
Abstract

What is venous reflux?
The veins are the blood vessels that return blood to the heart. Veins have valves that are small flaps of tissue that help the blood travel back toward the heart against gravity. As blood flows toward the heart, the valves are open. As blood starts to fall backward with the effect of gravity, the valves close. Venous reflux happens when the valves are damaged or not working properly and let blood go in the wrong direction within the vein. When this happens, blood pools toward the feet, causing veins to bulge or become twisted, also known as varicose veins. This prolonged pooling of blood toward the feet can lead to leg symptoms. A venous reflux study, sometimes referred to as a ‘venous insufficiency study’ or ‘venous incompetence study’, is a noninvasive ultrasound-based test to look at the valves in the veins and determine if they are functioning normally.
What causes venous reflux?
In many cases, venous reflux is thought to result from weakness in the vein wall that leads to enlargement of the area of the vein where the valves are attached. In some patients, venous reflux develops after a prior blood clot, which can scar the vein and damage the valves.
Venous reflux is widespread and is more likely as people get older. Although both men and women can have venous reflux, it is more common in women. Pregnancy can play a role, with many women developing leg symptoms or varicose veins during pregnancy. Heredity plays a strong role in the development of venous reflux, especially if both parents have varicose veins. Obesity also increases the risk of developing venous reflux.
What are the symptoms of venous reflux?
Venous reflux can cause leg symptoms, often known as venous insufficiency. These symptoms include swelling, heaviness, aching, and itching. 1 Some patients have chronic skin changes such as redness, darkening, thinning, and dryness, and they may have poor wound healing. In severe cases, some patients may develop sores, often at the ankle or the lower part of the leg, called ulcers. Ulcers may develop after minimal trauma such as bumping the shin, but ulcers may also form spontaneously, with no trauma.
Why and how is venous reflux testing performed?
Oftentimes, the physical changes and symptoms caused by reflux are diagnosed on the basis of careful history taking and physical examination alone, and treatment such as compression stockings is started without further testing. In patients whose symptoms do not improve with initial treatment, venous reflux testing may be performed to help make the diagnosis or to help plan for a procedure to eliminate varicose veins.
A venous reflux study is a noninvasive ultrasound examination. 2 This test is performed in a vascular lab by a sonographer (also called a vascular ultrasound technologist). The test usually takes between 1 and 2 hours, depending on whether one or both legs are examined. It is important that the patient undergoing the test is well hydrated, has not skipped meals, and has not worn compression stockings, compression bandages, or other compression garments in the 24 hours before the test. There is no need to fast beforehand, and medications can be taken as usual prior to the test.
On arrival to the testing area, the patient will be asked to change into a gown or disposable shorts because the sonographer will look at the veins all the way up to the groin. The sonographer places warm gel on the patient’s leg and uses a transducer—a handheld probe attached to the ultrasound machine—to obtain images. Ultrasound translates high-frequency sound waves (higher than those the human ear can hear) into pictures of the patient’s blood vessels. There is no contrast dye used and no exposure to radiation during an ultrasound test.
First, the sonographer looks for any old or new blood clots in the veins. During this portion of the test, the sonographer uses the transducer to press on the deep and surface (superficial) veins in the thigh and calf. Veins that are free from blood clots collapse completely with pressure from the transducer. If the sonographer finds a new blood clot, the test may be stopped and the patient’s physician notified.
After checking for blood clots, the sonographer uses multiple, recurring, short compressions to determine if the valves let blood go in the wrong direction within the vein (i.e., venous reflux) (Figure 1). The sonographer can generate these compressions by squeezing the leg with the hands, or the sonographer may use an automatic blood pressure cuff that inflates and deflates rapidly to generate the compressions. For the reflux part of the test, the patient is asked to stand, shifting all his or her weight onto the opposite leg so the muscles in the leg being examined can be fully relaxed (Figure 2A). The standing position is important because pooling is the greatest and the valves are the most challenged when standing. If the patient is unable to stand, the bed or cart may be tilted so the legs are as low as possible compared to the heart (Figure 2B). Patients who feel uncomfortable standing for long periods or who become dizzy during the test should inform the sonographer. If the patient is not standing or in a position with the legs well below the level of the heart, the study may be falsely negative (i.e., normal).
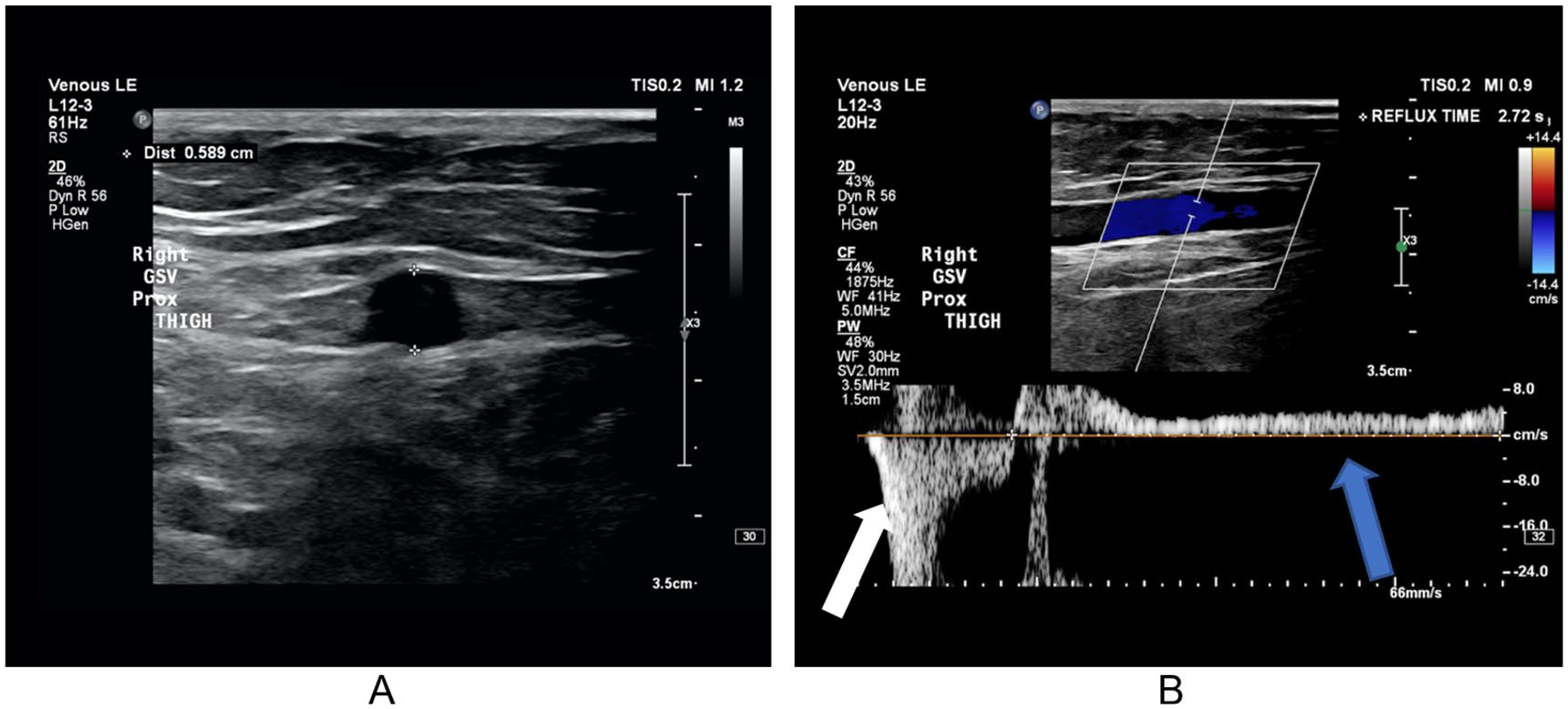
(A) Image of a superficial vein using ultrasound. The size of the vein is measured to determine if it is enlarged (i.e., a varicose vein). (B) Doppler image of the blood flow within the vein, going in the wrong direction (reflux). The sonographer measures the length of time the blood goes the wrong way (gray/blue arrow) after a compression maneuver (squeezing of the calf; white arrow). There is a minimum length of time to be considered abnormal. Shown here is significant reflux lasting 2.7 seconds. GSV, great saphenous vein.
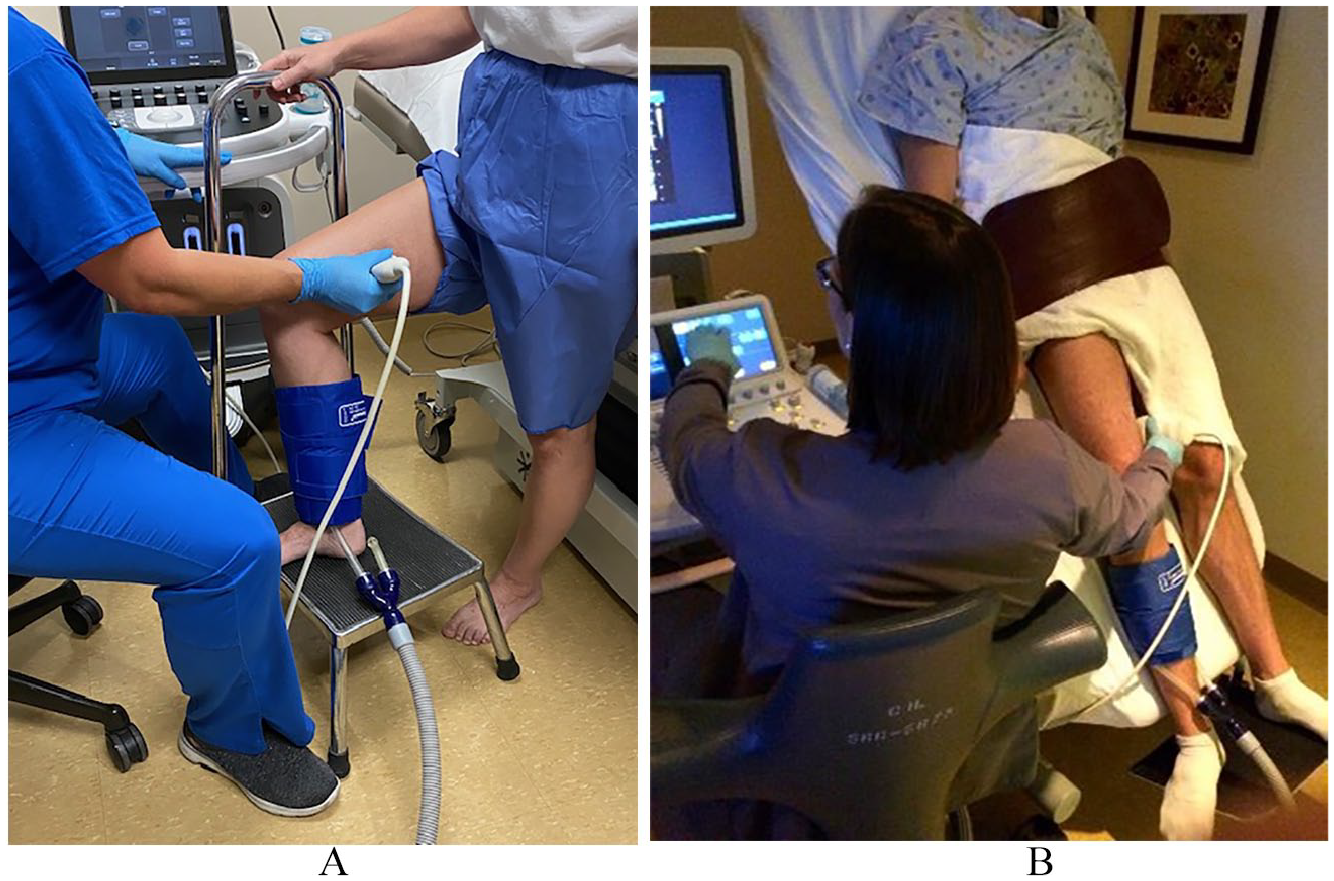
(A) Patient in the optimal standing position for a reflux study with weight on the left leg and the right leg relaxed. (B) An alternative position on a tilted table. The patient is still placing all weight on the leg not being scanned.
If abnormal veins are identified, the sonographer obtains measurements of their diameter and depth, which can aid in planning possible procedures.
During the test, a number of sounds can be heard, which may sound like a heartbeat and a whooshing sound as the blood moves through the veins.
How is venous reflux defined?
During a venous reflux test, reflux time is measured. Normal valves in the veins allow a small amount of blood to flow backward. In general, reflux in a normal vein should last less than half a second. Reflux may be noted in the deep veins or the superficial veins.
What will the test results show, and how is that information used?
The test may be normal, which can be helpful in determining that vein reflux is not the reason for the patient’s symptoms and guide the physician toward another cause for the patient’s leg complaints. Occasionally the test will show a blood clot in the deep or surface veins. If there is a clot in the deep veins, the patient usually will be treated with a blood thinner (anticoagulant) medication.
During the test, the sonographer will record which veins are affected and the reflux times and size of the affected veins, and a physician trained in interpretation of ultrasound will finalize a report. This information can help determine if a procedure to seal off or eliminate the refluxing veins should be recommended. It can also help determine which procedure might be best.
Conclusion
In summary, a venous reflux study is an ultrasound examination of the leg veins that determines if blood is returning to the heart normally. The results of this test provide a map of healthy and unhealthy veins that can then be used by a vascular specialist to determine whether a patient would benefit from a particular treatment for varicose veins and reflux, or if the veins in the legs may not be the cause of a patient’s symptoms.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage.
The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.