
Abstract

Ulnar artery thrombosis is a rare condition which can occur in hypothenar hammer syndrome (HHS), in which acute or repetitive blunt trauma to the ulnar artery causes local occlusion and thrombosis. 1 It typically presents unilaterally in the dominant hand and there have been no reported cases of HHS from yoga. We describe a rare case of bilateral ulnar artery thrombosis in a patient with multiple thrombophilia risk factors after performing the downward dog yoga maneuver in which both hands are extended with weight applied through the wrists (Panel A).
A 47-year-old female developed bilateral wrist pain while performing the downward dog yoga maneuver. She then noted progressive swelling and tenderness over the ulnar aspect of both wrists and symmetrically cool fingertips and thumb. She was otherwise a healthy non-smoker on the combined oral contraceptive pill (OCP) only. Her mother had recurrent deep vein thrombosis with a positive prothrombin gene mutation and elevated lipoprotein(a).
On examination, the patient had bilateral positive Allen’s tests with swelling and tenderness over both distal ulnar arteries. A left hand Allen’s test showed pallor due to the absence of ulnar artery filling of the palmar arch (Panel B). Her body mass index was 42 and her cardiac, peripheral vascular, rheumatological and hematological system examinations were normal.

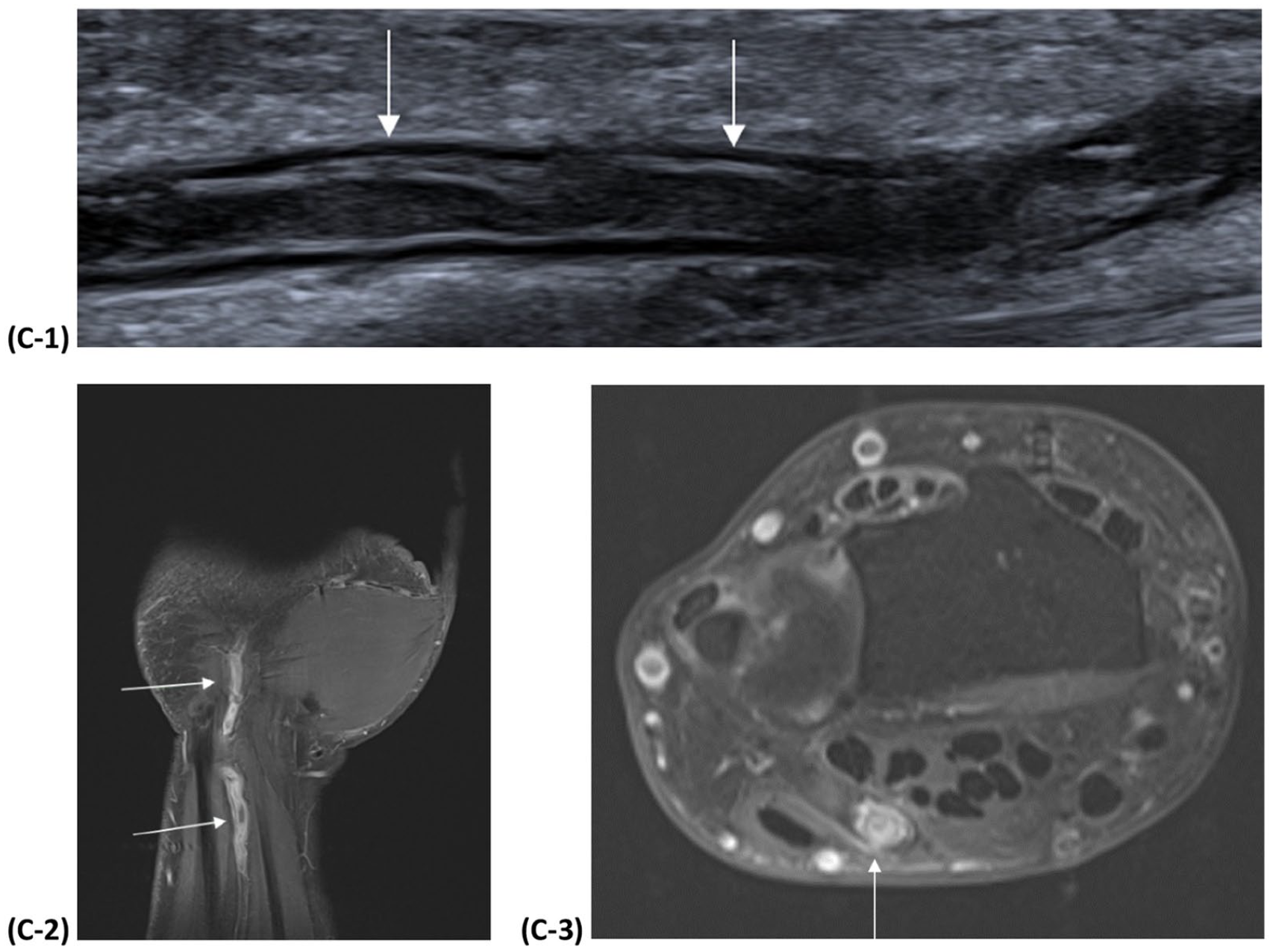
Duplex ultrasound demonstrated bilateral ulnar artery thrombosis measuring 4 cm in length, extending proximally from the level of the wrist (Panel C1: arrows). Magnetic resonance imaging (MRI) of her more symptomatic left wrist confirmed a long-segment thrombosis with no external compression of the ulnar artery (Panels C2, C3: arrows highlight thrombosis). A transthoracic echocardiogram, Holter monitor, and duplex ultrasound of the supra-aortic and upper limb arteries were normal.
Laboratory studies were significant for a positive lupus anticoagulant (LAC), which was confirmed on repeat testing at 12 weeks. Her lipoprotein(a) was elevated at 1500 mg/L. Inflammatory markers, full blood count, autoimmune serology including antinuclear antibody, antineutrophil cytoplasmic antibody, anticardiolipin and beta-2-glycoprotein antibodies were normal. Tests for heritable thrombophilia tests were negative.
She commenced warfarin with enoxaparin bridging and discontinued the OCP. Symptoms resolved at 3-month follow-up, but the Allen’s test remained positive and residual occlusive thrombus was confirmed on repeat imaging.
We describe a rare case of bilateral ulnar artery thrombosis triggered by anatomical occlusion on wrist extension during the downward dog maneuver in a patient with a strong thrombotic tendency. Treatment was commenced with warfarin given superior efficacy over direct oral anticoagulants in antiphospholipid syndrome.2,3
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.