
Abstract

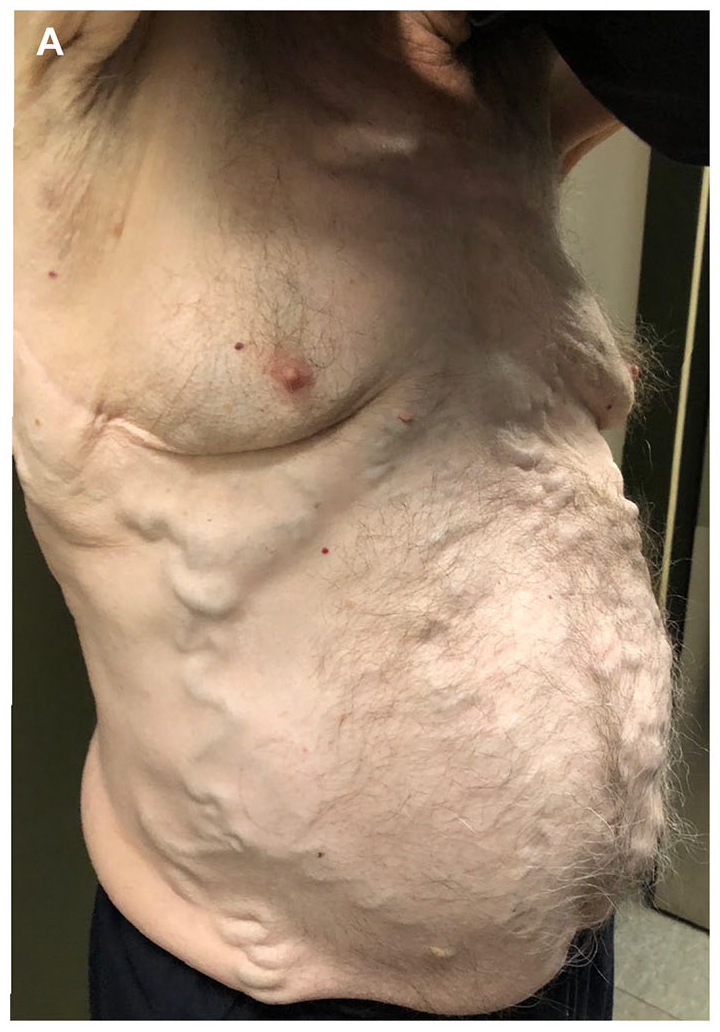
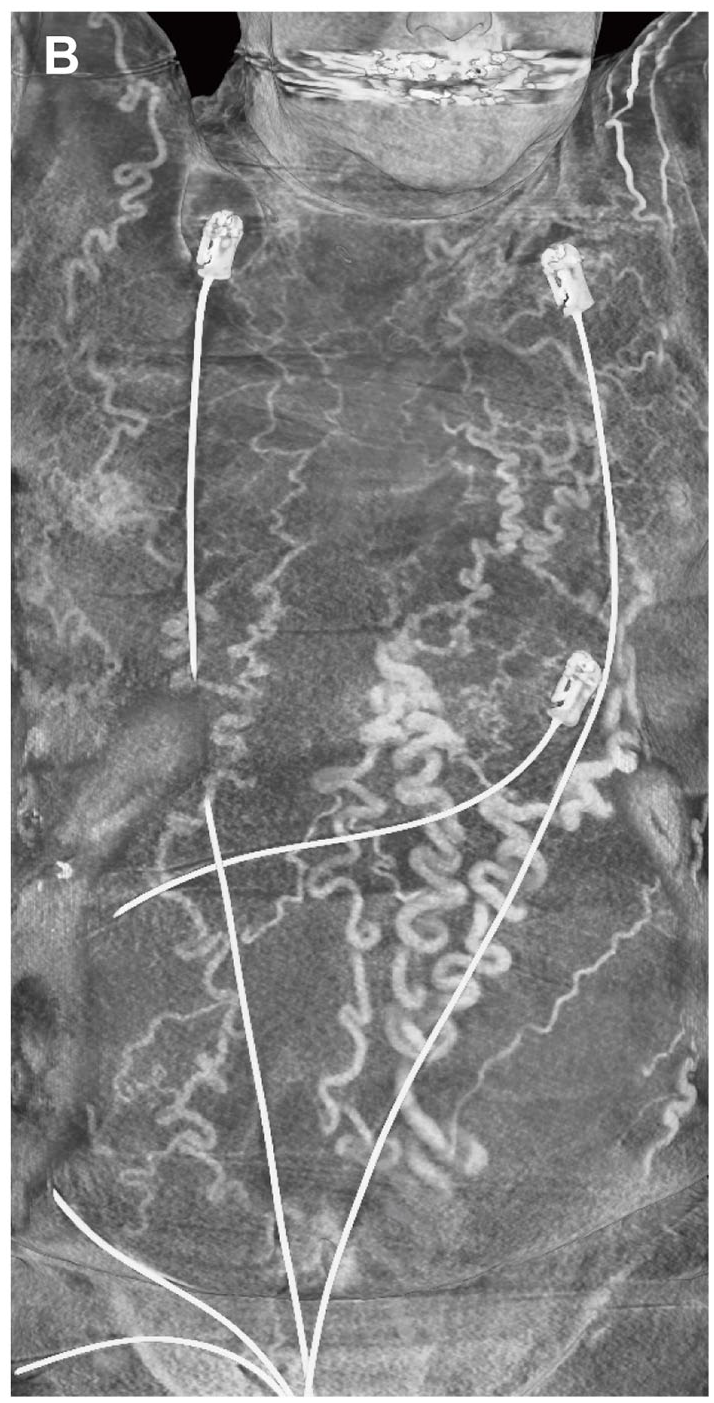
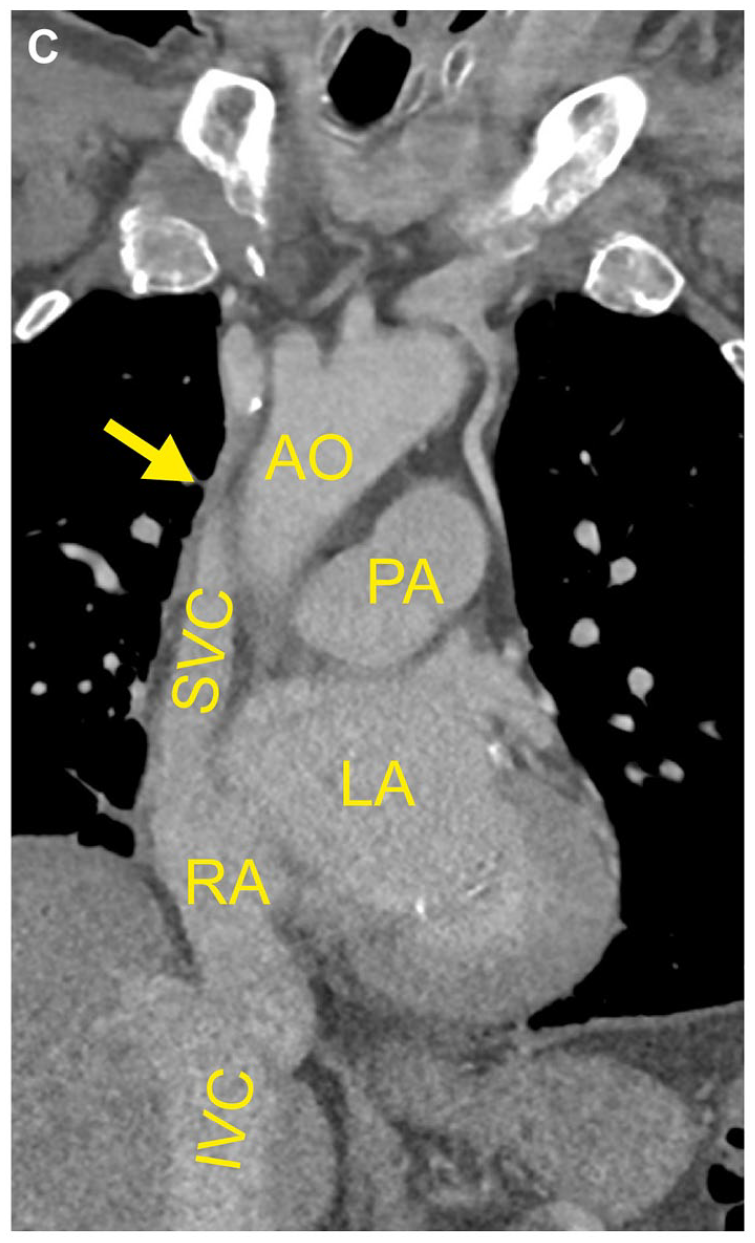
During planning for a transcatheter aortic valve replacement for severe aortic stenosis in a 76-year-old man, physical examination showed pronounced varicose veins of the abdomen (Panel A). Thorough clinical history revealed their development after a thymectomy and radiotherapy for thymic carcinoma about 40 years ago. The patient had long accepted the varicosities as a mere cosmetic issue. Liver cirrhosis and portal hypertension were ruled out and the patient was prepared for aortic valve replacement. However, in the preprocedural CT angiography, the contrast agent injected into the left cubital vein drained via the superficial epigastric veins into the femoral veins before entering the inferior vena cava (Panel B; CT reconstruction). Panels C and D show coronal CT images with arrows pointing at the occluded superior vena cava (AO, aorta; LA, left atrium; PA, pulmonary artery; RA, right atrium; SVC/IVC, superior/inferior vena cava; VJI, internal jugular vein). Clinical relevance emerged, when, after successful aortic valve replacement, implantation of the temporary pacemaker lead through the jugular vein was not feasible. Phlebography confirmed an occlusion of the superior vena cava with drainage via collaterals on the abdomen and the azygos system, presumably attributable to the previous cancer treatment.

Symptoms of superior vena cava syndrome (SVC) include edema of head and neck as well as dyspnea, with the severity depending on the speed of development of SVC and the capacity of collaterals. Typical causes are intrathoracic tumors, with lung carcinoma and non-Hodgkin lymphoma causing the majority of malignant-associated cases. However, compression can also be caused by nonmalignant masses and, more recently, the growing use of intravascular devices has led to an increased proportion of SVC caused by venous thrombus formation.1,2 The history of cancer treatment in the present case, therefore, depicts a rare cause for SVC. 3 Fortunately, the gradual development of SVC appears to have guarded our patient from more severe symptoms. Permanent pacemaker implantation was not required, and the patient could be discharged.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Acknowledgements
We thank Dr. Johannes Rübenthaler (University Hospital Munich, LMU, Munich, Germany) for his kind help in the reconstruction of the CT images.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.