
Abstract

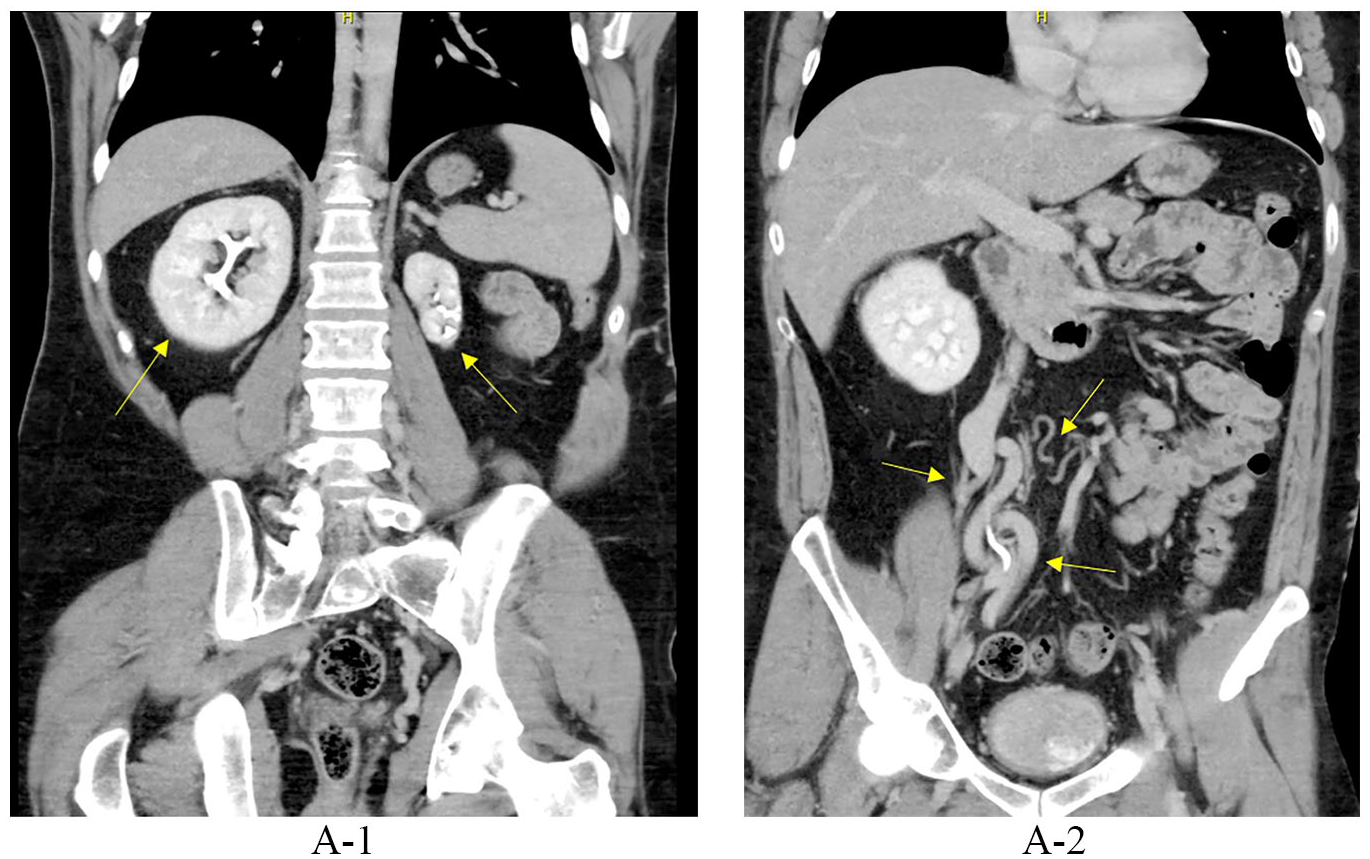
A 36-year-old male with no previous medical problem presented with a 3-day history of left leg pain and swelling. Lower extremity duplex ultrasound showed extensive acute deep vein thrombosis (DVT) of the left external iliac vein, common femoral vein, profunda femoral vein, femoral vein, popliteal vein, gastrocnemius vein, tibial veins, and peroneal vein. Owing to the extensive degree of thrombus, computed tomography (CT) of the abdomen and pelvis was ordered. CT showed extensive abdominal/pelvic venous thrombosis, congenital absence of the inferior vena cava (IVC), as well as atrophy of the left kidney with hypertrophy of the right kidney (Panel A1, arrows). There was also presence of extensive collateral veins (Panel A2, arrows).
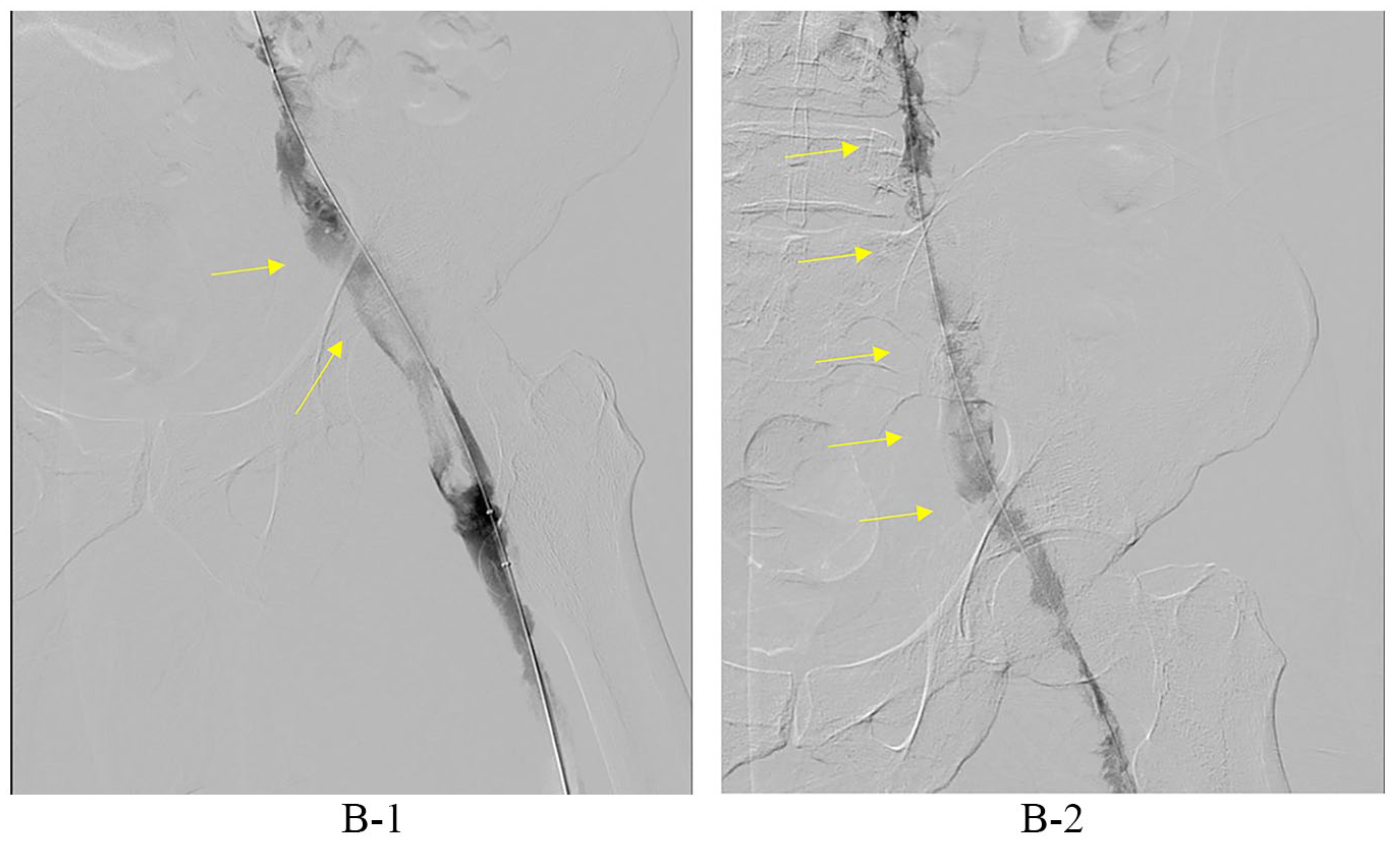
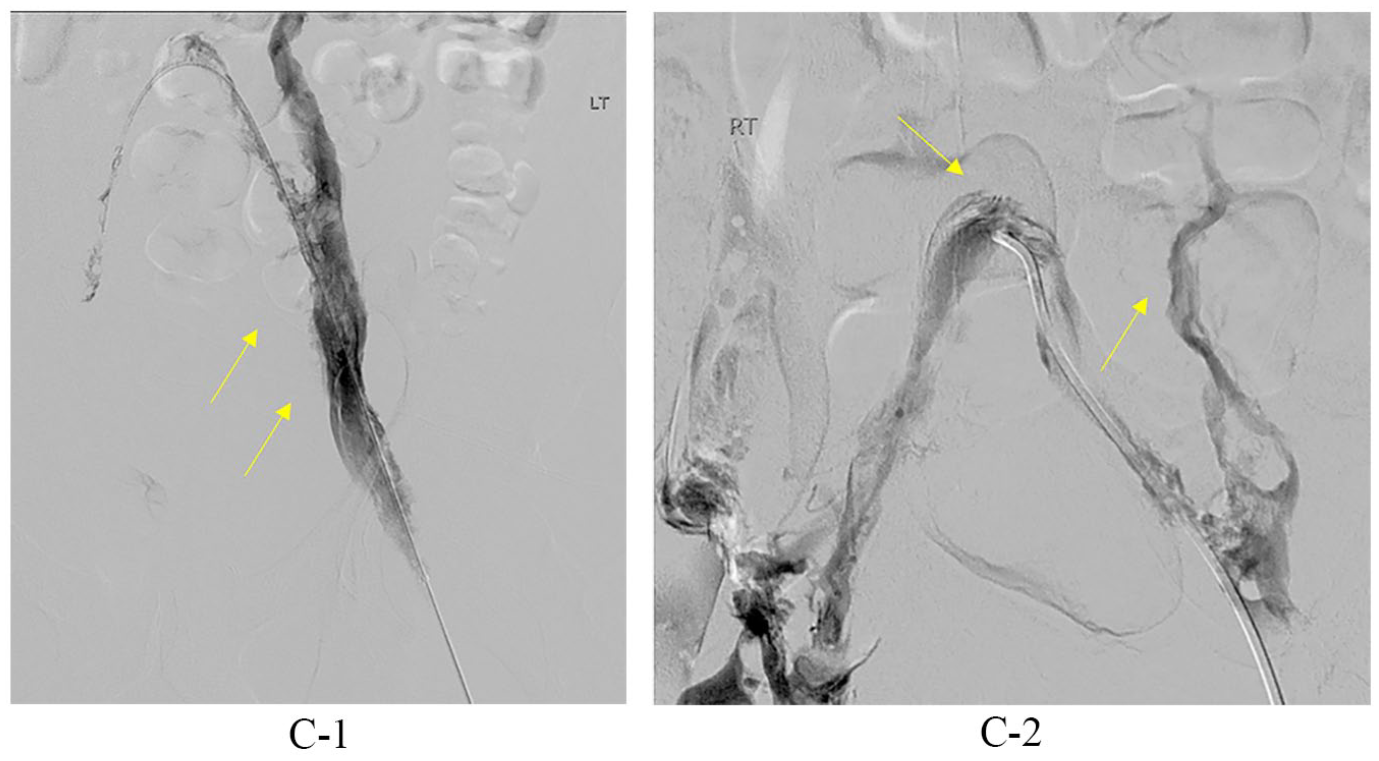
He was started on oral anticoagulation, but because of persistent pain underwent mechanical thrombectomy with catheter-directed thrombolysis. Venography confirmed the extensive DVT in the femoral, iliac, and paralumbar veins (Panels B1 and B2, arrows). The procedure improved outflow from the left lower extremity to paralumbar collaterals in the abdomen (Panel C1, arrows), and absence of the IVC was again identified (Panel C2, arrows). At 2-month follow-up, the patient reported only mild persistent pain and swelling of the left lower extremity with return to normal daily activities. Extensive thrombophilia workup was unremarkable except for heterozygous Factor V Leiden mutation.
Considering the unique presentation, a review of the literature uncovered a description that fit this patient. The KILT (Kidney and IVC abnormalities with Leg Thrombosis) syndrome is a disorder consisting of renal and IVC maldevelopment, and DVT. Perhaps in utero venous thrombosis predisposed to these developmental abnormalities. Ninety percent of malformations involve the suprarenal IVC but can also involve the renal and infrarenal IVC, and either kidney can be affected depending upon the venous abnormality.1–3 Lower extremity venous outflow is maintained by collaterals to the azygous and hemi-azygous systems. The prevalence of KILT syndrome is unknown due to a lack of awareness in asymptomatic patients and underdiagnosis in symptomatic patients.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.