
Abstract

Aortic infections may be the result of hematogenous dissemination from a remote focal infection or direct invasion from an adjacent septic focus such as infection involving the intervertebral disc and the nearest vertebrae of the spine (spondylodiscitis). They are so rare that the exact incidence is unknown 1 ; however, the mortality rate is still 20% to 40%. 2 Diagnosis is challenging because clinical features are nonspecific. Radiological imaging is mandatory in the early detection of infective vascular complications and to plan the treatment strategy. We describe a rare case of penetrating aortic ulcer (PAU) of the descending thoracic aorta that arose during the hospitalization of a patient with spondylodiscitis.
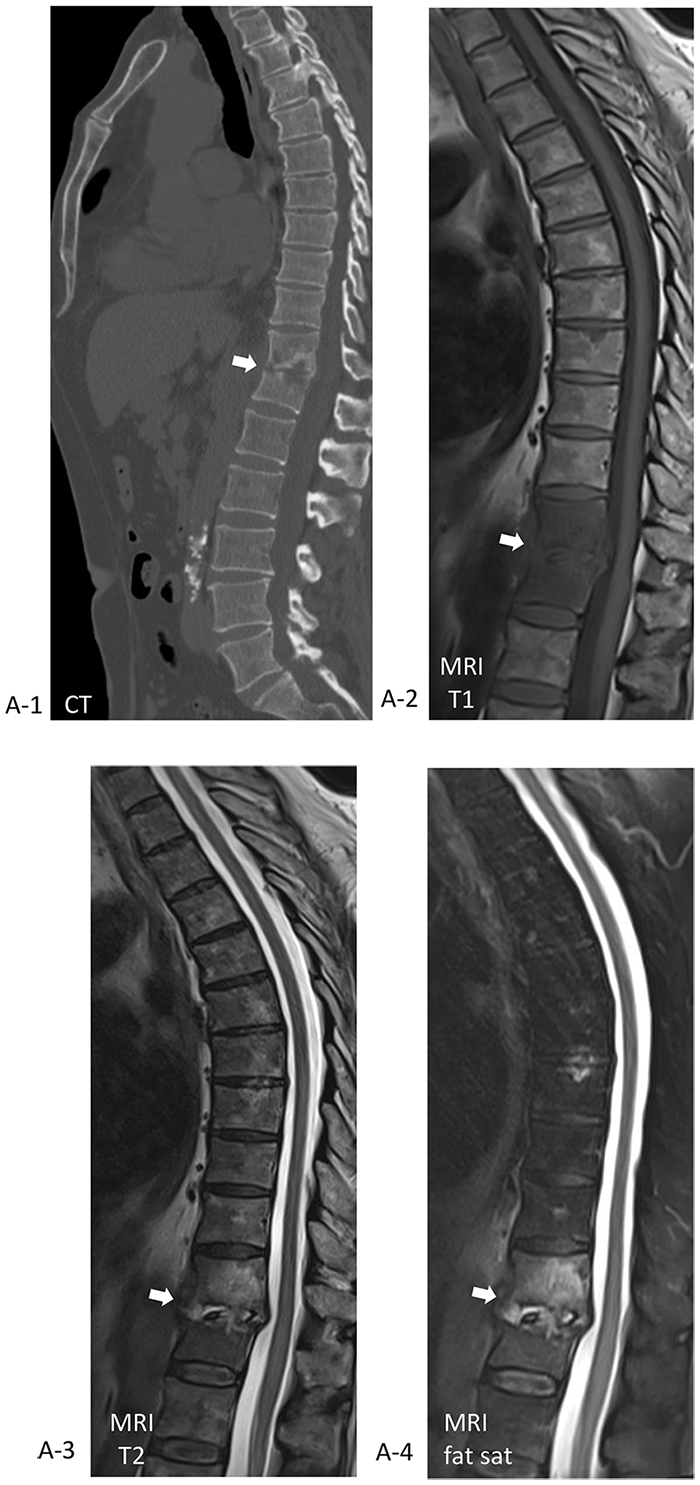
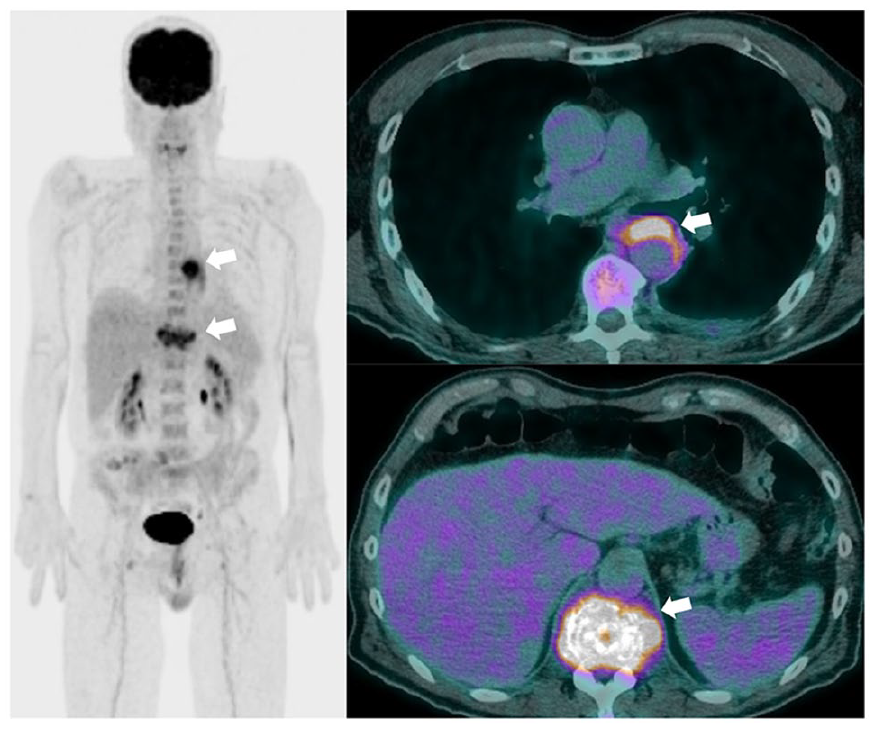
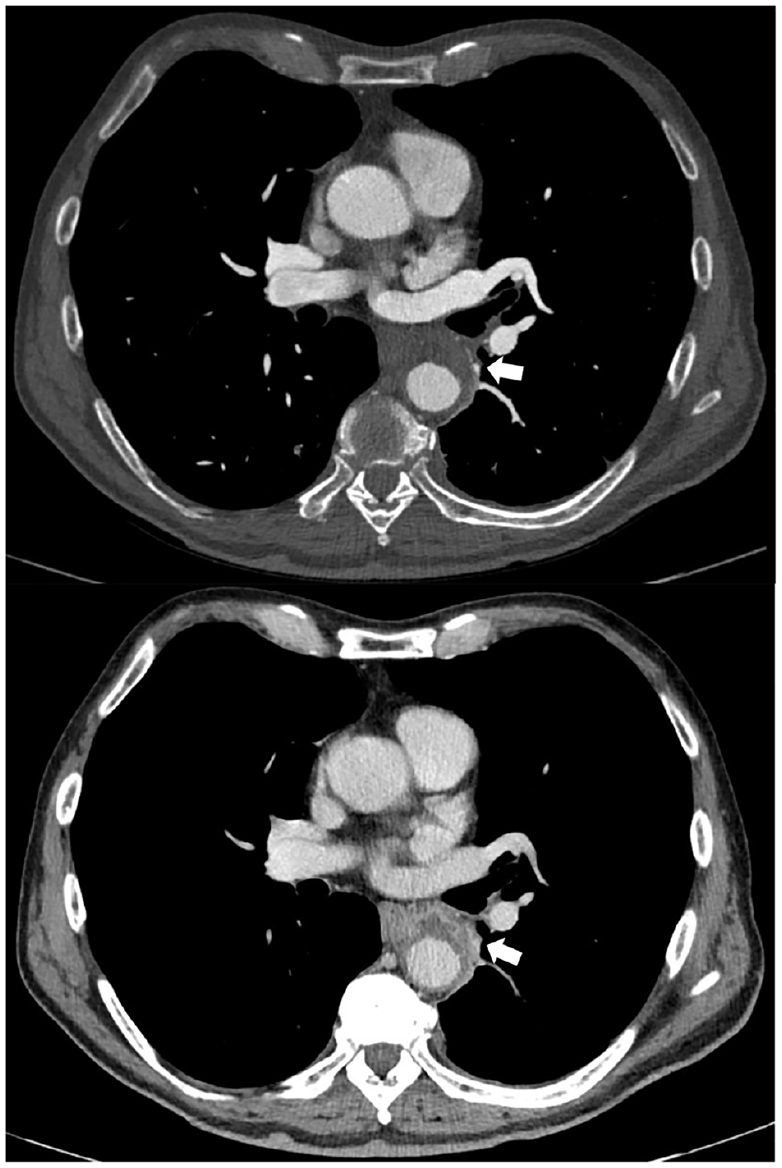
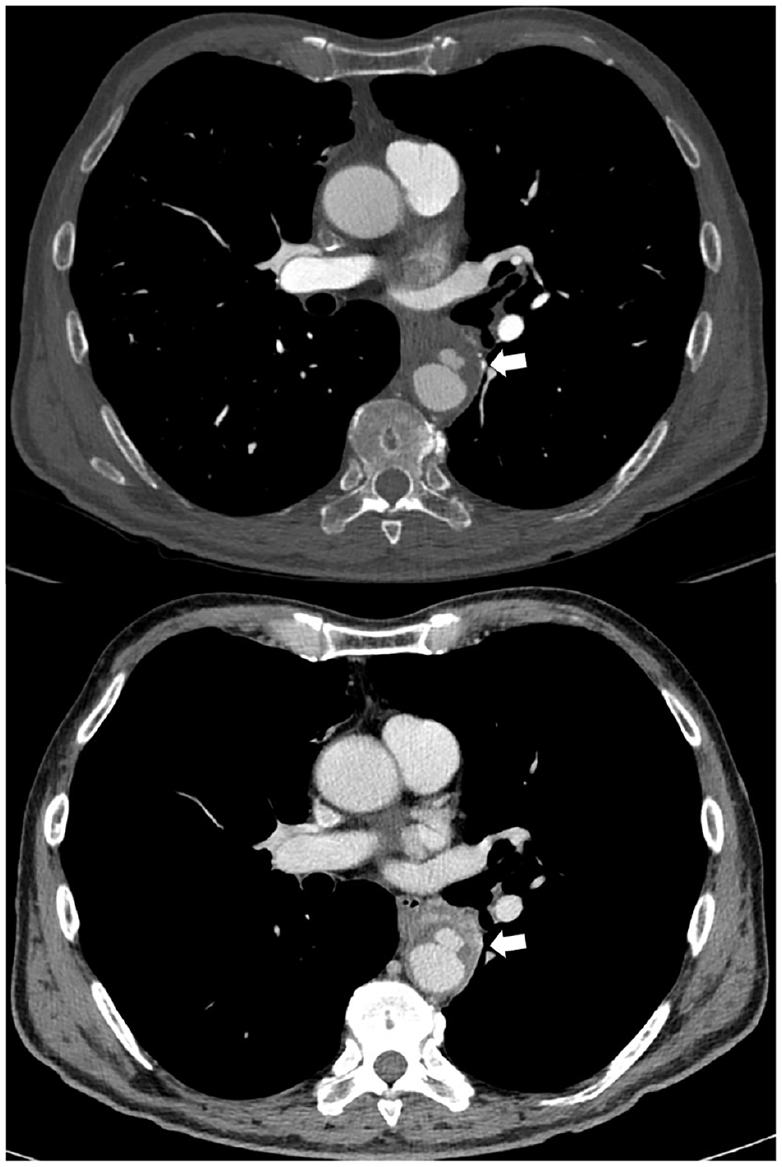
A 67-year-old man, with arterial hypertension and immunoglobulin G lambda monoclonal gammopathy, was admitted to our emergency department with a diagnosis of spondylodiscitis involving D11 and D12 vertebral bones following recently performed dorso-lumbar computed tomography (CT) (Panel A-1, arrow) and magnetic resonance imaging (MRI) (Panels A-2–A-4, arrows). On clinical examination, he had suffered severe back pain for 2 months, as well as fever and difficulty walking. Initial laboratory analysis revealed a C-reactive protein (CRP) level of 5.8 mg/L, a white cell count of 7.300/mm3, a hemoglobin level of 12.1 g/dL, and a creatinine level of 1.4 mg/dL. Blood culture isolated Streptococcus agalactiae and after infectious disease consultation the patient was started on appropriate intravenous antibiotic therapy – first with amoxicillin and clavulanic acid and then with cephalosporins. He became afebrile and resumed walking without aids after rehabilitation therapy. A 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET)/CT was performed a week later; it showed radiotracer uptake in the septic focus of the spine (SUVmax 9.1) and in the middle of the descending thoracic aorta (SUVmax 13.3) (Panel B, arrows). CT angiography (CTA) showed a PAU of the descending aorta (Type B) of 12 mm in depth – an additional finding and as a result of infective vascular damage that arose during the hospitalization (Panel C, arrows). Antibiotic therapy was continued until CRP level normalization was achieved for 2 consecutive weeks. According to general consensus, medical therapy with careful clinical follow-up and imaging surveillance are the treatment strategy of choice for Type B PAU. 3 However, CTA was repeated 10 days later: the PAU ulceration was wider with wall thickness reduction (Panel D, arrows). The CRP level stayed normal without antibiotics. Given the high risk of rupture, he underwent endovascular repair 4 weeks later.
Note – This figure is in color online.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.