
Abstract

A 61-year-old female with stage 4 chronic kidney disease, arterial hypertension, and type 2 diabetes was referred for definitive vascular access creation. Preoperative mapping by Doppler ultrasound (US) revealed extensive atheromatosis affecting both upper limbs. The left cephalic and basilic veins displayed a filiform wave pattern, thus a VA on the left was considered inappropriate for this right-handed patient. On the right, the cephalic vein was undetectable, whereas the basilic vein presented a diameter of 2.5 mm and 4.4 mm, before and after tourniquet compression. The brachial artery had a 3.3 mm diameter and displayed a blood flow volume of 0.09 L/min.
A brachio-basilic fistula was created under local anesthesia, on a program of outpatient surgery. At the fistula completion, a continuous thrill was palpable and a low-frequency bruit was perceived throughout its length.
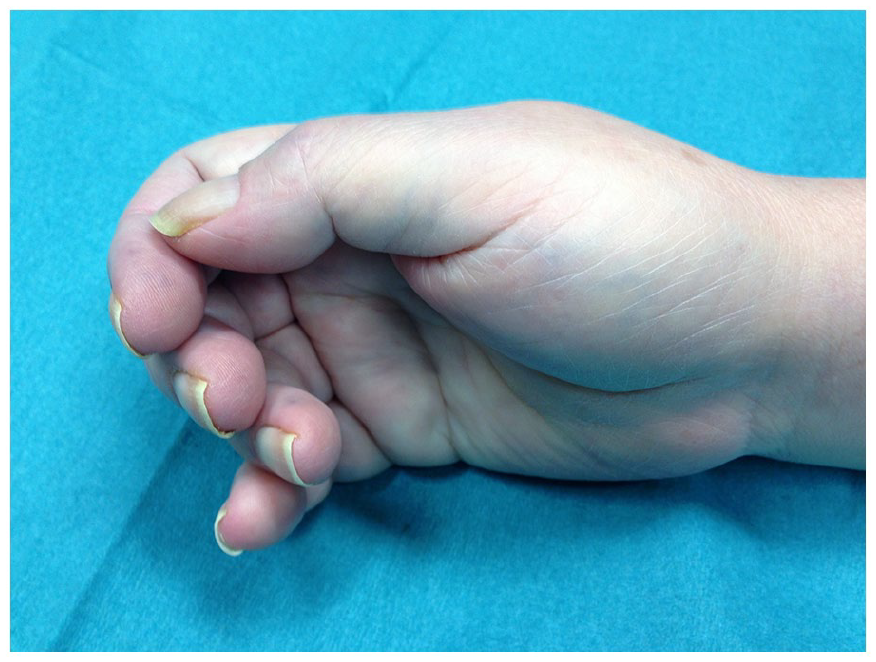
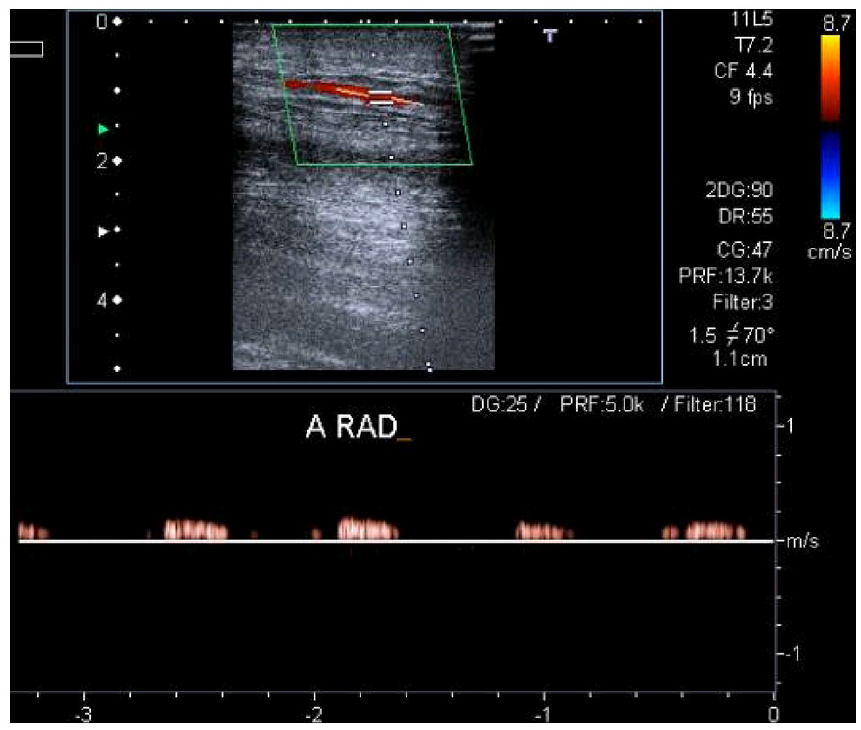
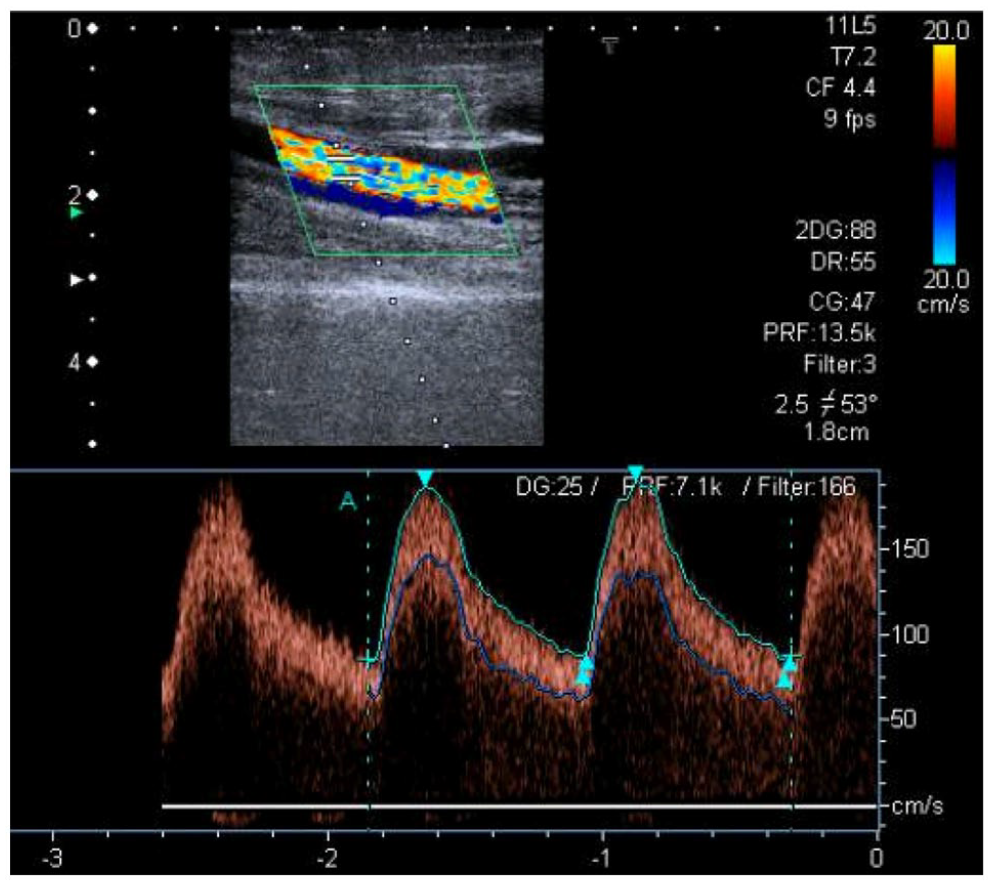
On follow-up 2 days later, the patient reported worsening rest pain, numbness, edema, and weakness of the right forearm; the radial pulse was not palpable. There was no pallor, cyanosis, tenderness, or tightness on deep palpation, nor any signs of local infection (Panel A: patient’s right hand before vascular access ligation). A continuous thrill and low-frequency bruit were still present. Duplex US showed a diminished radial artery waveform (Panel B) and a vascular access flow volume of 900 mL/min, near the upper normal limit (Panel C).
The multidisciplinary team agreed the most plausible diagnosis was monomelic neuropathy and the condition was managed by urgent fistula ligation. The patient immediately experienced relief of pain. Unfortunately, functional disability persisted and, after 6 months of rehabilitation, she maintains chronic pain, muscle atrophy, and weakness (assessment of strength graded 2+ on a scale of 0–5) (Panel D: patient’s right hand showing thenar atrophy [arrow], after 6 months of rehabilitation). Additional vascular access surgical procedures were deemed inappropriate; thus, hemodialysis was initiated after placement of a central venous catheter.

Monomelic neuropathy is a rare complication of vascular access surgery and was first defined by Wilbourn et al. 1 as a severe and potentially irreversible condition caused by ischemic damage of multiple distal nerve groups of a limb, developing within hours. Atherosclerotic and diabetic vascular diseases are important risk factors. 2 Muscle weakness is frequently overshadowed by severe neuropathic pain and allodynia. 3 The hand is typically warm and the radial pulse may or may not be palpable. The diagnosis is clinical in essence, but can be confirmed by numerous studies, 4 including electromyography, pulse volume recordings, and fistulography. Most experts agree that immediate vascular access ligation is required, mainly to increase the prospects of functional recovery.2,4,5
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.