
Abstract

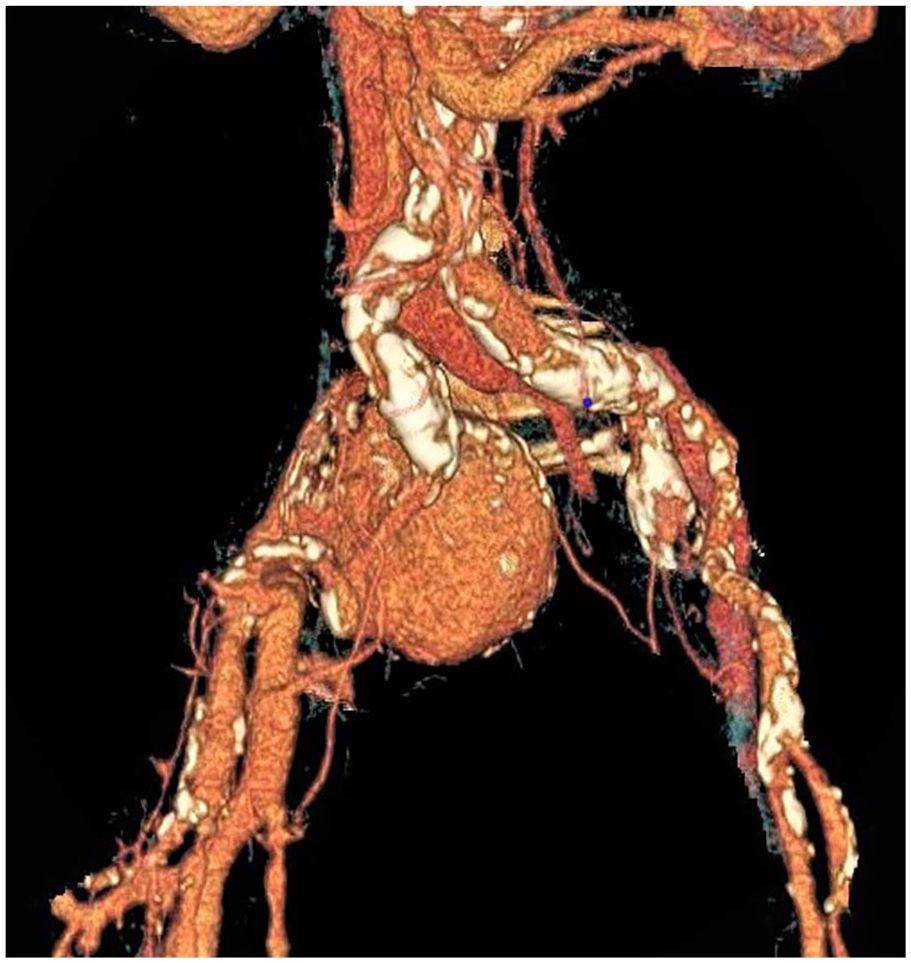
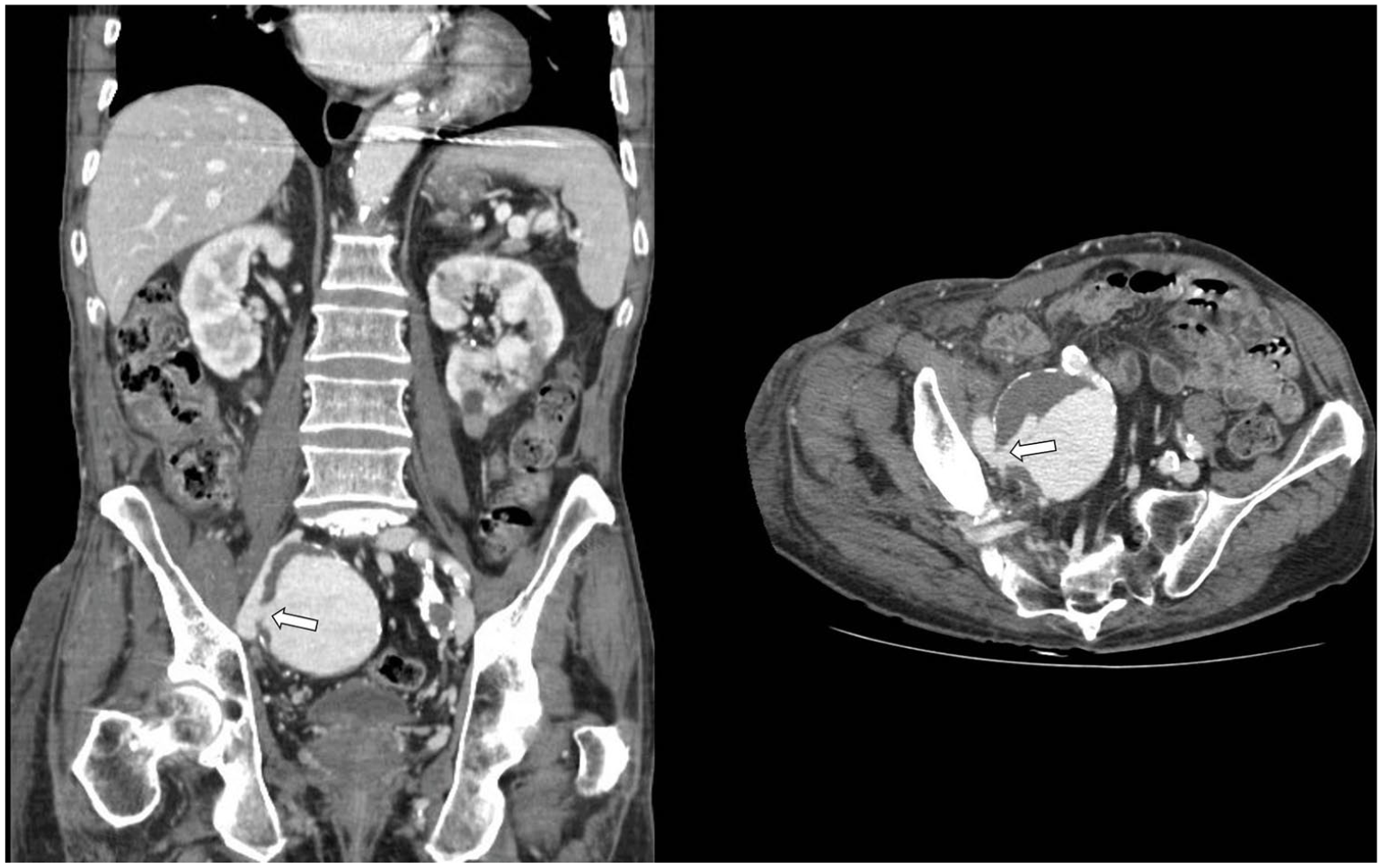
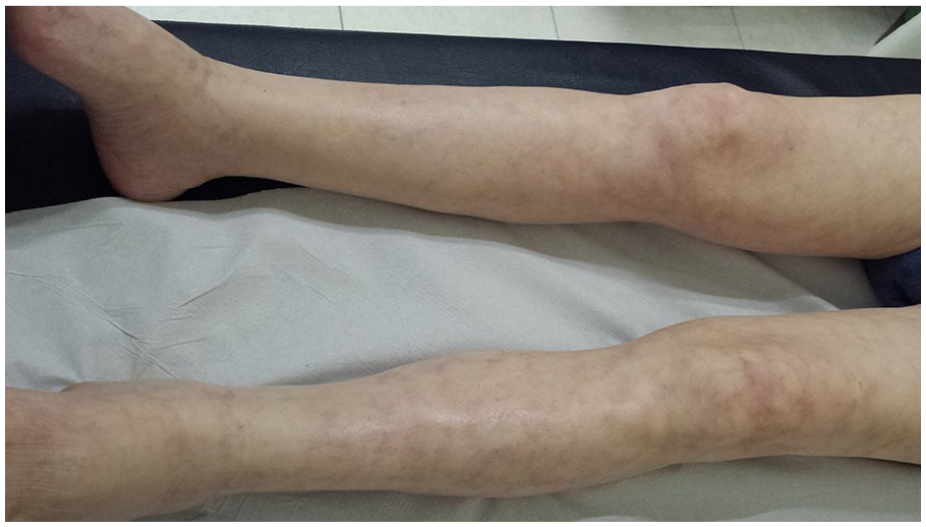
A 74-year-old Caucasian male presented at the emergency departament with swelling and pain of the entire right leg. Laboratory evaluation was notable only for a D-dimer level of 2433 ng/mL (normal range: 0–500 ng/mL). Venous duplex ultrasound revealed echogenic material, loss of compressibility and continuous Doppler signal in the femoro-popliteal veins consistent with acute deep vein thrombosis (DVT). He was started on low molecular weight heparin and referred to the internal medicine clinic for follow up 12 days later. On follow up exam he was noted to have livido reticularis and swelling of the entire right leg, including the inguinal and buttock area; no abdominal mass or pulsatile lesions were detected (Panel A). Computed tomography angiography was performed, which revealed a 7 cm saccular aneurysm of the right internal iliac artery (Panels B and C) that was in communication with the ipsilateral external iliac vein (arteriovenous fistula; arrow in Panel C). No proximal DVT was detected. The patient underwent aneurysm repair via endovascular approach with attempted coiling of the internal iliac artery aneurysm, which was unsuccessful and required open repair with aneurysmectomy via transperitoneal approach. Significant bleeding occurred through the arteriovenous fistula that was sutured, and a venous stent was placed in the external iliac vein. The patient was treated with low molecular weight heparin followed by warfarin. At follow-up, on postoperative day 50, the swelling of the right leg was completely resolved (Panel D).

DVT of the lower extremities is commonly seen in practice, and incidence increases with advancing age. Potentially modifiable risk factors must be considered, including intra-abdominal pathologies leading to venous outflow obstruction like May–Thurner anatomy. 1 The presence of an isolated internal iliac artery aneurysm has been described as an infrequent cause of DVT, and the association with concomitant arteriovenous fistula is similarly rarely reported.2,3 The etiology of the fistula and aneurysm in this case is unknown. Common considerations include a history of trauma, prior abdominal/pelvic surgery or endovascular procedures, infection (mycotic aneurysm), and inflammatory vasculitis. Rarely, ruptured atherosclerotic aneurysms causing arteriovenous fistula may occur.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.