
Abstract
The aim of this study was to analyze the results of infrapopliteal venous and prosthetic bypass surgeries for patients with chronic limb-threatening ischemia (CLTI) and moderate to severe chronic kidney disease (CKD). All consecutive patients undergoing infrapopliteal bypass surgeries at two academic vascular centers between March 2002 and November 2018 were included in this retrospective study. During this timeframe, infrapopliteal grafts were performed for 487 patients. Of these patients, 160 (32.9%; group 1) had normal renal function, 248 (50.9%; group 2) had moderate CKD, and 79 (16.2%; group 3) had severe CKD according to the Kidney Disease Improving Global Outcomes guidelines. After 5 years’ follow-up, the primary patency rate was 46.0% and the secondary patency rate was 54.9% without statistical significance noted between the CKD groups. Limb salvage (65.3%, p = 0.024) and long-term survival (19.6%, p < 0.001) were considerably lower in patients with severe CKD. In subgroup analysis, vein grafts had significantly better long-term patency rates compared to prosthetic grafts, regardless of CKD group. However, in patients with severe CKD, patency rates of vein and heparin-bonded expanded polytetrafluoroethylene (HePTFE) grafts were comparable at the 1-year mark. Our study shows that autologous vein grafts remain the first choice for infrapopliteal bypass surgeries in patients with CKD. HePTFE grafts showed good short-term results in patients with severe CKD. Given the short life expectancy of these high-risk patients, prosthetic HePTFE grafts may be reasonable in this population if a suitable vein is absent.
Keywords
Introduction
Chronic kidney disease (CKD) adversely affects the outcome of therapy for lower extremity peripheral artery disease (PAD), especially in patients with critical limb-threatening ischemia (CLTI) and end-stage renal disease (ESRD).1–3 Surgical revascularization is a therapeutic option for these patients, who are often characterized by diffuse atherosclerotic disease frequently involving infrapopliteal vessels, impaired immunity, susceptibility to infection, and poor wound healing. 3 For these patients, previous studies have demonstrated the benefits of autologous vein grafting, compared to prosthetic conduits, in terms of patency rates and limb salvage after lower extremity bypass.1,4,5 However, these studies mainly focused on patients with ESRD who underwent a variety of different lower extremity bypass surgeries, and they compared the autologous vein with expanded polytetrafluoroethylene (PTFE) bypass grafts.
Heparin-bonded PTFE (HePTFE) grafts have already proven their durability in femoropopliteal bypass surgery in both of the positions above the knee and below the knee. 6 Some authors have also reported encouraging results for HePTFE in the infrapopliteal position in the absence of a suitable autologous vein. 7 However, the role of HePTFE for patients with various degrees of CKD remains unclear. Furthermore, there is a lack of information about the long-term outcomes of infrapopliteal HePTFE grafts for patients with CKD. The aim of our study was to analyze and compare the outcomes of venous, PTFE, and HePTFE tibial and peroneal bypasses for patients with normal renal function or moderate to severe CKD, in terms of the outcome measures of patency, limb salvage, and patient survival.
Methods
Data collection and ethical considerations
In this retrospective study, an analysis of all patients undergoing tibial and peroneal bypass surgery from March 2002 to November 2018 at two academic vascular centers was performed. Data were generated from a prospectively compiled database. Data evaluation was performed by one of the two principal investigators (TB and WS) and was reviewed by the second principal investigator (WS). The data collected is shown in the appendix and included patient demographics, preoperative risk factors, procedural details, postoperative complications, and follow-up information. Patient consent was not required and so it was not obtained because only de-identified data were used. The study was approved by the local ethics committee prior to data collection in accordance with the Declaration of Helsinki (University Medical Center Regensburg approval numbers 14-101-0017 and 20-1697-104).
Study criteria
The indication for treatment was CLTI in all the cases. CLTI was defined as rest pain or tissue loss persisting for more than 2 weeks (Rutherford class 4–6). 8 Based on angiographic findings, each case was discussed by an interdisciplinary board of vascular specialists (vascular surgeons, angiologists, and interventional radiologists) to determine which procedure (endovascular therapy or bypass surgery) would be the first-line therapy. Patients with acute embolic or thrombotic occlusions, graft infections in addition to sequential bypasses, and those who had undergone bridge bypass surgeries (infrapopliteal bypass where a short segment of vein grafts were used to bridge two crural arteries) 9 and composite bypass surgeries consisting of autologous and prosthetic conduits were excluded from the analysis.
Risk factors and chronic kidney disease (CKD) staging
The preoperative risk factors included age, sex, diabetes mellitus, hypertension, coronary artery disease (CAD), cerebrovascular disease, active tobacco use, hyperlipidemia, and renal function. Baseline preoperative creatinine, age, sex, and race were used to calculate the estimated glomerular filtration rate (eGFR) for each patient. The patients were assigned to standard CKD classes according to the Kidney Disease Improving Global Outcomes (KDIGO) Clinical Practice Guidelines for the Evaluation and Management of CKD. 10 For comparative analysis, patients were classified into three groups:
Group 1: patients with normal renal function characterized by an eGFR > 90 mL/min/1.73 m2.
Group 2: patients with moderate degrees of CKD, denoted as CKD classes 2–3, with an eGFR of 30–89 mL/min/1.73 m2.
Group 3: patients with severe CKD, denoted as CKD classes 4–5, with an eGFR < 30 mL/min/1.73 m2, including those on dialysis.
Surgical procedure
Autologous veins were the preferred type of conduit graft. All the patients underwent a clinical examination and duplex ultrasound for vein mapping. The diameter of the vein was measured at the proximal thigh and distal calf using a high-tourniquet. 11 For the patients on dialysis, vein mapping was performed on nondialysis days. 12 In the majority, a greater saphenous vein (GSV) was used. A small saphenous vein (SSV) or arm vein was used whenever the GSV was not available. Prosthetic grafts were only used if an adequate vein was absent (diameter < 3 mm) or if more than two vein segments were needed to achieve a sufficient graft length. The prosthetic grafts used consisted of either PTFE in one center or HePTFE (PROPATEN; WL Gore & Associates, Inc., Flagstaff, AZ, USA) in the other. The surgical procedure was performed using standard techniques. The peroneal artery was always exposed using a medial approach. Before clamping, the patients received 5000 IU of heparin intravenously. When vein grafts were used, proximal anastomosis was performed first. All the prosthetic grafts were ring-enforced with a diameter of 6 mm. Grafts with preformed cuffs, patches, or arteriovenous fistulas at the distal anastomotic sites were not used. Before leaving the operating room, an angiography was performed to exclude technical failures. All the patients underwent clinical examinations and duplex ultrasounds before discharge.
Postoperative data
The follow-up visits included a duplex ultrasound and an evaluation of wound healing and pain 6 months postoperatively and annually thereafter. In case of complications (e.g., graft occlusion) within the first 6 postoperative months, patients were seen earlier.
According to the European Society of Cardiology guidelines, the patients with autologous grafts were discharged with anticoagulation therapy consisting of phenprocoumon to aim for a normalized ratio between two and four. 13 If patients had an indication for antiplatelet therapy, they also received 100 mg aspirin daily. The patients with prosthetic grafts were set on dual antiplatelet therapy consisting of aspirin (100 mg) and clopidogrel (75 mg) daily. 13 If they had an indication for anticoagulation due to cardiac reasons, they received antiplatelet therapy with aspirin (100 mg) daily and phenprocoumon.
Study endpoints
The primary endpoints were primary and secondary patency. Limb salvage and patient survival were secondary endpoints. The patency rates were defined according to the recommended standards for reports dealing with lower limb ischemia. 8 The 30-day results included 30-day mortality, 30-day amputation, 30-day graft failure, and morbidity data. Thirty-day mortality was defined as death within 30 days of the operation. Thirty-day amputation was defined as any above-ankle amputation of the index limb within 30 days of the index operation. Thirty-day graft failure was defined as occlusion of the bypass graft within 30 days of the index procedure. The recorded morbidity data consisted of perioperative myocardial infarction and perioperative stroke. For the patients who became unavailable during the follow-up period, the last available data regarding their status were used in the study.
Statistical analysis
All the categorical variables are presented as the absolute and relative frequencies, and age is shown as the mean (SD). Comparisons between the three renal function groups (normal vs moderate vs severe) were performed using an analysis of variance (ANOVA) for age and Pearson’s chi-squared test of independence was used for all the categorical data. The median follow-up time was assessed using the reverse Kaplan–Meier method of overall survival (OS). Loss of primary patency, loss of secondary patency, major amputation, and OS were defined from the date of tibial bypass surgery to the date of the respective event. In the case of no event, the patient was censored. The impact of renal function and graft material on all endpoints was analyzed using the Kaplan–Meier method. Furthermore, due to the advanced age of the patients, the cumulative incidence function (CIF) of loss of primary patency, loss of secondary patency, and major amputation were computed using a competing risk analysis with death as the competing event. Uni- and multivariable Cox proportional hazards regression models were used to assess the impact of renal function, graft material, and several further predictor variables on OS. Hazard ratios (HRs) and 95% CIs were calculated. Fine and Gray’s proportional subdistribution hazards regression models were used to estimate the subdistribution HRs for all predictor variables on the remaining endpoints with death as a competing risk. R software, version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria), was used for statistical analyses using the following packages: tableone, cmprsk, timereg, riskRegression, current-survival, and cr17.
Results
Between March 2002 and November 2018, 487 patients (295 men; age 73.28 ± 10.13 years) received 334 tibial (68.6%) and 153 peroneal (31.4%) bypass grafts. Kidney function was normal for 160 patients (32.9%), whereas 248 patients (50.9%) had moderate CKD, and 79 (16.2%) had severe CKD. The indication was CLTI in all the cases. Ischemic rest pain was present in 127 patients (26.1%) and tissue loss was present in 360 patients (73.9%). The median follow-up time was 6.1 years.
The preoperative risk factors and indications were similarly distributed between the groups except for age, diabetes mellitus, hypertonus, CAD, smoking history, cerebrovascular disease, and Rutherford class. A comparison of the preoperative risk factors and indications is shown in Table 1. Vein bypasses were performed in 289 patients (59.3%), with the GSV most commonly used. In 198 patients (40.7%, prosthetic conduits were used, which consisted of PTFE in 74 patients (15.2%) and HePTFE in 125 patients (25.7%). There were no significant differences in the procedural details between the groups regarding the distribution of PTFE and the tibiofibular trunk as the distal anastomotic vessel. The comparisons of procedural details and bypass graft characteristics are shown in Table 2.
Preoperative risk factors and indications presented with chronic kidney disease stage.
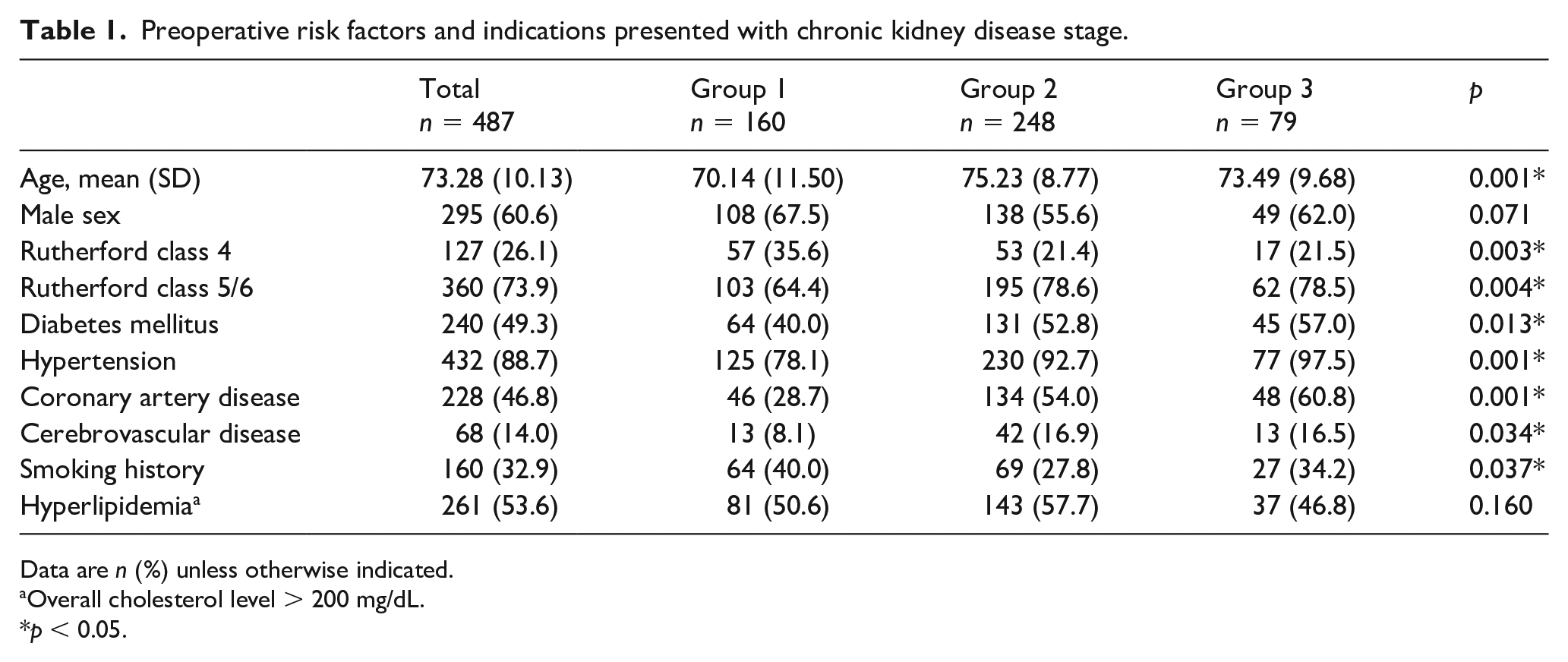
Data are n (%) unless otherwise indicated.
Overall cholesterol level > 200 mg/dL.
p < 0.05.
Procedural details and bypass graft characteristics.
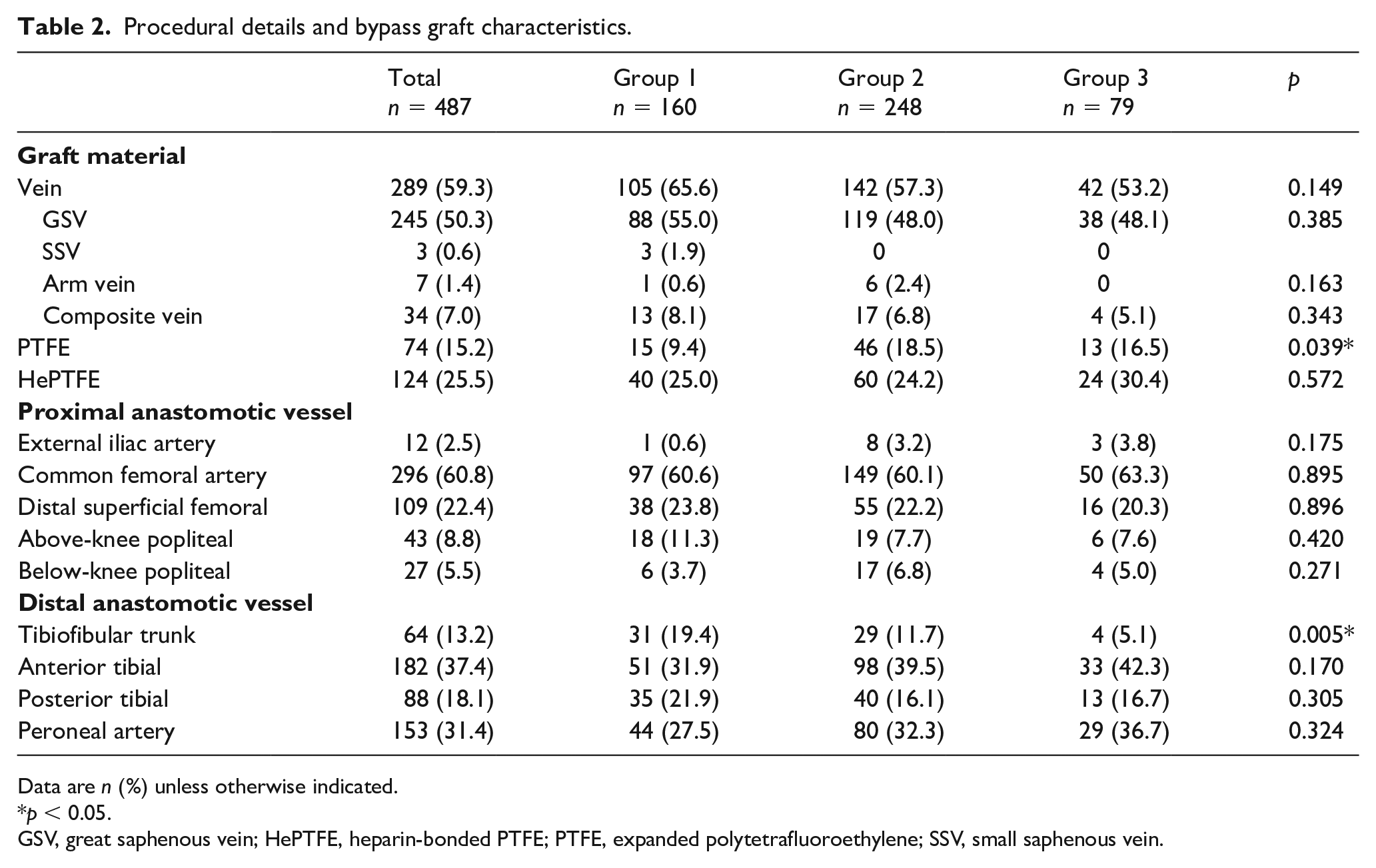
Data are n (%) unless otherwise indicated.
p < 0.05.
GSV, great saphenous vein; HePTFE, heparin-bonded PTFE; PTFE, expanded polytetrafluoroethylene; SSV, small saphenous vein.
30-day results
The 30-day results are shown in Table 3. Overall, 25/487 patients died; thus, the 30-day mortality rate was 5.1% (group 1 = 5/160 [3.1%] vs group 2 = 10/248 [4.0%] vs group 3 = 10/79 [12.7%]; p = 0.004). Of these 25 cases, the sources of death were myocardial infarction (n = 11), pneumonia (n = 3), renal failure (n = 4), and multiorgan failure (n = 4). In two cases, the cause of death was not related to the bypass surgery. Univariate analysis showed that CKD severity had no influence on 30-day mortality rate (group 2: odds ratio (OR) 1.44 [0.49–4.22]; p = 0.508; group 3: OR 2.55 [0.75–8.62]; p = 0.133). Perioperative myocardial infarction occurred in 4.7% (23/487; group 1 = 4/160 [2.5%] vs group 2 = 15/248 [6.0%] vs group 3 = 4/79 [5.1%]; p = 0.253) and perioperative stroke occurred in 1.4% (7/487; group 1 = 1/160 [0.6%] vs group 2 = 2/248 [0.8%] vs group 3 = 4/79 [5.1%]; p = 0.012) of the patients. The overall 30-day graft failure rate was 10.9% (53/487) leading to major amputation in 3.3% (16/487; group 1 = 4/160 [2.5%] vs group 2 = 5/248 [2.0%] vs group 3 = 7/79 [8.9%]; p = 0.049) of the patients.
Results at 30 days.
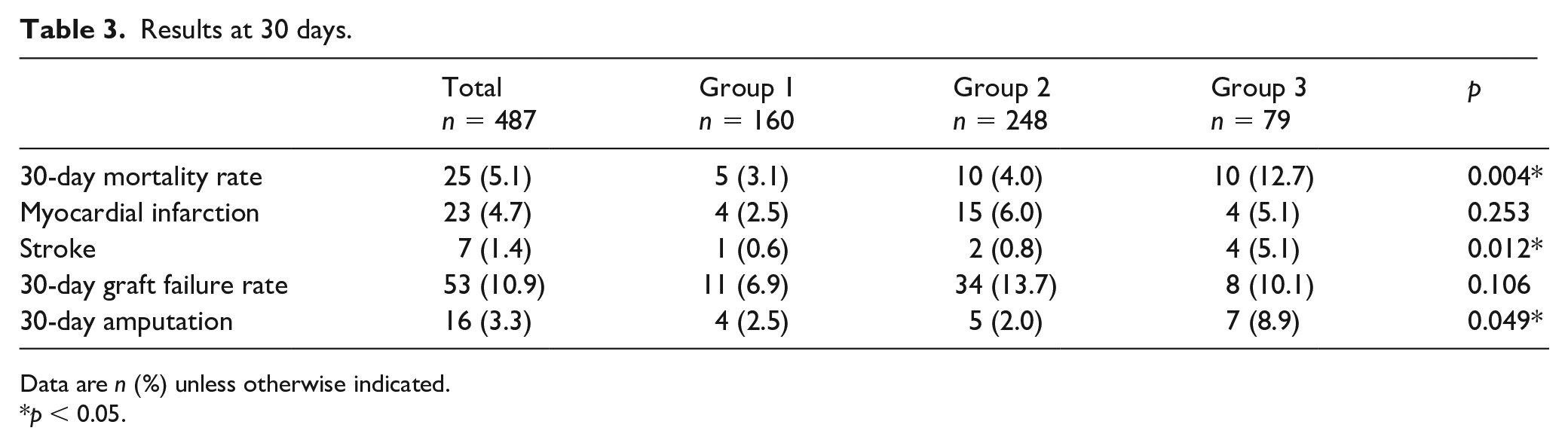
Data are n (%) unless otherwise indicated.
p < 0.05.
Long-term outcomes
At the follow-up timepoints of 1, 3, and 5 years, the overall primary patency rates were 64.6%, 52.1%, and 46.0%, respectively. The primary patency rates were 71.1%, 56.4%, and 48.2% for group 1; 60.0%, 49.9%, and 44.3% for group 2; and 65.5%, 48.5%, and 48.5% for group 3, respectively. No significant differences were noted between the groups (p = 0.363). Additionally, at 1, 3, and 5 years, overall secondary patency rates were 72.7%, 61.7%, and 54.9%, respectively. The secondary patency rates were 79.0%, 66.7%, and 58.8% for group 1; 69.2%, 59.8%, and 54.4% for group 2; and 69.9%, 54.9%, and 46.3% for group 3, respectively. No significant differences were noted between the groups (p = 0.268).
Limb salvage rates are shown in Figure 1. At the timepoints 1, 3, and 5 years, the resulting limb salvage rates overall were 86.5%, 79.2%, and 77.3%, respectively. They did not differ significantly between patients with normal renal function and patients with moderate CKD (91.3%, 84.3%, and 82.1% for group 1 vs 85.4%, 79.2%, and 77.2% for group 2; p = 0.239), whereas they were significantly lower for patients with severe CKD (79.2%, 65.3%, and 65.3% for group 3; p = 0.006).
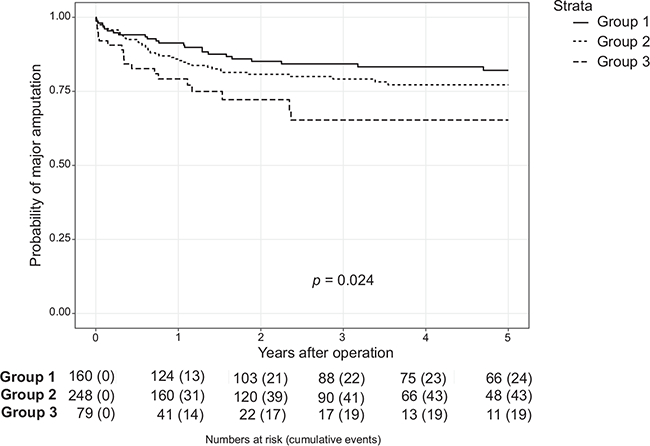
Loss of limb salvage.
Survival rates are shown in Figure 2. At 1, 3, and 5 years, the overall survival rates were 80.1%, 60.1%, and 48.0%, respectively. Survival rates were significantly lower for patients with moderate and severe CKD compared to patients with normal function. At 1, 3, and 5 years, survival rates were 89.1%, 76.5%, and 67.0% for group 1; 80.1%, 59.7%, and 44.1% for group 2; and 61.9%, 27.7%, and 19.6% for group 3 (p < 0.001).
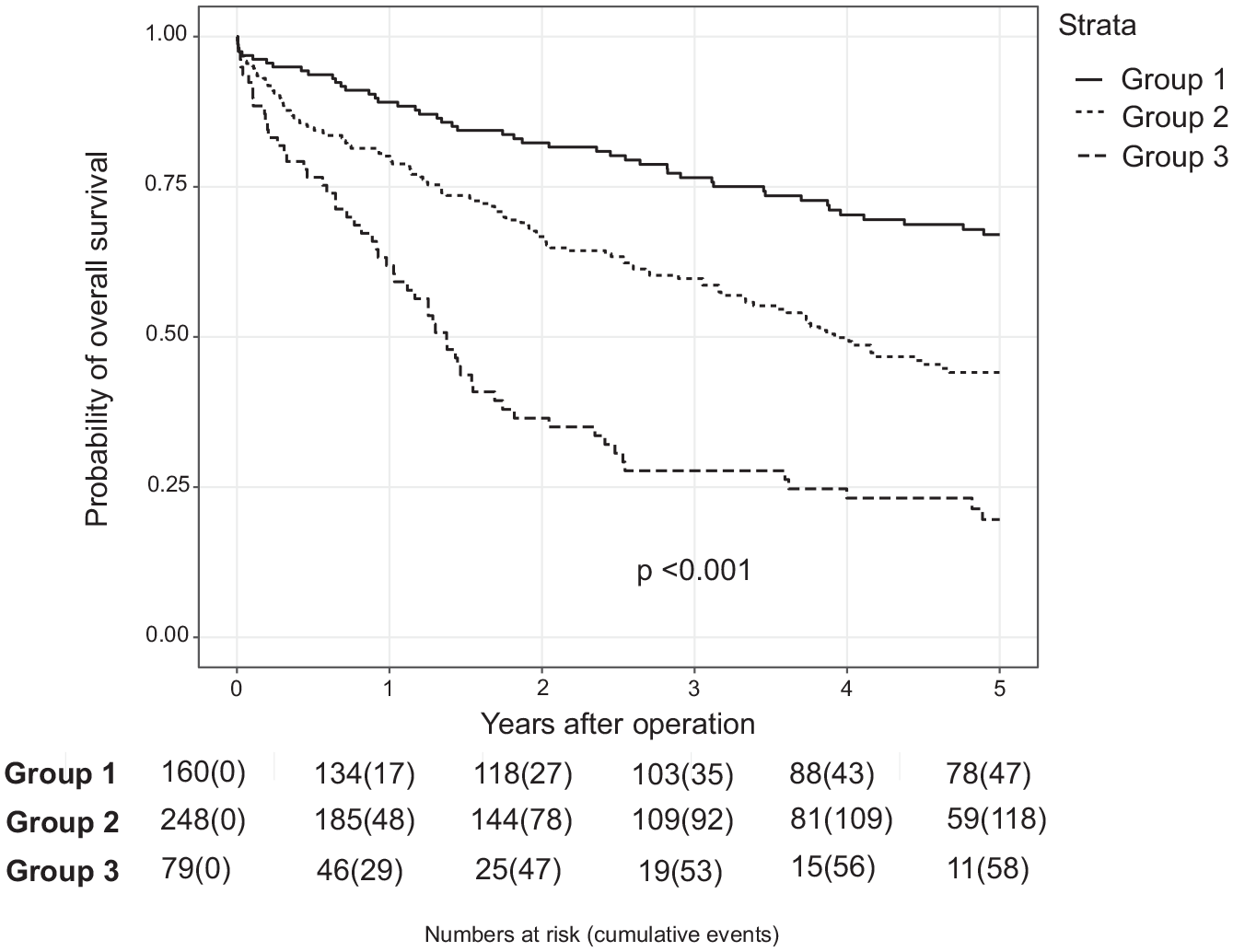
Probability of survival.
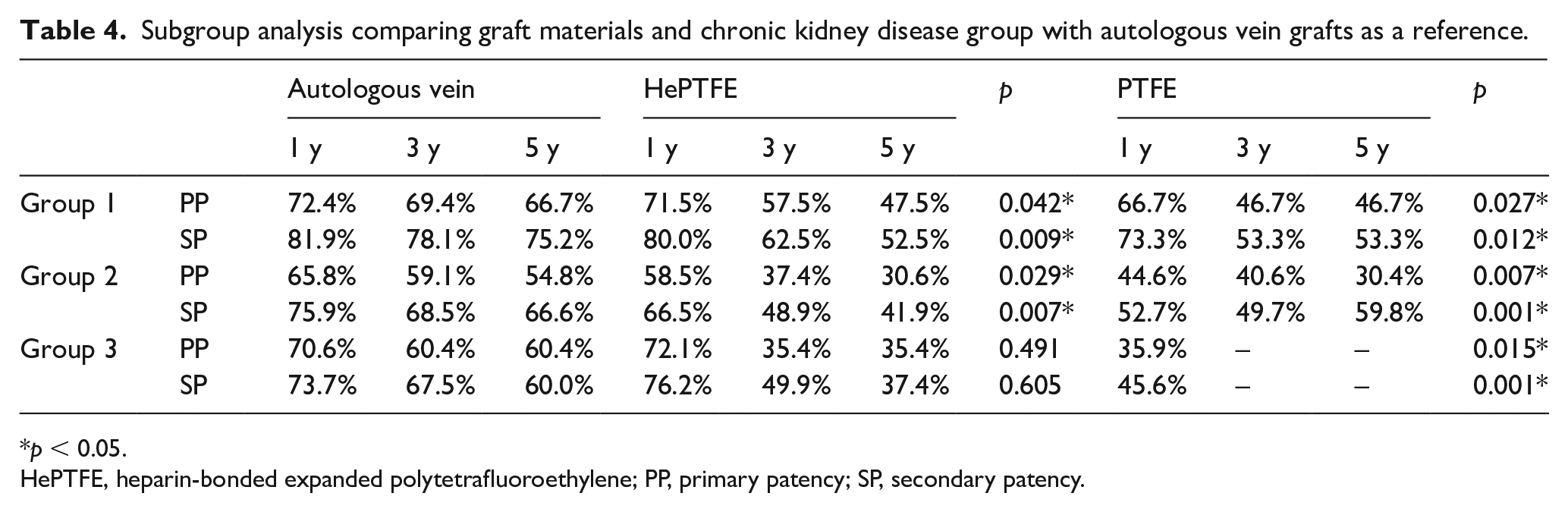
The subgroup analyses comparing graft materials, with autologous vein grafting as a reference, and CKD class is presented in Table 4. At the timepoints 1, 3, and 5 years, primary and secondary patency rates using HePTFE and PTFE grafts were significantly lower for groups 1 and 2 compared to the autologous vein grafts. PFTE grafts produced the worst results. For group 3, analysis of the primary and secondary patency rates of PTFE grafts was only performed at the 1-year timepoint because not enough patients with these grafts survived beyond this to identify any meaningful relationship. With regards to the HePTFE grafts, the primary and secondary patency rates for group 3 at the 1-year timepoint were similar to those of the autologous vein grafts. At the timepoints 3 and 5 years, the primary and secondary patency rates for HePTFE grafts were lower but did not cross the threshold of statistical significance.
Subgroup analysis comparing graft materials and chronic kidney disease group with autologous vein grafts as a reference.
p < 0.05.
HePTFE, heparin-bonded expanded polytetrafluoroethylene; PP, primary patency; SP, secondary patency.
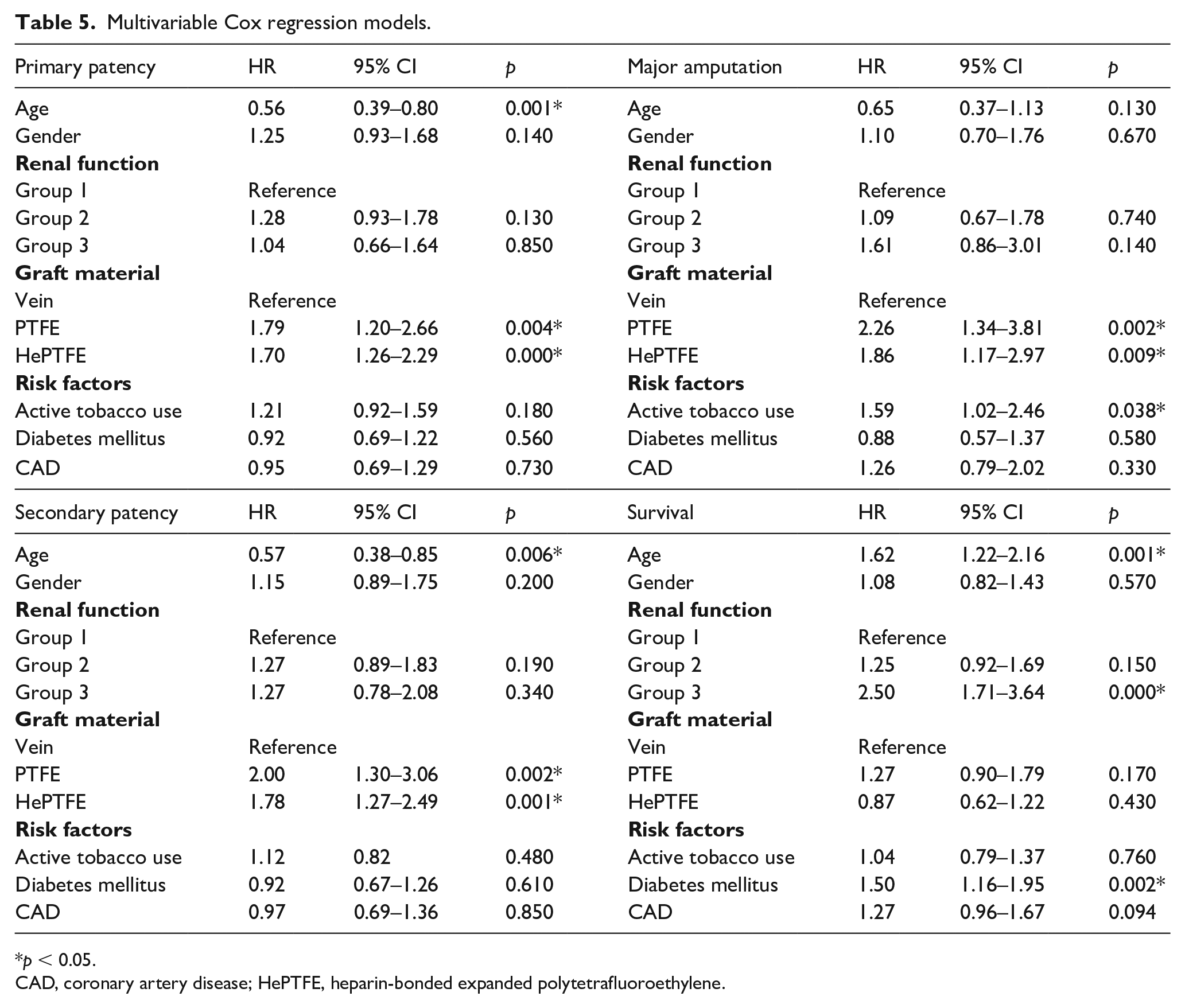
The multivariable Cox regression models are shown in Table 5. Multivariable Cox regression showed that CKD severity had no influence on the primary (group 2: HR 1.28 [0.93–1.78]; p = 0.130; group 3: HR 1.04 [0.66–1.64]; p = 0.850) and secondary patency rates (group 2: HR 1.27 [0.89–1.83]; p = 0.190; group 3: HR 1.27 [0.78–2.08]; p = 0.340). Prosthetic graft materials were risk factors for loss of primary patency (PTFE: HR 1.79 [1.20–2.66]; p = 0.004; HePTFE: HR 1.70 [1.26–2.29]; p < 0.0001) and loss of secondary patency (PTFE: HR 2.00 [1.30–3.06]; p = 0.002; HePTFE: HR 1.78 [1.27–2.49]; p < 0.001). Active tobacco use (HR 1.59 [1.02–2.46]; p = 0.038), PTFE (HR 2.26 [1.34–3.81]; p = 0.002), and HePTFE graft use (HR 1.86 [1.17–2.97]; p = 0.009) were risk factors for major amputation. Severe CKD (HR 2.50 [1.71–3.64]; p = 0.000), diabetes (HR 1.50 [1.16–1.95]; p = 0.002), and age ⩾ 80 years (HR 1.62 [1.22–2.16]; p = 0.001) were associated with an increased risk of death.
Multivariable Cox regression models.
p < 0.05.
CAD, coronary artery disease; HePTFE, heparin-bonded expanded polytetrafluoroethylene.
Discussion
Patients with CKD have a higher risk of developing generalized atherosclerosis compared to individuals with normal renal function. 14 Furthermore, 20% of these patients suffer from PAD with nearly a twofold higher risk of developing CLTI leading to death or amputation, if left untreated. 15 Several earlier studies have evaluated the role of surgical revascularization, including all types of lower extremity bypass surgery, for CLTI patients with CKD, but these studies primarily focused on patients with ESRD.1,2,5 To the best of our knowledge, no earlier studies have exclusively analyzed the long-term outcomes after infrapopliteal HePTFE bypass surgery for patients with varying degrees of CKD severity.
In our cohort, the different stages of CKD had no significant effect on the long-term graft patency rates after surgical revascularization via infrapopliteal bypass. However, the choice of graft material had an influence, especially for patients with severe CKD. These findings compare favorably with previously published reports.1,5 Ballotta et al. reported primary patency rates of 49.1% for CKD patients on dialysis and 85.3% for those not on dialysis 5 years after infrapopliteal bypass surgery, mainly using the vein as the graft material. Secondary patency rates were 68.0% and 90.1%, respectively. 1 In our cohort, the patients with autologous vein grafts and severe CKD achieved comparable results after 5 years. In contrast to the above-mentioned study, the primary and secondary patency rates for patients with moderate CKD and normal renal function were considerably lower. However, we primarily included short vein bypass grafts with inflow arteries on the more distal vessels. Furthermore, more peroneal bypass surgeries were performed in our cohort, and we used more prosthetic grafts, which may explain the poorer patency rates for the patients with moderate CKD and normal renal function.
Arhuidese et al. reported different findings, however. They analyzed the outcomes of autogenous and prosthetic bypass grafts for patients with ESRD and included femoropopliteal, femorotibial, and popliteotibial bypass surgeries. 5 The primary and secondary patency rates in their study were 18% and 30%, respectively, for both types of conduit grafts at 5 years. However, the authors demonstrated via a multivariate analysis an advantage for autogenous compared to prosthetic bypass graft usage in terms of patency rate, which is potentially of the most clinical relevance for femorotibial and popliteotibial configurations. 5 In our study, the prosthetic graft materials were risk factors for loss of primary and secondary patency, and we did not differ between bypasses in the femorotibial and popliteotibial positions. The primary and secondary patency rates for the prosthetic materials, either HePTFE or PTFE, were significantly worse after 5 years, compared to the autologous vein grafts, for all the CKD groups analyzed. In contrast to these findings, the subgroup analysis showed comparable patency rates between autologous vein and HePTFE grafts in patients with severe CKD at the 1-year mark, whereas PTFE produced extremely poor results. These findings are similar to those reported for a study in which the use of HePTFE grafts in CLTI alone was investigated. Daenens et al. reported a primary patency rate of 79% for femorotibial HePTFE bypasses and 69% for autologous vein grafting at the 1-year mark, without statistical significance. 16 Neville et al. found that the patency rates of vein and HePTFE grafts after 1 year were not significantly different, although the vein grafts achieved better results. 17
Nevertheless, we observed a significant difference in perioperative mortality and long-term survival rates between the groups, with the worst results for patients with severe CKD. Our limb salvage rates did not differ between the patients with normal renal function and those with moderate CKD, whereas it was significantly lower for the patients with severe CKD. Our survival rate after 5 years was 19.6% for the patients with severe CKD, and the limb salvage rate was 65.3% for this patient group. In a recent meta-analysis, Albers et al. described a 5-year pooled patient survival rate of 23.0% and a limb salvage rate of 66.0% for patients with ESRD, both of which are comparable to our findings. This analysis included all types of infrainguinal arterial reconstructions, axillo-femoral and aorto-femoral bypasses, and ilio-femoral bypasses. 4 Similar results were reported by Biancari et al., in which ESRD patients had significantly lower OS rates than patients with no or less severe renal failure. The limb salvage rate for the ESRD patients was 60.8%. 18 Furthermore, Lacroix et al. analyzed the mortality rates of patients with CKD who were hospitalized for PAD and described a mortality rate that increased according to the CKD class. In that study, the presence of severe CKD was an independent predictor of 1-year mortality, and the limb salvage rate for the ESRD patients was 59.8% at the 1-year mark. 19 As in our study, Patel et al. found that age, diabetes, and severe CKD were risk factors for reduced life expectancy. 20 The perioperative mortality rate for the patients with severe CKD in our study was significantly higher than that of the patients with no or moderate CKD; within the first 30 days, 12.7% of our patients with severe CKD had died, with more than 70% of them suffering with trophic lesions. This is in-line with a recent analysis by Lüders et al., who described a twofold higher in-hospital mortality (7.8%) for patients with CKD alone compared to those without known CKD (4%); the highest in-hospital mortality occurred for patients with CKD stage 4 and Fontaine stage IV (16%), which is equivalent to group 3 in our study, regardless of the therapy. 21 However, the Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia recommend endovascular therapy for high-risk patients with a perioperative mortality > 5%. 3 Owing to the high perioperative mortality of patients with severe CKD in our cohort, we also believe that perhaps a more aggressive approach to endovascular revascularization may be warranted for this population.
Study limitations
Several limitations should be pointed out in the current study. First, our study cohort was too small to evaluate outcomes for all the CKD classes, which would have been ideal. As in other studies, only the CKD 4 and 5 patients (eGFR threshold of < 30 mL/min/1.73 m2) in our study were at the highest risk of adverse events, such as limb loss and nonsurvival. 15 Therefore, we chose to stratify the patients into groups with and without severe CKD. Another limitation was the retrospective design of our study, leading to possible observational and selection bias. Additionally, we did not measure all the reliable confounders on patency, limb salvage, and survival; thus, our data may not be fully comparable to the entire population. Moreover, we did not analyze endovascularly treated CKD patients over the study period because the study focused on tibial and peroneal bypasses. Therefore, we could not compare the results between the endovascular and the operative treatments for these patients.
Conclusions
In conclusion, our data confirmed the long-term benefits of autologous conduits compared to prosthetic conduits for patients with CKD and CLTI. Nevertheless, HePTFE grafts displayed good short-term results for patients with severe CKD. Given the short life-expectancy of these high-risk patients, prosthetic HePTFE grafts may be reasonable for this population if a suitable vein for autologous grafting is not available.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X211036751 – Supplemental material for Impact of chronic kidney disease on the outcomes of infrapopliteal venous, and heparin-bonded expanded polytetrafluoroethylene bypass surgeries: A retrospective cohort study
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X211036751 for Impact of chronic kidney disease on the outcomes of infrapopliteal venous, and heparin-bonded expanded polytetrafluoroethylene bypass surgeries: A retrospective cohort study by Thomas Betz, Ingolf Toepel, Karin Pfister, Malisia Lang, Markus Steinbauer, Christian Uhl, Florian Zeman and Wilma Schierling in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.