
Abstract

We present a patient with a right cervical mass. The importance of this case is that imaging studies suggested a possible paraganglioma, which may have resulted in incorrect treatment.
A 78-year-old man presented with a 3-month history of an asymptomatic right neck mass. He is a mild smoker with chronic obstructive pulmonary disease (COPD). On examination, a solitary, firm, 4-cm mass was palpable on the right side of the neck. No other masses were found. An outside hospital neck duplex ultrasound proposed a diagnosis of a carotid aneurysm with intramural thrombus. Once admitted, computed tomography angiography (CTA) revealed an ovoid (4.4 × 2.1 × 9.3 cm) right carotid space mass, completely surrounding the common, internal, and external carotid arteries (Panel A-1, black arrows), with mild bifurcation splaying (Panel A-2, white arrow) and progressive contrast enhancement. Magnetic resonance imaging (MRI) showed homogeneous intermediate signal intensity, with small hypointense foci suggesting a possible ‘salt-and-pepper’ appearance on T2-weighted images (Panel B-1, white arrows). MRI confirmed the hypercellular (Panel B-2, black arrows) and hypovascular nature of the lesion (Panel B-3, white arrows). Finally, an 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) showed a hypermetabolic solitary mass with moderate glucose uptake (SUVmax of 5.1) (Panel C-1, black arrows). MRI and PET/CT reports included a paraganglioma as a strong consideration in the differential diagnosis.


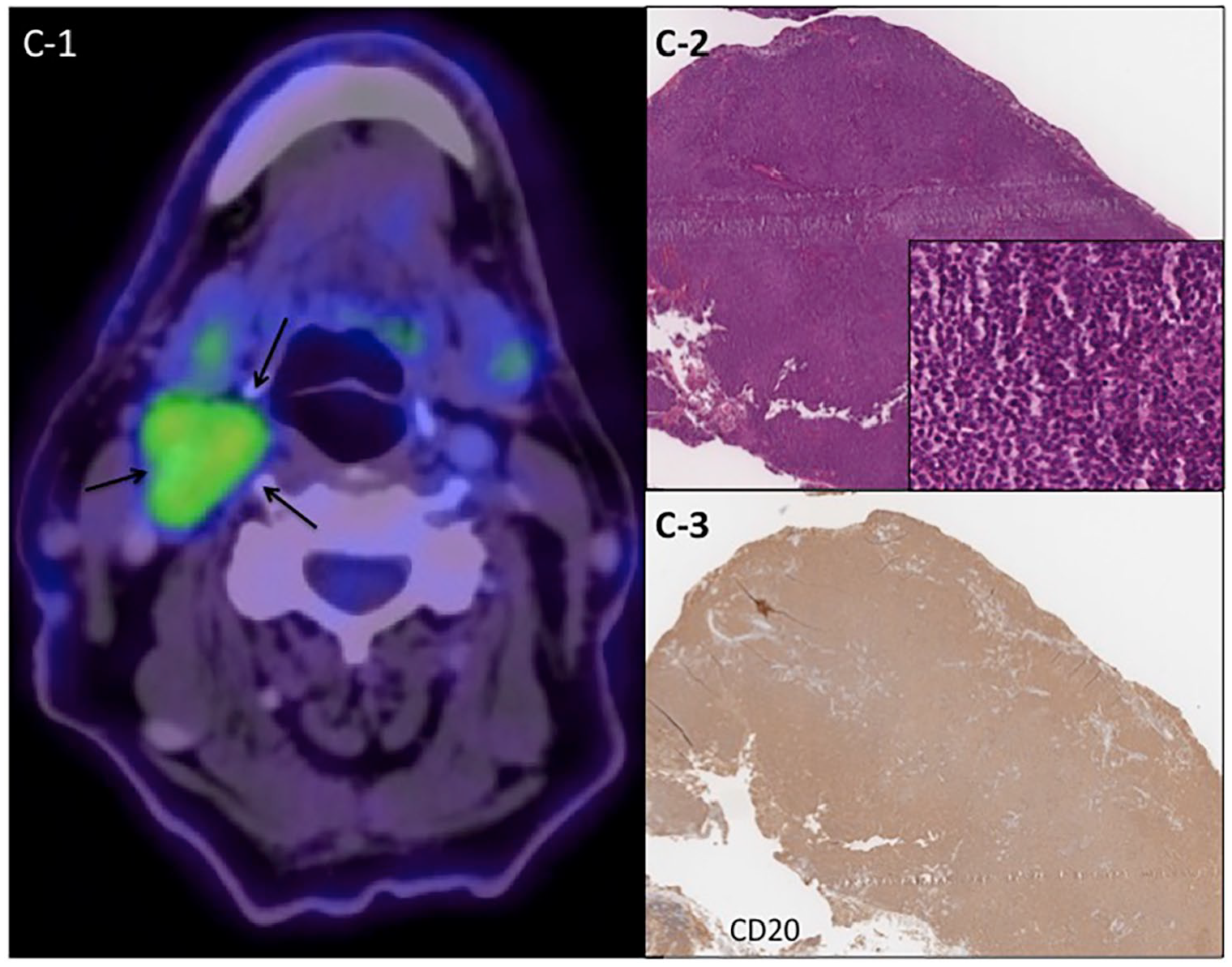
An incisional biopsy was planned. At surgery, a soft, dark purple mass wrapping the bifurcation and carotid arteries filled the entire surgical field. A 2 × 1-cm tumor sample was obtained without incident. The patient was discharged on POD 3. Histological examination showed complete effacement of the lymph node architecture by a lymphoid neoplasm composed of small-to-medium-sized cells with monocytoid features (Panel C-2 inset) with strong positivity for the B-cell marker CD20 (Panel C-3), consistent with the diagnosis of low-grade marginal zone B-cell non-Hodgkin’s lymphoma. He received chemotherapy and is alive 13 months after the biopsy.
Neck paragangliomas are usually highly vascular lesions, although avascular lesions may be seen. Treatment is surgical excision, but neurovascular complications, including stroke, are more frequent in large, Shamblin III tumors. 1 This patient’s lesion could have been classified as a Shamblin III tumor and exeresis could potentially have had significant morbidity.
Based in our experience with carotid paragangliomas, 2 careful analysis of the imaging studies performed identified elements that in the present case were not typical for a paraganglioma: poor irrigation of the mass, overall homogeneous signal, large longitudinal extension, complete encirclement of the carotid space vessels, and only mild separation of the internal and external carotid arteries. PET/CT was performed to evaluate lesion metabolism and look for other masses. Reported high uptake in some paragangliomas did not allow confident differentiation from lymphoma. 3 Owing to the lack of a clear diagnosis and the possible risks of fine-needle aspiration cytology, an incisional biopsy allowed the correct diagnosis, avoiding unnecessary major surgery.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor-in-Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article from the Department of Vascular and Endovascular Surgery of the Pontificia Universidad Católica de Chile.