
Abstract

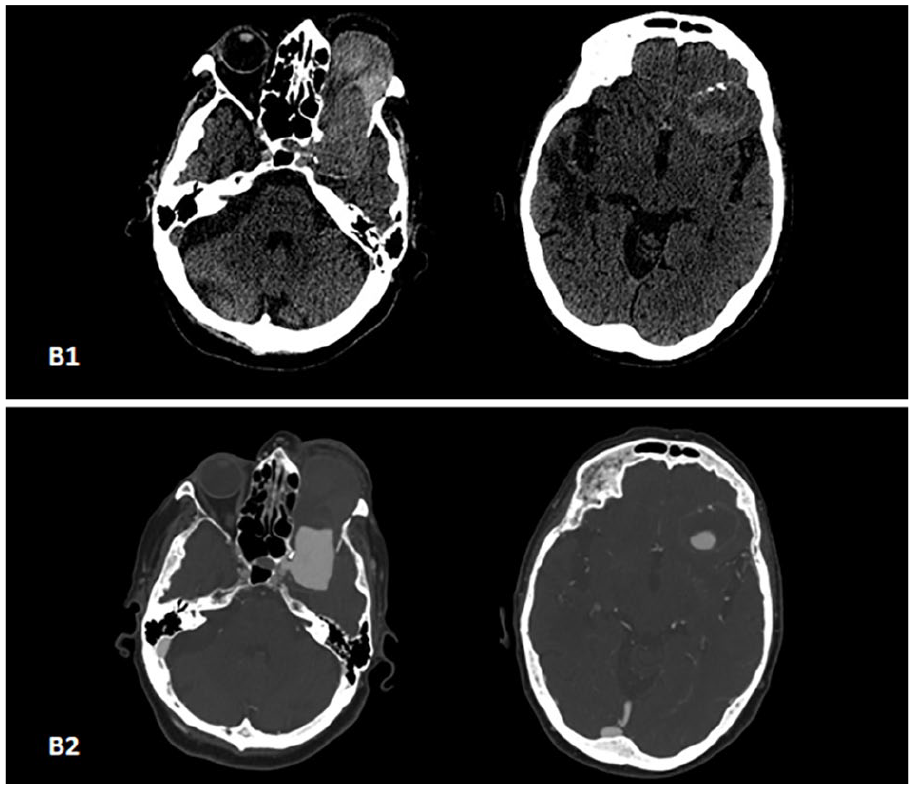
An 86-year-old female was admitted to our department for upper left lobe pneumonia. She had a history of carotid-ophthalmic artery aneurysm, which caused chronic headache, proptosis, and visual loss in the left eye (Panel A). The woman underwent a contrast-enhanced computerized tomography (CT) of the brain. A basal CT scan (Panel B1) showed a left voluminous carotid-ophthalmic fusiform aneurysm in the retro-suprabulbar area and the temporo-frontal lobe. It distorted the intraconal space and caused bone erosion of the orbital foramen and the lesser wing of the sphenoid. The mass had heterogeneous density with a mixed hypo- and hyper-dense pattern due to blood clot and fresh blood, respectively. At the aneurysm’s wall, focal hyperdensities indicated partial calcification. The basal CT image illustrated ischemic brain injury in the right temporoparietal lobe with a consensual widening of the Sylvian cistern, homolateral third ventricle, and cerebral aqueduct. At the post-contrast CT scan (Panel B2), the aneurysm sac showed a homogenous and intense enhancement of the wide residual lumen; the aneurysm neck was detectable in the carotid siphon tract.

In post-contrast sagittal reconstruction (Panel C), the aneurysm measured 7.2 × 3.2 × 3 cm, and the anteroposterior diameter of the residual lumen was 3.3 cm; the ophthalmic artery was not detectable. The lesion caused a mass effect over the eyeball that appeared compressed, deformed, and projected 2 cm beyond the orbital plane. The presence of hyperdensity in maxillary, frontal, and ethmoidal sinus due to mucus retention was likely caused by obstruction of the sinuses.

The lesion arose from the sidewall of the internal carotid artery, and the aneurysmal neck was 5.6 mm in post-contrast coronal reconstruction (Panel D1). The left middle cerebral artery was less opaque than the contralateral due to a steal effect. Tract A1 of the left anterior cerebral artery was not detectable (arrow, Panel D2).

Giant aneurysms are defined by a diameter of 25 mm or above and occur in female patients with higher frequency. 1 The patient usually complains of visual loss and nerve palsies due to mass effect; hemorrhagic presentation is rare. 2 The treatment strategy is still controversial and includes direct aneurysm clipping, ophthalmic artery closure, and conservative treatment. 2 Here, we describe an unusual case of an unruptured giant carotid-ophthalmic aneurysm, one of the largest reported in the literature. Owing to clinical status, age, and the aneurysm’s features, we chose to observe the patient as she was not suitable for any surgical or endovascular intervention.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.