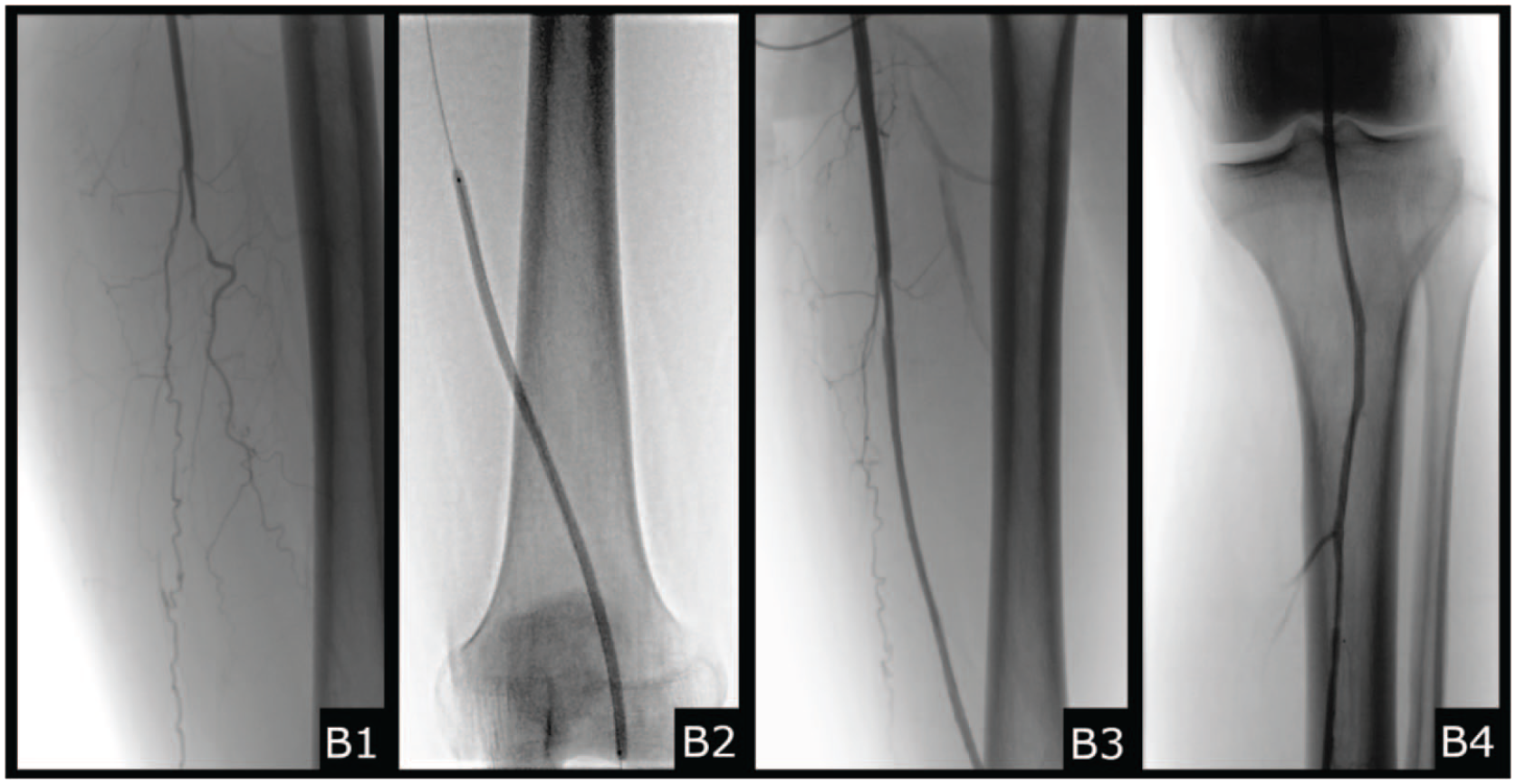
After admission to our ward, we decided to perform recanalization and percutaneous transluminal angioplasty of the left arteries: superficial femoral (SFA), popliteal (PA), tibial posterior (TPA), and tibiofibular trunk (TFT) (Panel B1 shows occluded SFA and PA, B2 shows angioplasty of SFA and PA, B3 and B4 show recanalized SFA, PA, TPA, TFT). This resulted in increased postoperative ABI values (R: 0.3, L: 0.72). We introduced pharmacological treatment: 4 weeks of enoxaparin 60 mg and 6 weeks of clopidogrel 75 mg. Also, acetylsalicylic acid 75 mg and atorvastatin 40 mg for permanent use. Wound debridement and amputation of the distal phalanx of the hallux and the distal and middle phalanges of the second toe were performed.
At 1-month follow-up, there was a significant improvement of ulceration healing (WIfI Scale: W1-I1-fI0; Panel A2). The half-year follow-up revealed complete regression of wounds within the forefoot (W0-I1-fI0; Panel A3), absence of intermittent claudication, limb function recovery, and an improvement in the patient’s quality of life. Doppler ultrasound examination confirmed patency following the endovascular treatment of the arteries.
To the best of our knowledge, this is the first described case of psoriasis-induced CLI in a patient without other cardiovascular disease risk factors or comorbidities. We hypothesize that the ulceration was not an effect of the local psoriasis lesions, but of ischemia caused by psoriasis inflammation affecting vascular endothelium. Owing to the increased risk of cardiovascular disease among patients with psoriasis, peripheral artery disease should not be overlooked during the diagnostic process.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.