
Abstract
The fluoropolymer-coated, paclitaxel-eluting Eluvia stent has shown promising results for the endovascular treatment of femoropopliteal artery lesions in patients with claudication. The aim of the current study was to evaluate efficacy and safety outcomes of the Eluvia stent for the treatment of long femoropopliteal lesions in Asian patients. This is a single-center, retrospective study. The primary endpoint was primary patency at 1 year. Secondary outcomes were 30-days complication rate, technical success, 1-year freedom from clinically driven target lesion revascularization (CD-TLR), limb salvage, survival, amputation-free survival (AFS), wound healing, and clinical improvement. A total of 64 patients with 67 femoropopliteal lesions were included; 78% suffered from diabetes and 84% had chronic limb-threatening ischemia (CLTI). Of those with ischemic wounds, 79% did not have run-off to the foot. Mean lesion length was 193 ± 128 mm and 52% were severely calcified. Primary patency at 1 year was 84% in the overall cohort and 91% in patients with complete lesion coverage with the Eluvia stent. Technical success was achieved in 100% of the cases and 30-day complications occurred in six patients. Twelve-month freedom from CD-TLR, limb salvage, survival, and AFS were 92%, 93%, 85%, and 80%, respectively. In 80% of patients, complete wound healing was experienced and 84% had clinical improvement after 1 year. The Eluvia stent showed promising 12-month patency and clinical results for femoropopliteal treatment in this CLTI-dominant patient population with severely calcified, long lesions. Patient numbers were, however, small; larger trials are required to validate these findings. Aneurysmal change seen in some cases also needs further investigation.
Keywords
Introduction
Endovascular treatment is the first choice for short femoropopliteal (FP) artery lesions. However, percutaneous intervention of long FP lesions remains challenging due to high rates of restenosis.1,2 Drug-eluting stents (DES) were introduced to help lower neointimal hyperplasia that causes restenosis. A recent meta-analysis showed favorable results with DES compared with balloon angioplasty and bare metal stents (BMS) in terms of lower rates of restenosis and target lesion revascularization. 3
The polymer-free, paclitaxel-eluting Zilver® PTX® stent (Cook Medical, Bloomington, IN, USA) was the first DES that showed good 5-year results for the treatment of short FP lesions in patients with claudication. 4 However, for patients with longer lesions, the Zilver PTX stent showed no superiority over BMS or balloon angioplasty.5–7
The Eluvia™ (Boston Scientific, Marlborough, MA, USA) is another paclitaxel-eluting vascular stent but, unlike Zilver PTX, is coated with a fluoropolymer. 8 In addition, Eluvia releases drug over a longer period of time: 12 months versus 2 months for the Zilver PTX.9,10 Early experience with the Eluvia stent for the treatment of short lesions in claudicants has shown promising results.11–13 The Eluvia stent was non-inferior compared with the Zilver PTX stent in 12-month primary patency and major adverse event rates, and showed significantly lower 12-month late lumen loss.11,14
Despite the good outcomes in these studies, there is limited evidence of the Eluvia stent in patients with chronic limb-threatening ischemia (CLTI) with long lesions. Therefore, the aim of the current study was to investigate the safety and efficacy of the Eluvia stent for the treatment of long FP artery lesions in an Asian patient population.
Methods
Study design and population
The study is a single-center, physician-initiated, retrospective study undertaken at Changi General Hospital, Singapore. The study was approved by the SingHealth institutional review board (IRB 2019/2493). Baseline data were collected from the electronic medical records of all patients. Procedural data were collected from the interventional report and visual assessment of the angiograms was by an experienced vascular surgeon.
Inclusion criteria included consecutive patients with symptomatic peripheral arterial occlusive disease who underwent stenting with the Eluvia DES system for the treatment of superficial femoral or popliteal artery disease between September 2016 and October 2018. Treatment with the Eluvia stent was performed on the discretion of the operator. Excluded were patients with acute limb ischemia, common femoral artery disease, use of DES to treat in-stent restenosis, drug-coated balloon (DCB) treatment of the same segment less than 1 month before, and patients who were subjected to bail-out stenting with DES after simultaneous DCB treatment of the same segment (i.e., double drug).
Patients with claudication were followed up at least once every 6 months until 2 years. Patients with CLTI were seen at least every 2 weeks by a vascular surgeon who also cared for their wounds according to the local protocol, until complete wound healing was achieved. Duplex ultrasound surveillance of the FP tract was performed at 12 months. Angiography was performed in case of suspicion of clinically relevant restenosis, meaning delayed or no wound healing, or deterioration of claudication, in the presence of restenosis determined by ultrasound. Ankle–brachial index or other indices of perfusion were not performed routinely as per institutional practice due to a high prevalence of calcified vessels below-the-knee.
Study device
The Eluvia stent consists of a primer layer of poly n-butylmethacrylate (PBMA). The second layer above the primer layer comprises of an active layer of paclitaxel (at a concentration of 0.167 μg/mm2 stent surface area) and the fluoropolymer, polyvinylidene fluoride-co-hexafluoropropylene (PVDF-HFP). The biocompatible fluoropolymer allows the gradual elution of paclitaxel over a 12-month period. The diameter and length range of the stent are 6–7 mm and 40–120 mm, respectively.8,10
Procedure overview
All patients received antiplatelet therapy with 100 mg of aspirin at least 7 days prior to the procedure. Dual antiplatelet therapy consisting of aspirin and clopidogrel was prescribed for 6 months after the procedure, followed by lifelong monotherapy with either one of the medications. Patients who required anticoagulation for other indications were maintained on anticoagulant agents with additional clopidogrel therapy 6 months after the procedure. Patients with aspirin allergy received lifelong clopidogrel and vice versa.
Diagnostic angiography was performed via antegrade or crossover access. Two orthogonal magnified angiographic projections of the target lesions were obtained prior to the intervention. After angiography, systemic intra-arterial heparinization was performed as per the institutional protocol.
A 0.018 or 0.035-inch guide wire was passed through the target lesion and predilatation with a balloon catheter was performed. The predilatation balloon was sized 0.5 mm less than the reference vessel diameter (RVD), which was visually assessed. The balloon was routinely inflated for a minimum of 90 seconds. If there was a suboptimal result to balloon angioplasty due to dissection or recoil of more than 50%, the patient was considered for stenting with DES. Prior to DES implantation, the vessel was again predilated with a semi-compliant balloon (Mustang™ Balloon; Boston Scientific) sized 1:1 to RVD at aggressive pressures (approximating burst) to facilitate optimal stent expansion. Non-compliant balloon angioplasty was used when results were suboptimal. RVD was determined by visual assessment of the operator during the procedure and confirmed on angiographic response to predilatation. Stents were sized 1 mm larger than the RVD. Stenting of distal segments was performed before proximal segments and stents were overlapped at least 1 cm in length, with careful consideration to avoid geographic miss. Total lesion coverage with DES was preferred and left to the discretion of the operator but not mandatory. When used in combination with a DCB, maximum overlap of 1 cm between the stent and DCB was allowed whilst ensuring that the whole lesion was covered by either DES or DCB (hybrid drug coverage). Hybrid drug coverage was used to limit the length of the stents in the target vessel. In these cases, segments that responded well to predilatation were treated with DCB and those segments with recoil after predilatation were stented with DES. A 1-cm segment of overlap between the DCB segment and the DES segment was used to avoid geographic miss, which can happen due to parallel errors, and ensure that the whole lesion was covered with drug. A combination with BMS was also possible and used as bail-out in the initial experience.
Post-dilatation was routinely performed with a less compliant balloon (e.g., Mustang Balloon) or a non-compliant balloon with a size at least equivalent to the RVD within the treated area to ensure no geographical miss.
Supplementary iliac stenting and below-the-knee therapy was performed simultaneously in the same setting if required. Coronary everolimus-eluting stents (XIENCE PRIME; Abbott Vascular, Santa Clara, CA, USA) were occasionally used below-the-knee for bail-out stenting in combination with plain balloon angioplasty (POBA) but no DES were used for the iliac arteries.
Study endpoints
The primary endpoint was 1-year primary patency, defined as freedom from restenosis or occlusion on ultrasound or angiography without any clinically driven target lesion revascularization (CD-TLR) or bypass. Significant restenosis on duplex ultrasound was defined as peak systolic velocity ratio (PSVR) ⩾ 2.4. Angiographic definition of restenosis was > 50% on orthogonal views.
Secondary endpoints were 30-day complication rate, technical success, and 1-year freedom from CD-TLR, limb salvage, survival, amputation-free survival (AFS), complete wound healing (full epithelization of wound), and clinical improvement. Technical success was defined as delivery and deployment of the study stent to the target lesion to achieve residual angiographic stenosis ⩽ 30%, assessed visually on final angiogram. Major amputation was defined as amputation above the ankle. Survival was defined as freedom from all-cause death. Clinical improvement was defined as complete wound healing, resolution of rest pain or improvement of claudication by at least one Rutherford class. Clinical improvement was evaluated during outpatient follow-up visits.
Statistical analysis
Baseline characteristics and procedural information are presented as mean with SD or median and IQR in case of continuous data, and as numbers with percentages in case of categorical data. Kaplan–Meier (KM) analysis was performed to estimate the primary patency, freedom from CD-TLR, survival, limb salvage, and AFS at 12 months. Subgroup analysis for primary patency was performed for patients with TASC C and D lesions. Also, primary patency analysis between total lesion coverage with Eluvia stents, the combination of Eluvia and DCB (hybrid drug coverage), and the combination of Eluvia and BMS or POBA, was performed. Statistical significance was defined as a p-value less than 0.05. Statistical analysis was performed using IBM SPSS 26.0 software (IBM Corp., Armonk, NY, USA).
Results
Baseline patient and lesion characteristics
A total of 64 patients were enrolled in the study with a mean age of 70 ± 12 years. A total of 67 FP lesions were treated with 146 Eluvia stents. Three patients had bilateral treatment. Rutherford category 4 or 5 (i.e., CLTI) accounted for 84% of the limbs. Mean lesion length was 193 ± 128 mm; 48% of the lesions were occlusions and 52% were severely calcified according to the Peripheral Academic Research Consortium (PARC) classification. Before revascularization, 60% of the patients had 0 or 1 tibial run-off vessels. Table 1 summarizes the baseline patient and lesion characteristics.
Baseline patient and lesion characteristics.
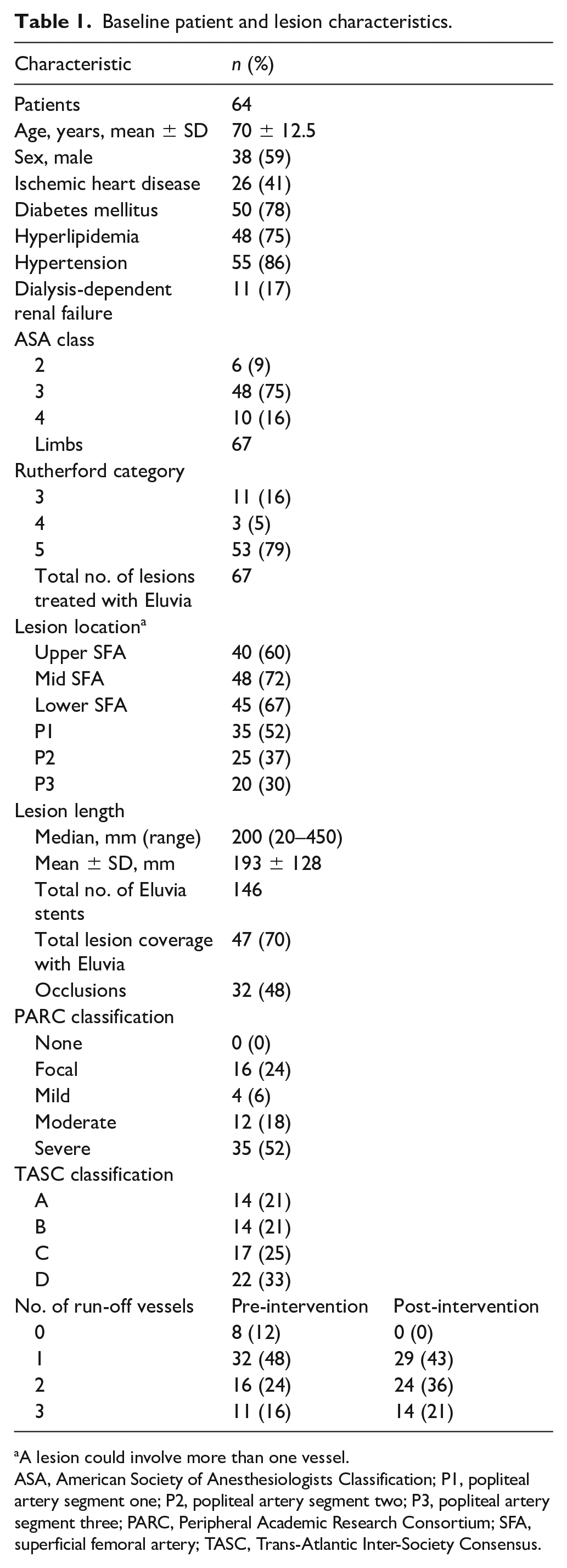
A lesion could involve more than one vessel.
ASA, American Society of Anesthesiologists Classification; P1, popliteal artery segment one; P2, popliteal artery segment two; P3, popliteal artery segment three; PARC, Peripheral Academic Research Consortium; SFA, superficial femoral artery; TASC, Trans-Atlantic Inter-Society Consensus.
Procedural endpoints
The mean radiologic follow-up was 11.3 ± 7.8 months. Technical success was achieved in all cases. Complications within 30 days after the intervention occurred in six patients: two patients developed a pseudoaneurysm of the groin that was managed with either compression or thrombin injection, two patients had a hematoma on the access site that did not require transfusion and were treated conservatively, one patient experienced a myocardial infarction, and one patient died from a myocardial infarction.
Primary endpoint
The primary patency at 1 year for the total cohort was 84%. In the subset of patients with TASC C and D lesions, primary patency was 86%. This subgroup consisted of 49% severely calcified lesions and a mean lesion length of 280 mm (± 97).
A subgroup of the total cohort with severely calcified lesions (n = 35) was also analyzed and showed a 1-year primary patency of 82%.
Analyzing patients per type of lesion coverage, 1-year primary patency was the highest (91%) for total lesion coverage with Eluvia stents, followed by 80% for hybrid drug coverage, and 42% for Eluvia and BMS or POBA coverage (Figure 1). Baseline characteristics did not differ significantly between the groups. The group with total lesion coverage, with 60%, TASC C and D lesions, the hybrid group 46%, and the Eluvia plus BMS or POBA group 72%. The group with total lesion coverage had, with 60%, more severely calcified lesions than the hybrid (23%) and Eluvia plus BMS or POBA groups (29%). Run-off was poorest in the hybrid group, with 31% with zero run-off vessels, versus 9% and 0% in the total lesion coverage and Eluvia plus BMS or POBA groups, respectively. Mean lesion lengths for the subgroups were 201 ± 136 mm for the total lesion coverage group, 153 ± 86 mm for the hybrid group, and 211 ± 143 mm for the Eluvia plus BMS or POBA group. Primary patency for lesions with a length ⩾ 150 mm and total lesion coverage with Eluvia stents (n = 27) was 90% after 12 months.
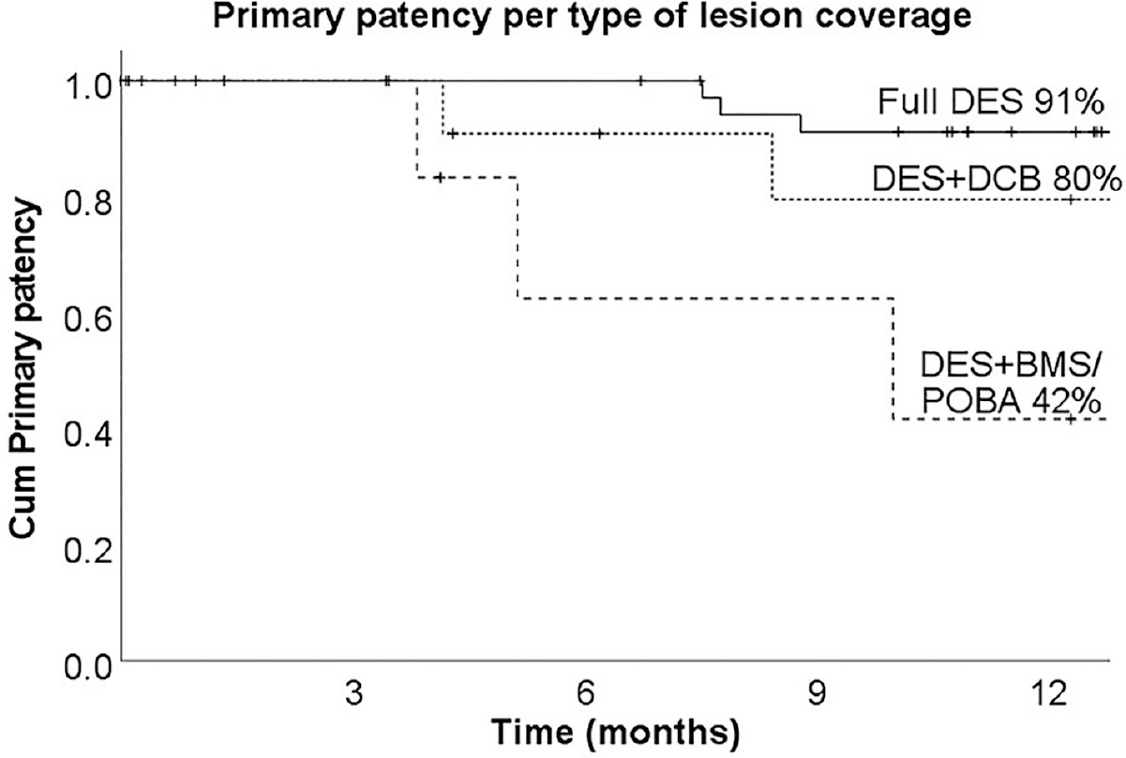
Primary patency rate based on the type of lesion coverage.
Secondary endpoints
Freedom from CD-TLR was 92% at 12 months after the index intervention. No major amputations were performed within 30 days after the procedure. Limb salvage was 93% at 12 months. Survival rate at 12 months was 85% and AFS 80%. Forty-four of 55 limbs with wounds (80%) experienced complete healing within 12 months. Clinical improvement was achieved in 56 out of 67 patients (84%) in the same period.
Three patients developed visible absence of wall apposition to the stent exceeding the diameter of the stent. Two of these were detected at 5 and 20 months postintervention and were occluded. The other one was asymptomatic and diagnosed at 22 months after the procedure. This patient refused intervention at the time of follow-up.
Discussion
The paclitaxel-eluting Eluvia stent showed good clinical and patency outcomes for the treatment of femoropopliteal artery disease in patients with claudication. The current study is the first investigating the Eluvia stent in a CLTI predominant population showing promising results for the treatment of long, severely calcified FP lesions in patients with compromised run-off.
Our patient population seemed more complex when compared to prior studies with the Eluvia stent in long (> 150 mm) FP lesions. The population in the current study comprised of 84% patients with CLTI compared with 48% in the MUENSTER registry and < 5% in the IMPERIAL long lesion cohort.15,16 Besides, the prevalence of diabetes mellitus among our study subjects was higher: 78% vs 37% in the MUENSTER registry and 40% in the IMPERIAL long lesion cohort. Furthermore, the prevalence of renal insufficiency and dialysis-dependent renal failure reported in the previous studies was 5–6%, compared to 17% dialysis-dependent renal failure in ours.
Besides differences in patient population, lesion complexity also varied. Severely calcified lesions were reported in 52% of our patients, similar to the 42% moderate/severe calcification noted in the MUENSTER registry, but was higher than the 28% in the IMPERIAL long lesion cohort. In addition, our study had more mid- and distal popliteal involvement compared with the other studies; close to 30% of our lesions involved the mid to distal popliteal artery. The degree of run-off vessels to the foot was also poorer in our study when compared to the MUENSTER registry: only 40% had ⩾ 2 run-off vessels versus 80% reported in the MUENSTER registry. In addition, for patients in our study with ischemic wounds, 79% did not have direct flow to the foot on preintervention angiogram. However, the number of total occlusions was higher in the MUENSTER registry.
Despite a more complex patient population, a larger proportion of CLTI with poorer run-off, primary patency, and freedom from CD-TLR rates are comparable to those in the MUENSTER registry and IMPERIAL long lesion cohort. It is important to note, however, that the MUENSTER registry used a more stringent duplex criteria to define primary patency (PSVR ⩽ 2.0) whereas we used a PSVR of ⩽ 2.4 in line with the IMPERIAL study.
Compared with the Zilver PTX stent, patency and freedom from CD-TLR rates in our study are higher than most results reported on the Zilver PTX stent.5,6,17–19 Whereas a direct comparison cannot be made, since this is not a randomized trial, the results are in line with the IMPERIAL trial, which showed significantly higher patency and lower major adverse event rates with Eluvia compared with Zilver PTX in claudicants. 12
Another interesting finding is that total lesion coverage was achieved in 70% of the lesions with a corresponding patency rate of 91% in these lesions. This patency rate was better compared with hybrid drug coverage with the Eluvia stent and DCB or the combination of Eluvia and BMS or POBA, while the total lesion coverage group had the highest proportion of severely calcified lesions. This seems to suggest that total lesion coverage with prolonged controlled drug elution combined with a stent scaffold could be a viable solution in long calcified lesions. However, owing to the small numbers and retrospective study design, no inference can be made and this is hypothesis generating at best. The respectable patency results could also be explained by the aggressive pre- and post-dilatation in all patients. The importance of standardized vessel preparation has been described before.20,21
Regarding safety of the Eluvia for treating FP lesions, visible absence of wall apposition to the stent was reported in three patients in our study (4.5%). This was first reported in the MUENSTER registry with a prevalence of 8%. 16 All three patients in the current study had full lesion coverage with Eluvia stents. Two of them had occluded stents while the stent was still patent in the third patient. The possibility of this observation being related drug elution must be further explored.
Study limitations
This study has some limitations. The major one is the retrospective study design. Owing to this, there was heterogeneity in the follow-up schedule. Besides, no routine duplex ultrasound or angiography follow-up of the patency of the below-the-knee vessels was performed as per institutional protocol; however, this was also not recommended by guidelines.22,23 Furthermore, clinical improvement was not reported in a standardized way by questionnaires but was obtained from reports during outpatient visits. Another limitation is that during the study period Eluvia was chosen randomly by different operators, which could be a source of bias. Owing to a shortage of long Eluvia stents, many patients received more than one Eluvia stent to fully cover the lesion. On the other hand, this reflects daily clinical practice and therefore shows results from real-world practice. Further, our study did not have a control arm and therefore extrapolation of study results and its comparison with other studies should be done cautiously. We carried out a subgroup analysis for the type of lesion coverage; however, the number of patients in each group was too small to draw firm conclusions.
Conclusion
In conclusion, this study demonstrated promising 1-year stent patency and clinical outcomes with the Eluvia stent in severely calcified, long FP lesions in patients with predominantly CLTI and poor run-off. Owing to the non-comparative retrospective study design and small subgroups, a well-powered prospective study is needed to validate our study findings. Presumptive aneurysmal change on duplex ultrasound, defined as visible absence of wall apposition to the stent exceeding the diameter of the stent on transverse section, in a minority of cases should be subject of further systematic investigations.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S Kum and CEVB Hazenberg are consultants to Boston Scientific. The other authors report no relevant disclosures.
Funding
The authors received an education grant for travel from Boston Scientific. Boston Scientific had no role in the study design; collection, analysis, and interpretation of data; writing of the manuscript; and there were no restrictions regarding publication.