
Abstract
This study aimed to investigate the effects of supervised exercise training (SET) on walking performance and spatiotemporal gait changes in patients with symptomatic lower extremity peripheral artery disease (PAD). In this single-arm prospective nonrandomized cohort study, patients with Fontaine stage II PAD following a 3-month SET program were included. Before and after SET, a constant-load treadmill test was performed to determine the pain-free and maximal walking distances (PFWD and MWD, respectively). During this test, spatiotemporal gait parameters were assessed. The ankle–brachial index (ABI) and toe–brachial index (TBI) were also measured. Twenty-seven patients with PAD (64.0 ± 1.9 y, 74% men) were included. Following SET, the PFWD (+68%; p = 0.001) and MWD (+79%; p ⩽ 0.001) significantly increased. The ABI and TBI did not change significantly. Following SET, the stride duration, stride frequency, stride length, and double support phase duration did not change significantly. In contrast, subphases of stance showed significant changes: the loading response (+8%; p = 0.03) and foot-flat (+2%; p = 0.01) phases were significantly longer, whereas the push-off phase (–7%; p = 0.002) was significantly shorter. A significant positive correlation was found between changes in the foot-flat phase and changes in PFWD (r = 0.43, p = 0.03). A significant negative correlation was found between changes in the push-off phase and changes in PFWD (r = −0.39, p = 0.05). No significant correlations were found between changes in relative durations of the subphases of stance and MWD. These results indicate that changes in temporal gait parameters during the foot contact phase potentially constitute an underlying mechanism of delayed claudication distance in patients with symptomatic PAD.
Keywords
Introduction
Intermittent claudication is a typical symptom of lower extremity peripheral artery disease (PAD). 1 The clinical manifestation of intermittent claudication is cramping lower limb pain occurring during exercise and resolving with rest. 1 Patients with PAD have impaired muscular strength and walking performance, and they experience a faster decline in function than do healthy age-matched subjects.2–4 This decline in function may decrease their quality of life. 5
Muscle weakness and poor endurance of the lower limb muscles may also be related to altered gait patterns in patients with PAD.6–10 Previous studies have shown that patients with PAD have a slower walking speed and step frequency, have a shorter step length, and spend more time in stance phase.11–13 These differences are present even before the development of pain,9,11,12 which may affect walking economy and fatigue, making ambulation challenging to execute in daily life. 14
Supervised exercise training (SET) is one of the recommended first-choice therapeutic options for symptomatic patients with lower extremity PAD.1,15 SET improves individuals’ walking capacity (e.g. pain-free (PFWD) and maximal (MWD) walking distance) and quality of life.16–20 Improvements are generally not accompanied by hemodynamic (ankle–brachial index, ABI) changes, 18 suggesting that other potential mechanisms are implicated.20,21 Gait pattern change is one potential mechanism that deserves further investigation. Results observed in the current literature suggest that different gait adaptations exist between an acute exercise (single bout) and a chronic (pre- vs post-intervention) response to SET in patients with PAD.
First, it has recently been showed that, during an acute bout of treadmill walking, patients with PAD modify temporal gait parameters of the subphases of stance (foot-flat and push-off). 12 The results of that study 12 showed that once claudication is established, the duration of foot-flat increases and the duration of the propulsion phase decreases compared to those under a pain-free walking condition. Although the mechanism is not fully understood, 12 it might be hypothesized that the longer duration of the foot-flat phase may favor better muscle oxygenation and stability, whereas the shorter duration of the propulsion phase may be related to the fatigue or inefficiency of ischemic calf muscles. 4 Nevertheless, the effects of SET on the evolution of these parameters over an acute bout of treadmill walking remain to be investigated.
Second, although chronic SET does not change spatiotemporal gait parameters, such as step length, step frequency, and stance and swing durations,10,22,23 it has recently been shown that SET modifies the hip and ankle kinematics and kinetics during foot-flat and push-off phases in patients with PAD. 24 Indeed, following 6 months of SET, improved ankle power absorption during foot-flat and ankle power generation during the push-off phase have been observed. 24 This finding suggests improved participation of the plantar flexors during walking following chronic SET. 24 As the plantar flexion angle and torque remain unchanged after SET, 24 we can deduce that increased ankle power generation during the push-off phase is likely related to an increased angular speed due to a shortened propulsion time. However, Schieber et al. 24 and other authors did not yet specifically investigate the effects of chronic SET on temporal gait parameters of the subphases of stance in patients with PAD.
The aim of the present study was to investigate changes in walking performance and spatiotemporal gait parameters (both assessed during the treadmill test) at both acute (single bout) and chronic (pre- vs post-intervention) response to SET in symptomatic patients with PAD. It was hypothesized that: (1) 3 months of SET would improve walking performance by increasing PFWD and MWD (chronic adaptations); (2) since PFWD would be increased, the changes in the stance phase associated with the onset of claudication (shorter duration of the propulsion phase along with longer duration of the foot-flat phase; similar acute adaptations to the maximal walking test) would be delayed during the maximal walking test after SET; and (3) SET would shorten propulsion time (chronic adaptations).
Methods
Study population
In this single-arm prospective nonrandomized study, symptomatic patients with PAD taking part in the Angiofit study conducted at the Division of Angiology, University Hospital of Lausanne, Switzerland were included. In brief, the Angiofit study includes a longitudinal observational cohort of symptomatic (Fontaine stage II) patients with chronic PAD participating in the clinical SET program. The inclusion criteria of the SET program are stable uni- or bilateral lower limb claudication (Fontaine stage II) and a resting ABI ⩽ 0.9 or an ABI decreased postexercise by > 20%. 1 The exclusion criteria of the SET program are the inability to participate in the SET program three times per week, critical limb ischemia, and a cardiac contraindication to exercise. 25 In this study, we included all patients with walking performance and spatiotemporal gait parameter data during the treadmill test before and after SET. Patients were excluded from these analyses if they suffered from neurological and neuromuscular disorders and other comorbidities (orthopedic, rheumatologic) leading to gait abnormalities. The Angiofit study was approved by the local ethics committee and was conducted according to the Declaration of Helsinki. All subjects provided written, voluntary, informed consent before participation.
Multimodal supervised exercise training (SET) program
Patients participated in the clinical SET program, which was coordinated by an angiologist and supervised by an exercise physiologist specializing in vascular rehabilitation (SL). 26 In line with recent guidelines,1,20 the SET program consisted of 36 sessions lasting 30–60 min over a 3-month period (3×/week).
Twice weekly, patients performed outdoor Nordic walking; once weekly, they performed indoor circuit training focused on the strengthening and endurance of the lower limbs. 26 Including a combination of these two training modalities allowed us to focus concomitantly on the main parameters (strength and endurance of the lower limbs) that describe functional decline in patients with PAD. In addition, Nordic walking may improve walking performance and reduce pain during exertion to a greater extent than walking without poles, despite the level of cardiovascular stimulation being higher. 27 Poles may also be useful and safe because patients with PAD sometimes have impaired balance. 28 The outdoor Nordic walking sessions were performed over 150 m of level ground. The patients were asked to walk back and forth and were supervised during all walking sessions. During these sessions, the patients were encouraged to exercise until moderate–severe claudication developed.20,29 The patients restarted the exercise when the pain disappeared. Borg’s scale was used to monitor the training intensity during each walking session. 30 At the beginning of the SET program, the patients exercised at a low intensity (9–11 on Borg’s scale). Afterwards, if tolerated, the patients were encouraged to exercise at a moderate or moderate-to-vigorous intensity (12–16 on Borg’s scale). 30
The indoor circuit training program was mainly composed of five to six stations, at which the patients remained for 2–4 min each, and at least two circuits were performed during each session. Each station included specific functional walking (toe/heel, high knees, side-to-side, backward walking) or resistance exercises focused on the main lower limb muscles (squat, calf/heel raise, lunges) using body weight, dumbbells or elastic bands. At the beginning of the SET program, each station had a 2-min duration. The patients were asked to perform 5–15 repetitions of each exercise using body weight interspersed with 30–60 s of recovery and were encouraged to exercise at low exercise intensity (9–11 on Borg’s scale). Subsequently, if tolerated, the patients were encouraged to exercise at a moderate intensity (12–14 on Borg’s scale). To that end, the duration of each station progressively increased to 4 min, and the patients were encouraged to perform 20–30 repetitions of each resistance exercise using body weight or 10–20 repetitions using dumbbells (from 1 to 5 kg) or elastic bands.
The sessions started with a 5–10 min warm-up focused on coordination and balance, and ended with a 5 min cool-down period. During the first month of SET, the patients also participated in 6-h structured therapeutic education workshops so that the patients with PAD received information on nutrition, physical activity, tobacco use and cardiovascular risk factors. SET adherence was defined as the percentage of attended sessions out of the total number of sessions. Usually, the SET program had a 3-month duration (90 days). However, by reasons of sickness or holidays, we allow patients to have two additional weeks to complete the SET program.
Assessments
All assessments were performed both 1–2 weeks before and after SET.
Physical characteristics
The patients’ medical histories were assessed thoroughly, and physical examinations were performed. Body mass index, resting heart rate, and systolic and diastolic blood pressure were recorded.
Vascular parameters
The ABI and toe–brachial index (TBI) were measured in the supine position. 1 The resting ABI was measured using a hand-held 5-MHz Doppler flow meter (Atys Medical, France) and calculated as the ratio of the ankle (dorsalis pedis and posterior tibial) systolic blood pressure on both sides to the highest humeral systolic pressure. The ABI was also measured postexercise. 1 The resting TBI was calculated using photoplethysmography (Atys Medical, France) as the ratio of the toe pressure to the highest humeral systolic pressure. The highest resting ABI and TBI values corresponding to the most symptomatic leg were considered.
Constant-load treadmill test
As spatiotemporal gait parameters are influenced by speed and slope,31,32 a constant-load treadmill test was performed. 20 The test was usually performed at 3.2 km/h with a 12% slope. However, for some patients, speed was adjusted (from 2.0 to 3.2 km/h) according to the patient’s level of tolerance, safety and feasibility, ensuring that the same parameters were used before and after SET. The PFWD and MWD were assessed. 20
Spatiotemporal gait parameters
To measure spatiotemporal gait parameters during the constant-load treadmill test, the patients wore two validated inertial sensor units from Physilogs® (Gait Up, Switzerland) integrating a microcontroller, memory unit, 3-axis accelerometer (range ± 3 g), gyroscope (range ± 800°·s−1), and battery; these components were contained in a small and lightweight unit attached to the feet with an elastic Velcro strap.33,34 These sensors, with a dedicated algorithm, were previously validated to assess gait patterns in young 34 and older adults.33,34 The accuracy and precision were demonstrated to be good, and the sensors showed excellent repeatability across measurements. 34 Before the treadmill test was started, the sensors were turned on with the patients in the standing position (automatic calibration).
Spatiotemporal gait parameters were continuously recorded during the treadmill test, but only 10 consecutive strides were selected and analyzed at three different time points. First, during pain-free walking (Pain-free), 10 strides after 1 min of pain-free walking at constant speed were selected. Second, regarding the pain condition (Pain), 10 strides were selected after the development of pain. Third, regarding the end of the test (End), 10 strides were selected before the end of the test, ensuring that the patients walked at a constant speed. The data were sampled at a frequency of 200 Hz and then low-pass filtered at 17 Hz.33,34 The temporal parameters assessed were stride duration and stride frequency and relative duration (% of gait cycle duration) of the swing, stance, and double support phases. The relative durations of the subphases of stance (loading response, foot-flat, and push-off) were also reported.33,34 The spatial parameter assessed was stride length. Both legs (the most symptomatic leg and less/non-symptomatic leg) were assessed. The symmetry between the two legs was assessed at each time point. To that end, the spatiotemporal gait parameters of the most symptomatic leg were divided by those of the less/non-symptomatic leg.
Statistical analysis
Based on the data of 85 patients with PAD who previously participated in our clinical SET program, 26 a sample size of 24 and 16 patients was needed to detect significant differences in PFWD and MWD after SET, respectively (power 80%; α = 5%). The data are expressed as mean ± SE. The normality of the distributions was visually and statistically (Kolmogorov–Smirnov test) assessed. Two-way repeated measures ANOVA [time (pre vs post) × exercise duration (pain-free vs pain vs end)] was performed to assess the inter-limb symmetry of the spatiotemporal gait parameters. The same analysis was used to compare the spatiotemporal gait parameters in the most symptomatic leg only. This analysis allows identifying differences between pre–post-intervention (time effect; chronic response to SET) and within the maximal treadmill test (exercise duration effect; acute adaptations). When repeated measures ANOVA revealed a significant main effect (time or exercise duration) or interaction effect, multiple comparisons with Bonferroni adjustments were performed to test the significance of the differences. A paired t-test was used to compare walking performance and vascular and physical characteristics before and after SET. Partial correlation was run to determine the relationship between changes in the relative durations of the subphases of stance and changes in walking performance following SET (i.e. delta), whilst controlling for gait baseline values. All statistical analyses were performed with IBM SPSS version 26 software (IBM Corp., Armonk, NY, USA). The level of significance was set to be p ⩽ 0.05.
Results
Study population
Twenty-seven patients with PAD were recruited and completed the SET program (Table 1). The pharmacological therapy provided before and after SET was similar for each patient, except that one patient stopped receiving antihypertensive therapy, and two patients started statin therapy during SET. During SET, two patients resumed smoking.
Baseline characteristics of the study population.
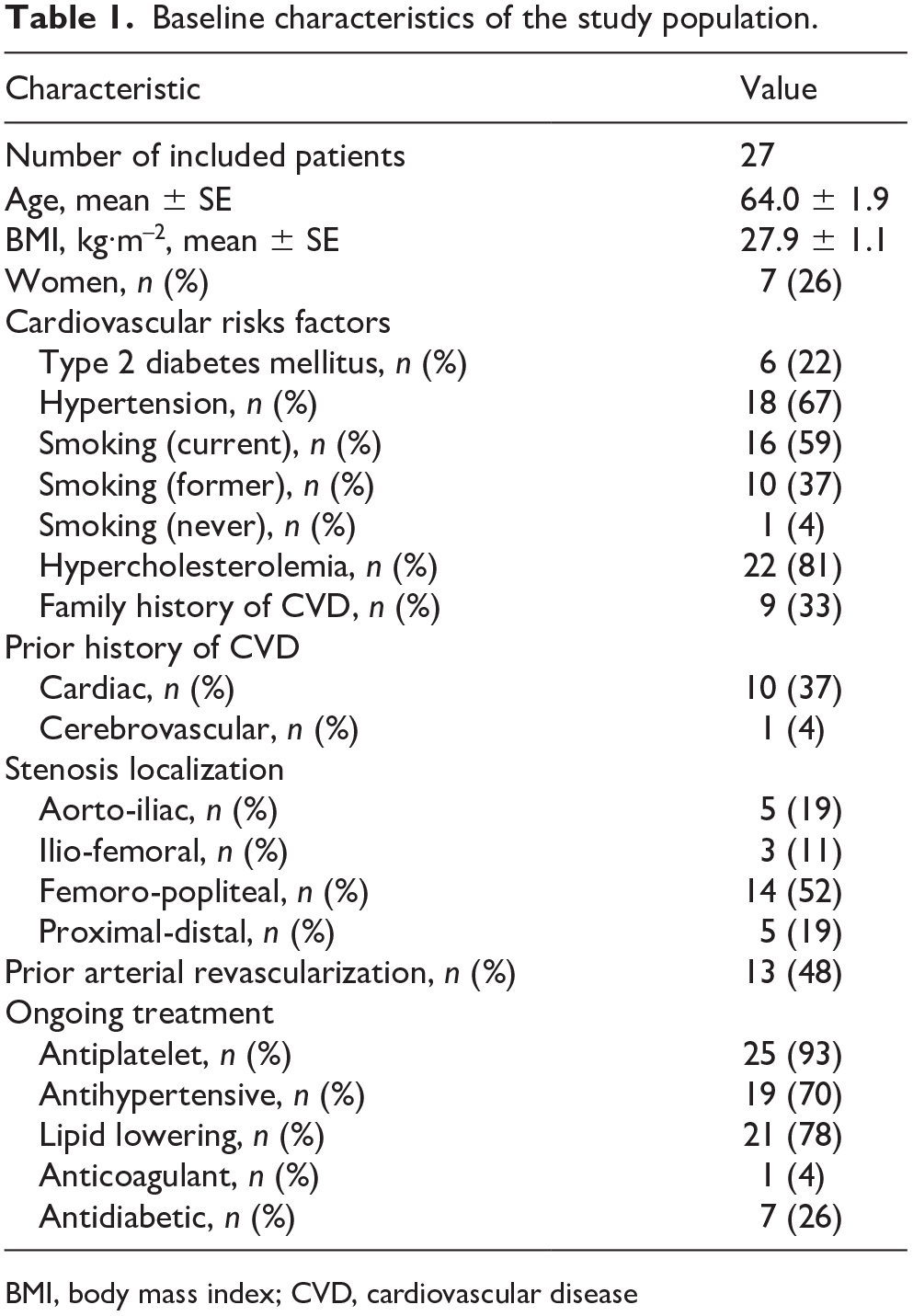
BMI, body mass index; CVD, cardiovascular disease
Characteristics of training
The mean number of sessions patients participated in was 35 sessions, and the mean training duration was 97 days. The rate of adherence to SET was 97% (83–100%). On average, the patients spent 66% (61–72%) of the SET program performing Nordic walking and 34% (28–39%) of the program performing strengthening exercises for the lower limbs.
Walking performance, vascular parameters, and physical characteristics
PFWD (+68%) and MWD (+79%) significantly increased after SET (Table 2). The ABI and TBI did not change significantly (Table 2). Body mass index, resting heart rate, and systolic and diastolic blood pressure remained unchanged after SET (Table 2).
Walking performances, vascular parameters, and physical characteristics before and after supervised exercise training.
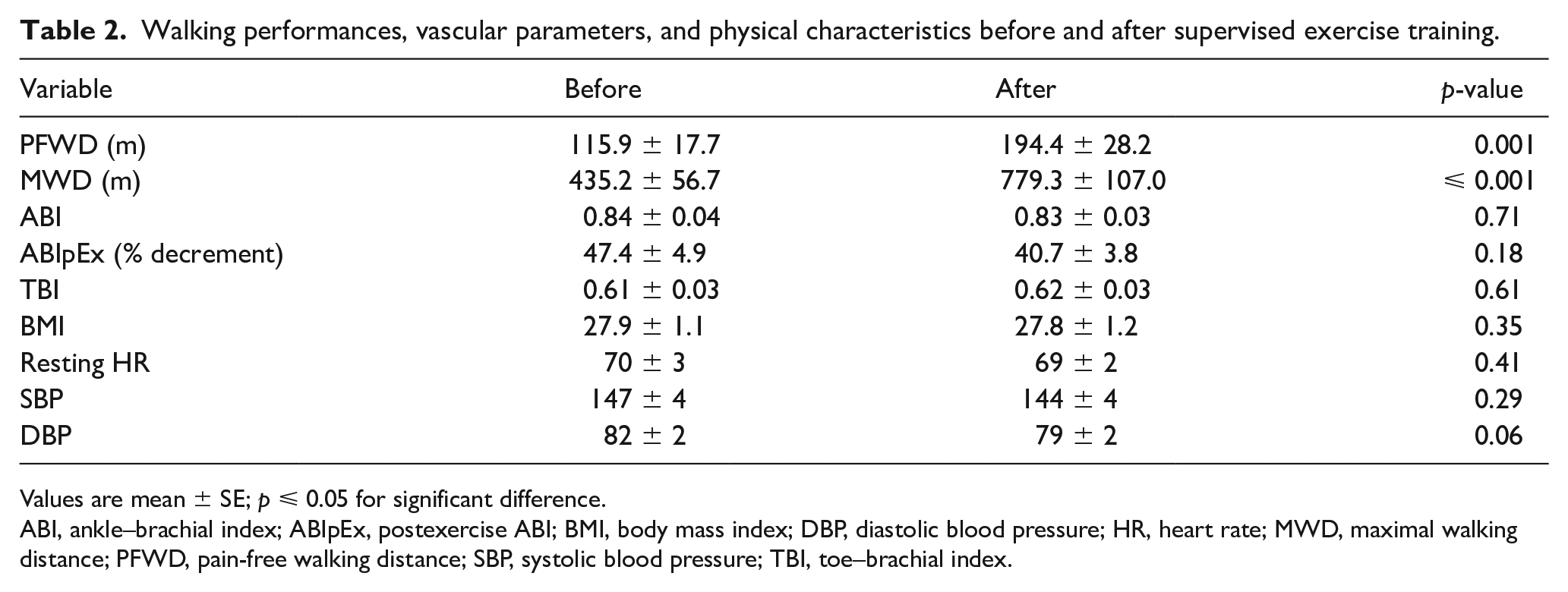
Values are mean ± SE; p ⩽ 0.05 for significant difference.
ABI, ankle–brachial index; ABIpEx, postexercise ABI; BMI, body mass index; DBP, diastolic blood pressure; HR, heart rate; MWD, maximal walking distance; PFWD, pain-free walking distance; SBP, systolic blood pressure; TBI, toe–brachial index.
Spatiotemporal gait parameters (chronic adaptations)
There was no significant time or time × exercise duration interaction effect on the inter-limb symmetry of the spatiotemporal gait parameters (data not shown), indicating that similar changes were induced by exercise and the intervention in the two lower limbs. Therefore, only the findings of the most symptomatic leg were reported. Stride duration, stride frequency, stride length, and relative duration of the double support phase did not change significantly after SET (Table 3). In contrast, following SET, the duration of the stance phase significantly increased, and the duration of the swing phase significantly decreased (time effect: p = 0.05; Table 3). Moreover, the duration of the loading response and foot-flat phase significantly increased (time effect: p ⩽ 0.03; Table 3), whereas the duration of the push-off phase significantly decreased (time effect: p = 0.002; Table 3).
Spatiotemporal gait parameters in the most symptomatic leg during constant-load treadmill test before and after SET.
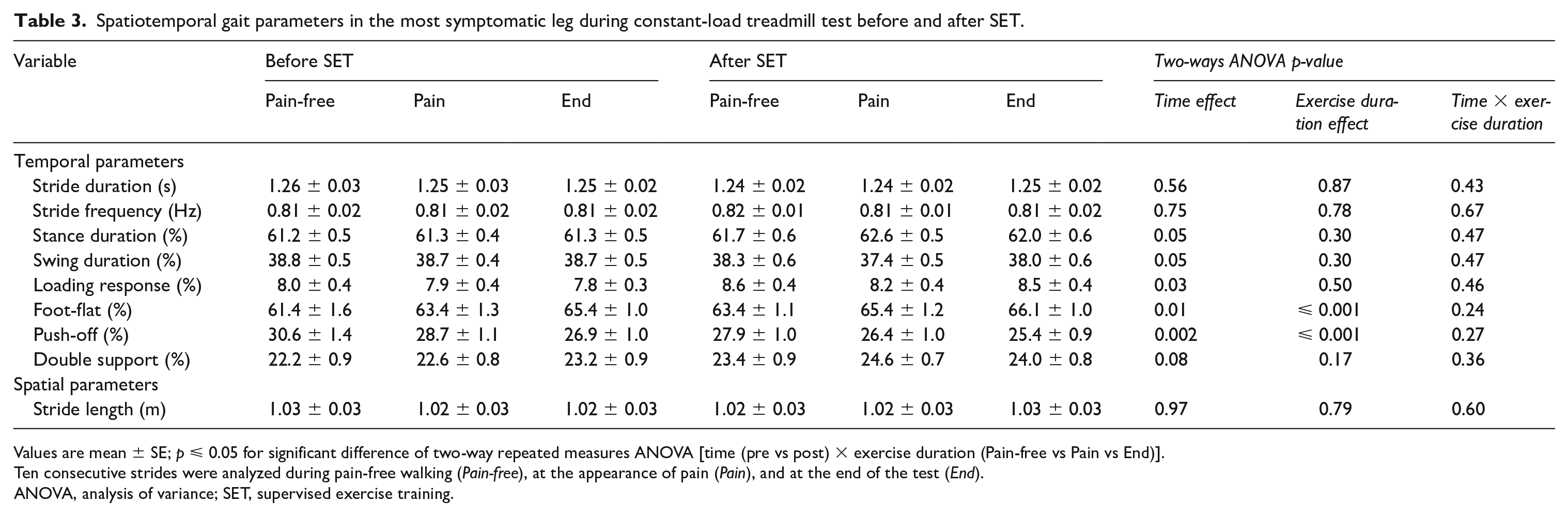
Values are mean ± SE; p ⩽ 0.05 for significant difference of two-way repeated measures ANOVA [time (pre vs post) × exercise duration (Pain-free vs Pain vs End)].
Ten consecutive strides were analyzed during pain-free walking (Pain-free), at the appearance of pain (Pain), and at the end of the test (End).
ANOVA, analysis of variance; SET, supervised exercise training.
Spatiotemporal gait parameters (acute adaptations)
During the treadmill test, the duration of the foot-flat phase and the duration of the push-off phase showed a significant exercise duration effect (p ⩽ 0.001; Table 3). Multiple comparisons showed that the duration of the foot-flat phase significantly increased (Pain-free < Pain < End; p ⩽ 0.02), and the duration of the push-off phase significantly decreased (Pain-free > Pain > End; p ⩽ 0.002). There was no significant time × exercise duration interaction effect (Table 3).
Correlations
There was a significant positive partial correlation between changes in the foot-flat phase and changes in PFWD, whilst controlling for foot-flat phase baseline values (r(24) = 0.43, p = 0.03). There was a significant negative partial correlation between changes in the push-off phase and changes in PFWD, whilst controlling for push-off phase baseline values (r(24) = −0.39, p = 0.05). There was no significant partial correlation between changes in the loading response and changes in PFWD, whilst controlling for the loading response baseline values (r(24) = 0.04, p = 0.86). There were no significant partial correlations between changes in relative durations of the subphases of stance and changes in MWD (p ⩾ 0.23).
Discussion
The results presented herein confirm our hypotheses. First, after 3 months of SET, walking performance was improved (increased PFWD and MWD; chronic adaptations). Second, the changes in the stance phase associated with the onset of claudication (shorter duration of the propulsion phase along with longer duration of the foot-flat phase) followed the same evolution during the MWD treadmill test before and after SET (acute adaptations), but they were delayed after the intervention (increased PFWD; chronic adaptations). Third, 3 months of SET shortened the duration of the push-off phase and lengthened the duration of the foot-flat and loading response phase (chronic adaptations). Additionally, changes in temporal gait parameters during the foot contact phase (foot-flat and push-off) were significantly correlated with changes in PFWD following SET. On the contrary, no significant correlations were found between changes in temporal gait parameters and MWD following SET. These results indicate that changes in temporal gait parameters during the foot contact phase potentially constitute an underlying mechanism of delayed claudication distance in patients with symptomatic PAD.
The results of the present study confirm the beneficial effect of SET on treadmill walking performance in symptomatic patients with PAD.16,18,20 Our multimodal SET includes a combination of two training modalities focused on the main parameters (strength and endurance of the lower limbs) that describe functional decline in patients with PAD. We recently showed that our multimodal SET is effective in improving quality of life, treadmill walking performances, and functional walking (6-minute walking distance) in symptomatic patients with PAD. 26
Controversies exist as to whether gait pattern improve after SET and whether it contributes to an increased exercise tolerance. Previous investigations have shown that SET does not improve the gait profile (kinetic, kinematic, or spatiotemporal gait parameters) in patients with symptomatic PAD.10,22,23,35 On the other hand, it has recently been shown that SET improves muscle strength and modifies hip and ankle kinematics and kinetics in these patients. 24 In addition, recent findings have also demonstrated that SET decreases the range of motion, torque, and work of the hip joint during walking. 36 These adaptations are related to an increased treadmill walking capacity.24,36 The reasons for the discrepancies among studies are difficult to determine, as little is known about the changes in the gait profile following SET and its potential contribution to improved walking performance. The differences may be related to the training modality (multimodal vs treadmill/cycling), duration (3, 6, 12 months), and gait assessment (concomitantly vs separately to a walking test). In the present study, both spatiotemporal gait parameters and walking performance were assessed during the treadmill test. Thus, the potential role of spatiotemporal gait parameters in exercise tolerance after SET, which is known to increase,16,20 could be assessed in patients with PAD. The results presented herein showed that during maximal acute exercise, the duration of the foot-flat phase progressively increased, and the duration of the push-off phase progressively decreased. This finding is in line with those recently observed by Gommans et al. in patients with PAD. 12 It was hypothesized that the longer duration of the foot-flat phase may favor better muscle oxygenation during exercise. 12 Additionally, the lengthened duration of foot-flat may also be an intuitive adaptive walking strategy aiming to increase stability once claudication appears and worsens to a maximal level. On the other hand, although our results are descriptive and cannot elucidate which mechanism occur, the shorter duration of the propulsion phase may be related to the fatigue or inefficiency of ischemic calf muscles. This is in line with recent findings showing that, once claudication is established, plantar flexor muscle strength further decreases compared to a pain-free condition. 4 To note, a similar evolution of temporal gait parameters of the subphases of stance was observed after SET (i.e. similar exercise acute adaptation before and after SET), but with a delayed claudication distance.
The novelty of the present results is that 3 months of SET shortened the duration of the push-off phase and lengthened the duration of the foot-flat and loading response phase. To note, temporal changes in the foot-flat and push-off phases were significantly correlated with changes in PFWD following SET. Despite the descriptive entity of our data, we may suggest that these results are in line with those presented by Schieber et al., 24 who have recently showed that SET improves ankle power generation during the push-off phase in patients with PAD. In this study, 24 plantar flexion angle and torque were unchanged after SET, suggesting that increased ankle power generation during the push-off phase was probably linked to an increased angular speed during plantar flexion. This phenomenon may lead to a decreased propulsion time. 24 These results suggest that, following SET, there is improved participation of the plantar flexors during walking. As recent findings have demonstrated that SET decreases the range of motion, torque, and work of the hip joint during walking, 36 the results of the present study may suggest that there is an improved distribution of the lower limb propulsive forces to walk at the same speed and incline following SET. Improved participation of the plantar flexors, which is associated with a longer duration of the foot-flat phase, may contribute to both a delay in the development of pain and improvements in treadmill performance following SET. First, it might be hypothesized that the longer duration of the foot-flat phase following SET may lead to increased walking stability. Second, the foot-flat phase is a subphase of stance associated with limited lower limb muscle activation. 9 Therefore, as an increase in arterial blood flow into skeletal muscles mainly occurs during the muscle relaxation phase,12,37 patients with PAD may adopt this gait pattern to improve the balance between oxygen delivery and consumption within skeletal muscles during walking exercise. 12 Taken together, these results suggest that changes in temporal gait patterns after SET mainly reside in the reorganization of the durations of the foot subphases of stance.
Limitations
Some methodological limitations need to be addressed. First, in this study, a control group that did not perform SET is lacking. Patients were recruited during routine clinical vascular visits. Therefore, for ethical considerations, all patients who meet the inclusion criteria and are willing to participate in SET must be included in our intervention. Previous studies have demonstrated a lack of clinical and health-related outcomes in control groups of patients with symptomatic PAD.16,18 Specifically regarding gait patterns, to the best of our knowledge, there is only one study that also included an age-matched PAD control group, and that study showed no significant differences between pre- and post-test conditions in spatiotemporal gait parameters. 22 Therefore, we preferred to engage patients in a lifestyle intervention to maximize their benefits. The beneficial effects of SET on spatiotemporal gait parameters need to be confirmed in a randomized control trial including a control group that does not undergo an exercise intervention and different training groups that perform a single training modality (Nordic walking or strengthening of the lower limbs). This would allow determining the relative role of each training modality on gait adaptations following SET and provide guidance for developing new targeted rehabilitation strategies in this population. Second, validation of the Physilogs® has never been investigated in patients with PAD. However, these inertial sensor units were previously validated to assess gait pattern in young 34 and older adults.33,34 In addition, the accuracy and precision were demonstrated to be good with excellent repeatability across measurements. 34 Third, the dose of the exercise intervention (e.g. the number and duration of sessions) may slightly differ between participants, and it is therefore difficult to determine the changes in walking performance and gait adaptations in relation to these differences. Fourth, the speculation that the decreased propulsion time after SET may be related to an increased ankle power generation during walking needs to be further assessed with more detailed analysis of gait (i.e. kinetics and kinematic analysis). Fifth, the speculation that a prolonged duration of the foot-flat phase may allow enhanced blood flow within skeletal muscles following SET also needs to be better assessed in the future.
Conclusion
In conclusion, the results presented herein showed that 3 months of SET shortened the duration of the push-off phase and lengthened the duration of the foot-flat and loading response phase. In addition, changes in foot-flat and push-off phases were significantly correlated with changes in PFWD following SET. These results indicate that changes in temporal gait parameters during the foot contact phase potentially constitute an underlying mechanism of delayed claudication distance in patients with symptomatic PAD.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.