
Abstract

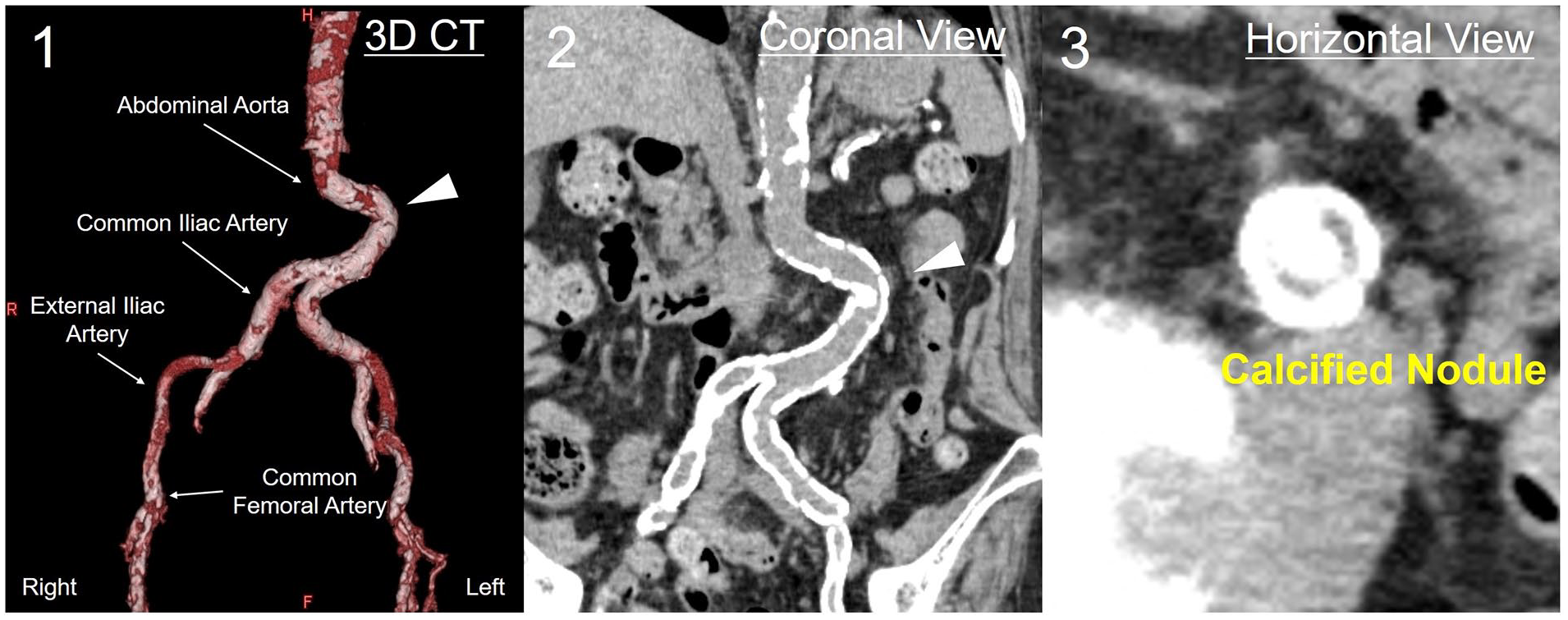
An 86-year-old female patient was admitted to our hospital with acute heart failure. Echocardiography revealed severe hypokinesis in the inferior left ventricular wall. Coronary angiography demonstrated severe stenosis and calcification of the right coronary artery. A staged percutaneous coronary intervention (PCI) was scheduled. However, few access routes for PCI were available, as both radial arteries were occluded, her left elbow was contracted in the flexed position due to previous stroke, the abdominal aorta had severe tortuosity, and a calcified nodule protruded into its lumen (Panels A, arrowhead). First, we attempted to perform PCI via the right brachial artery but could not manipulate the guiding catheter because of severe tortuosity and calcification in the right brachiocephalic and subclavian arteries. Therefore, we attempted PCI using the right common femoral artery (CFA). A 6-Fr long guiding sheath, coated with a hydrophilic polymer, was inserted into the thoracic aorta through the right CFA, and PCI was successfully performed without any major complications.
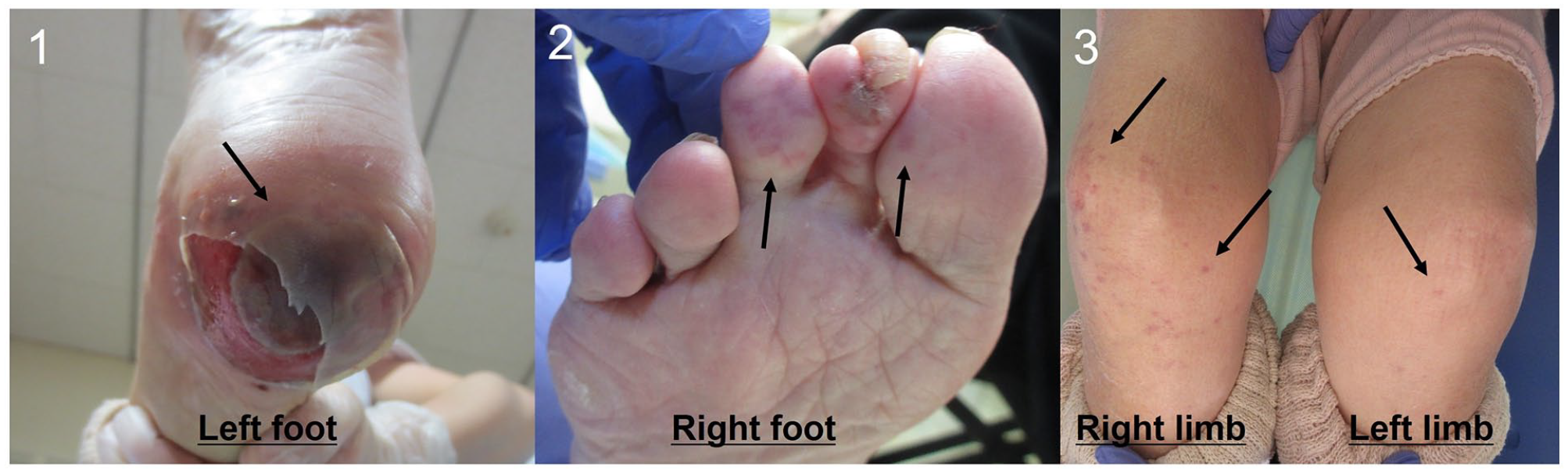
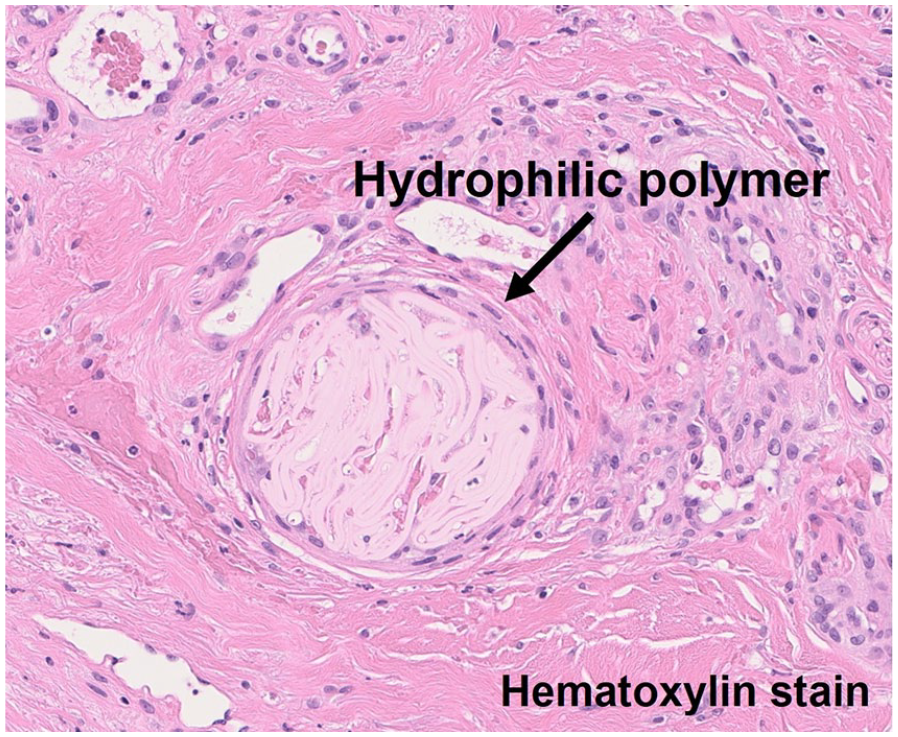
She presented with gangrene of her left heel (Panel B1, arrow) and purpura on her right toe and both lower limbs (Panels B2 and B3, arrows) a few days after discharge. Biopsy showed cutaneous intravascular aggregates of lamellated, nonrefractile, and colorless foreign material (Panel C, arrow), and hydrophilic polymer emboli (HPE) was diagnosed. The gangrene of her heel and purpura on both limbs gradually improved with conservative wound care.
Polymer coating technology of intravascular devices has decreased the invasiveness of percutaneous procedures and has been adopted worldwide. However, a US Food & Drug Administration safety communication raised concern and caution over HPE resulting from detached polymer particles embolizing downstream vessels. 1
Skin HPE findings are similar to those of cholesterol crystal emboli (CCE). However, in contrast to CCE, HPE treatment mainly consists of supportive care and does not require pharmacological intervention or surgery. 2 It is important to distinguish between HPE and CCE based on characteristic histological findings and appropriately treat them.2,3
Polymer coating technology lowers friction between devices and vessels; however, using large-diameter devices, vascular access associated with high friction (severe tortuous, calcification, and stenosis), and complex procedures (excessive manipulation, prolonged procedure, or multiple cannulation) have been reported to be risk factors for HPE.1,2 In this case, severe tortuosity and calcified nodules in the abdominal aorta may have interfered with the guiding sheath, even though it was a low-profile device, and resulted in HPE.
The development of devices, such as polymer-coated and low-profile devices, has enabled less invasive intravascular treatment for difficult-to-access cases; however, physicians should recognize the risk of HPE as an iatrogenic adverse event.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.