
Abstract

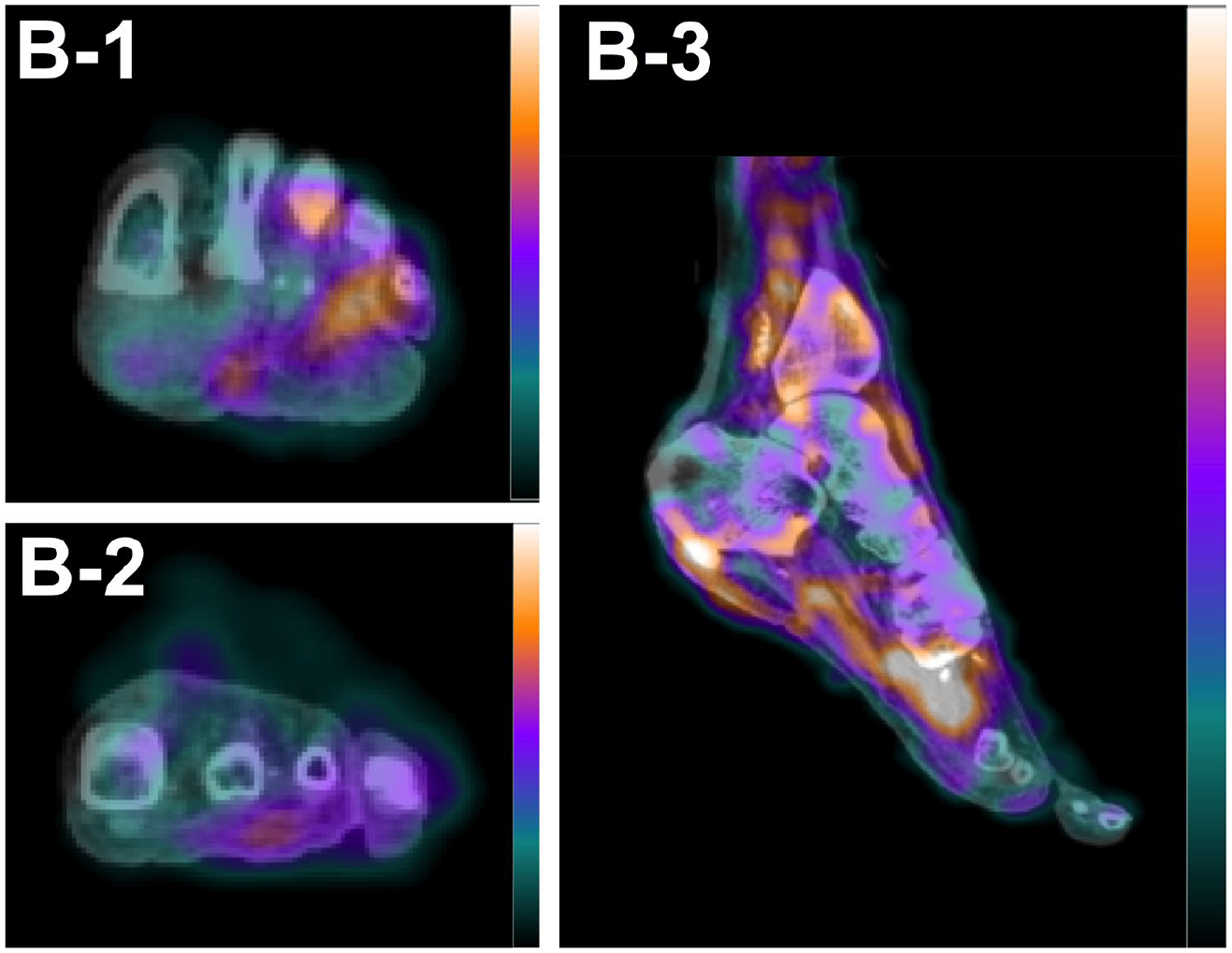
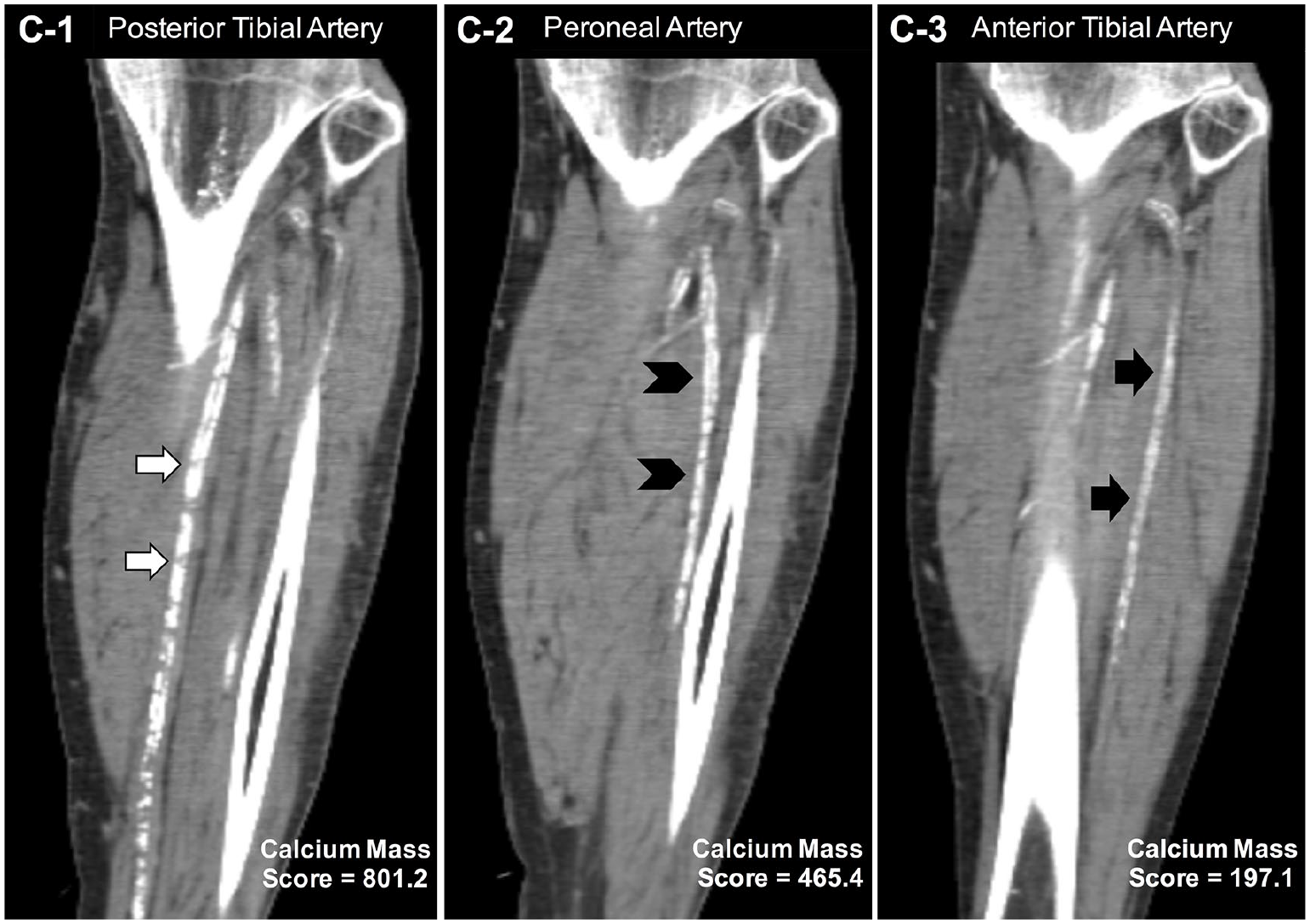
A 60-year-old male presented with critical limb ischemia (CLI), which was associated with second toe gangrene of the left foot (Panel A-1), a left limb ankle–brachial index (ABI) of 0.65, and bilateral claudication. The patient underwent single-photon emission computed tomography/computed tomography (SPECT/CT) imaging with technetium-99m-tetrofosmin to assess foot perfusion as part of an ongoing trial evaluating the utility of radiotracer-based perfusion imaging in patients with peripheral artery disease (PAD). 1 A CT scan was acquired after the SPECT image acquisition for anatomical registration of perfusion imaging, SPECT attenuation correction, and quantification of calcium burden. Co-registered SPECT/CT images revealed a relative perfusion defect that localized to the region of the gangrenous tissue and the great toe (Panels B-1 and B-2) and extended to the head of the metatarsals (Panel B-3). Quantitative analysis of the CT images revealed extensive calcification of the posterior tibial artery (Panel C-1, white arrows) as well as calcification of the peroneal (Panel C-2, black arrowheads) and anterior tibial (Panel C-3, black arrows) arteries, as determined by the calcium mass score. 2 The patient subsequently underwent digital subtraction angiography (DSA) to assess the left limb, which confirmed multivessel disease that consisted of occluded left common femoral (Panel D-1, arrows) and posterior tibial (Panel D-2, arrows) arteries. Endarterectomy of the left external iliac, common femoral, profunda femoris, and superficial femoral arteries was then successfully performed and DSA indicated two-vessel run-off below the knee. Two days post-revascularization, the patient underwent amputation of the necrotic/infected second toe (Panel A-2). One month later, the surrounding tissue demonstrated signs of necrosis, dehiscence, and infection. Therefore, a transmetatarsal amputation (TMA) was performed to the level of active bleeding, which corresponded with the perfusion assessment by SPECT/CT imaging one month earlier (Panel B-3). The amputation site healed over the following 10 months (Panels A-3 – A-5).
Radiotracer-based imaging has recently demonstrated utility for assessing regional abnormalities in microvascular perfusion of the foot and for quantifying perfusion responses to revascularization in patients with CLI.3,4 The current case highlights the potential of hybrid radiotracer-based imaging for providing dual assessment of both microvascular perfusion status and vessel-specific calcium burden in patients with CLI. Additionally, the present case suggests that radiotracer-based imaging of microvascular perfusion may offer insight into tissue viability and thereby assist clinicians with determining the appropriate level of amputation. Collectively, hybrid nuclear imaging techniques could provide novel insight into the interplay between lower extremity calcium burden, tissue perfusion, and risk for amputation.


‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine