
Abstract

Acute aortic syndromes and pulmonary embolism (PE) are in the cardiovascular differential diagnosis of acute chest discomfort.1,2 We present two challenging cases: a case of hemodynamically unstable PE in the course of recuperation following aortic rupture repair, and another case with acute aortic dissection while being treated with anticoagulation for prior hemodynamically unstable PE.
Case 1: syncope, tachycardia, and hypotension in a patient with recent aortic rupture open repair
A 69-year-old woman was brought to the emergency room with severe abdominal discomfort and tachycardia (102 bpm). Contrast-enhanced computed-tomography revealed a large ruptured abdominal aortic aneurysm and hematoma (Panels A1, A2). She underwent emergent open aneurysm repair and was discharged uneventfully on postoperative day 8.
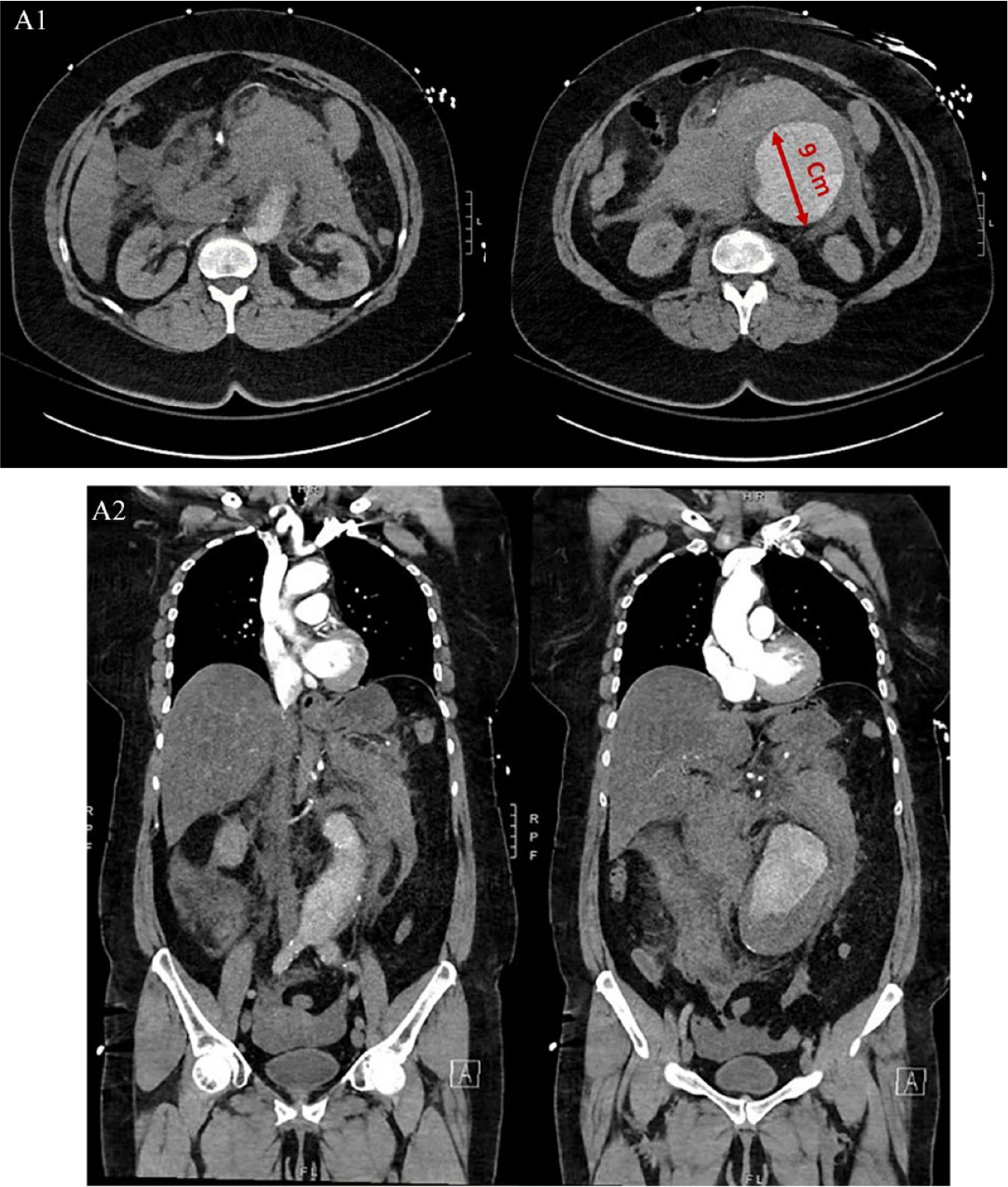
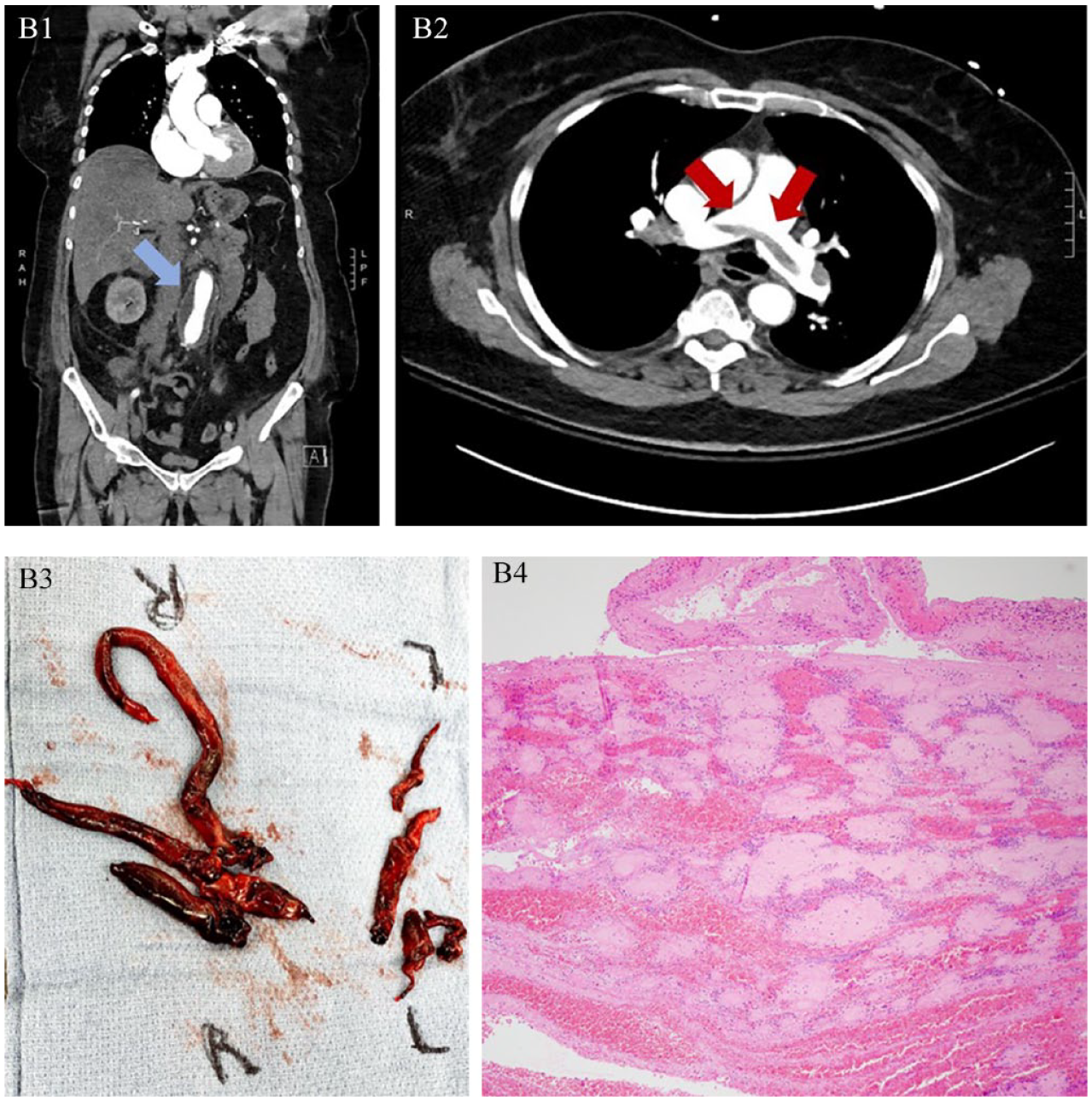
A week after discharge, she presented with respiratory distress, sinus tachycardia (126 bpm), and systolic hypotension (76 mmHg). Computed tomography of the chest, abdomen, and pelvis showed stable aortic contour (Panel B1, blue arrow) but a large saddle PE with right heart thrombi (Panels B2, red arrows). She underwent successful emergent surgical embolectomy (Panels B3, B4, Supplemental Video 1).
Case 2: chest pain and ST-elevation in a patient with ascending aortic aneurysm and prior hemodynamically unstable PE
A 61-year-old man with history of hypertension presented with intermittent chest discomfort that started 5 days previously and deteriorated on the day of admission.
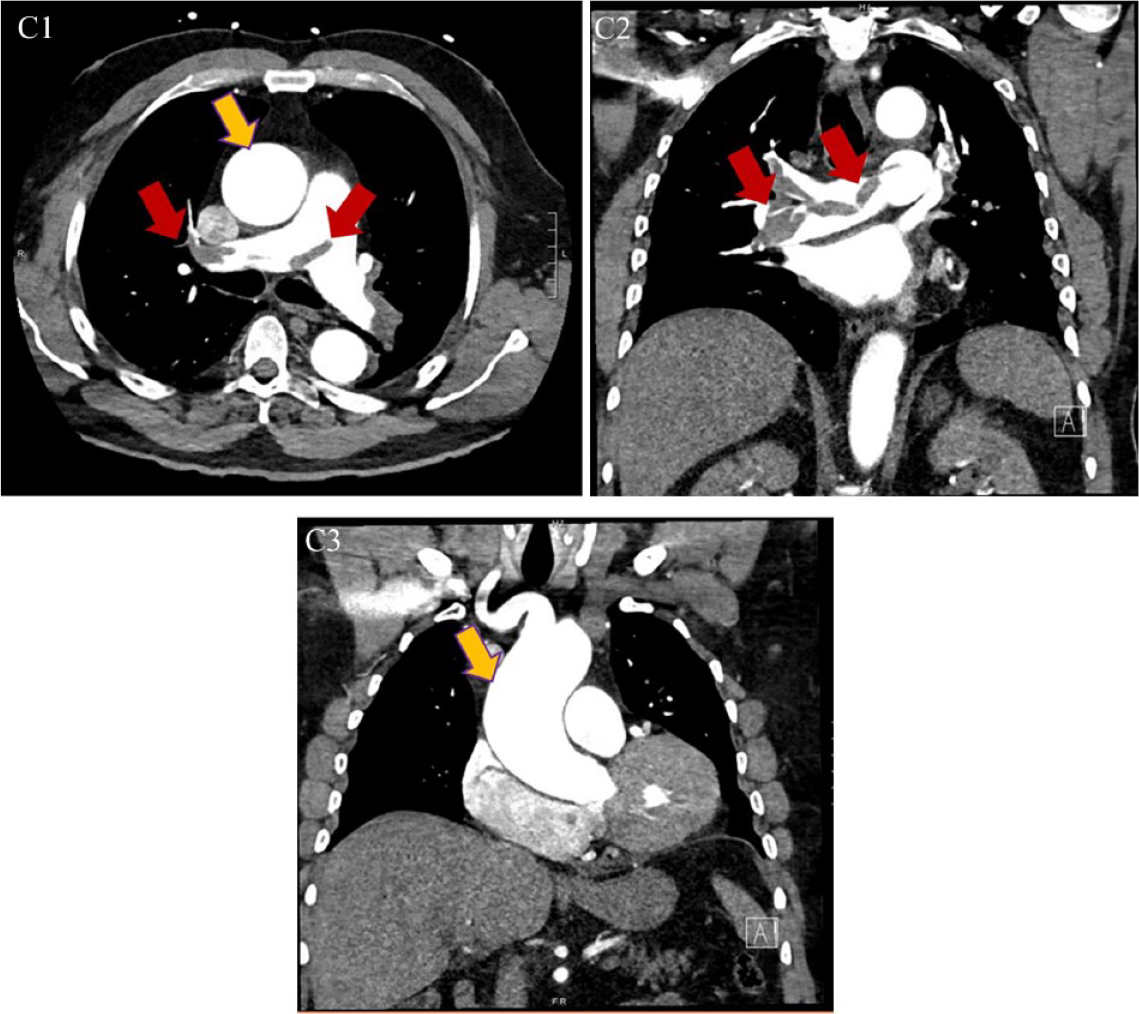
The previous year, he was diagnosed with hemodynamically unstable PE, which was treated with systemic fibrinolysis followed by apixaban (Panels C1, C2, red arrows). In addition, he was noted to have an aneurysmal ascending aorta, which measured 4.8 cm by 4.5 cm (Panel C1, C3, yellow arrows). He was advised to present for 6-month follow-up.
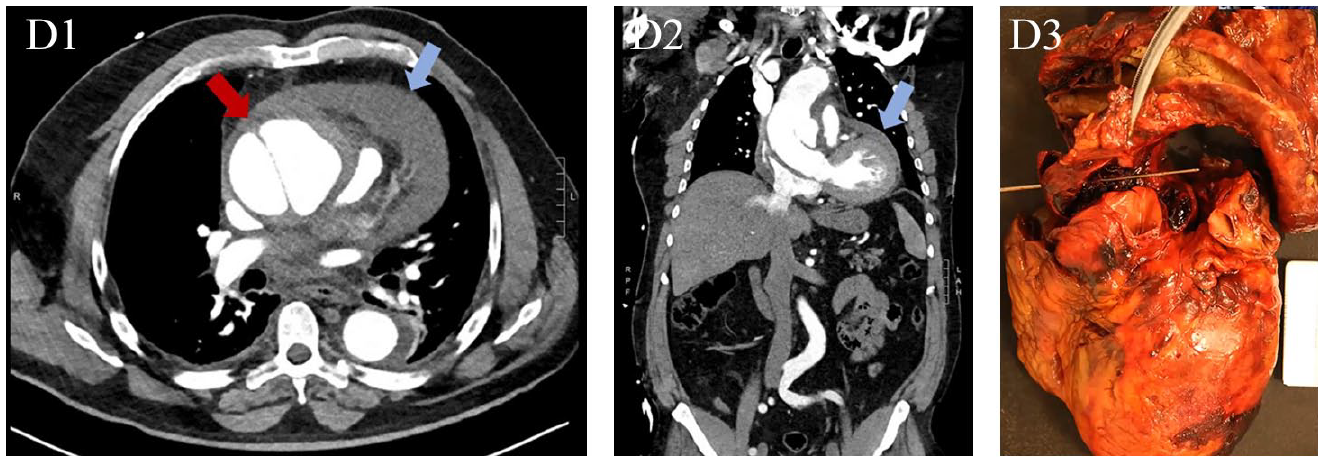
At the time of the index presentation, he was in distress, tachycardic (120 bpm), and hypertensive (166/111 mmHg). An electrocardiogram showed inferior ST-segment elevations. Bedside echocardiography showed the presence of pericardial effusion and aortic insufficiency, shifting the concern for a Stanford type A acute aortic syndrome, which was confirmed by computed tomography (Panels D1, D2, red arrow and blue arrows). He was emergently moved to the operating room. However, he suffered from a cardiac arrest and expired in the operating room. Autopsy confirmed the acute aortic rupture (Panel D3).
PE and acute aortic syndromes are vascular emergencies that may occur in close succession. 3 Their recognition and management require a team with expertise in both conditions such that the “uninvited guest” of a second vascular medicine emergency is recognized and treated.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Bikdeli reports that he is a consulting expert, on behalf of the plaintiff, for litigation related to two specific brand models of IVC filters. Dr Piazza has received research grant support to Brigham and Women’s Hospital from EKOS, a BTG International Group company, Bayer, the Bristol Myers Squibb/Pfizer Alliance, Portola, and Janssen; he has received consulting fees from Amgen, Pfizer, Boston Scientific Corporation, and Thrombolex. Dr Goldhaber has received research support from Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Boston Scientific, Daiichi-Sankyo, Janssen, the National Heart, Blood, and Lung Institute, and the Thrombosis Research Institute; he has received consulting fees from Bayer, Agile, Boston Scientific Corporation, and Boehringer Ingelheim.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.