
Abstract

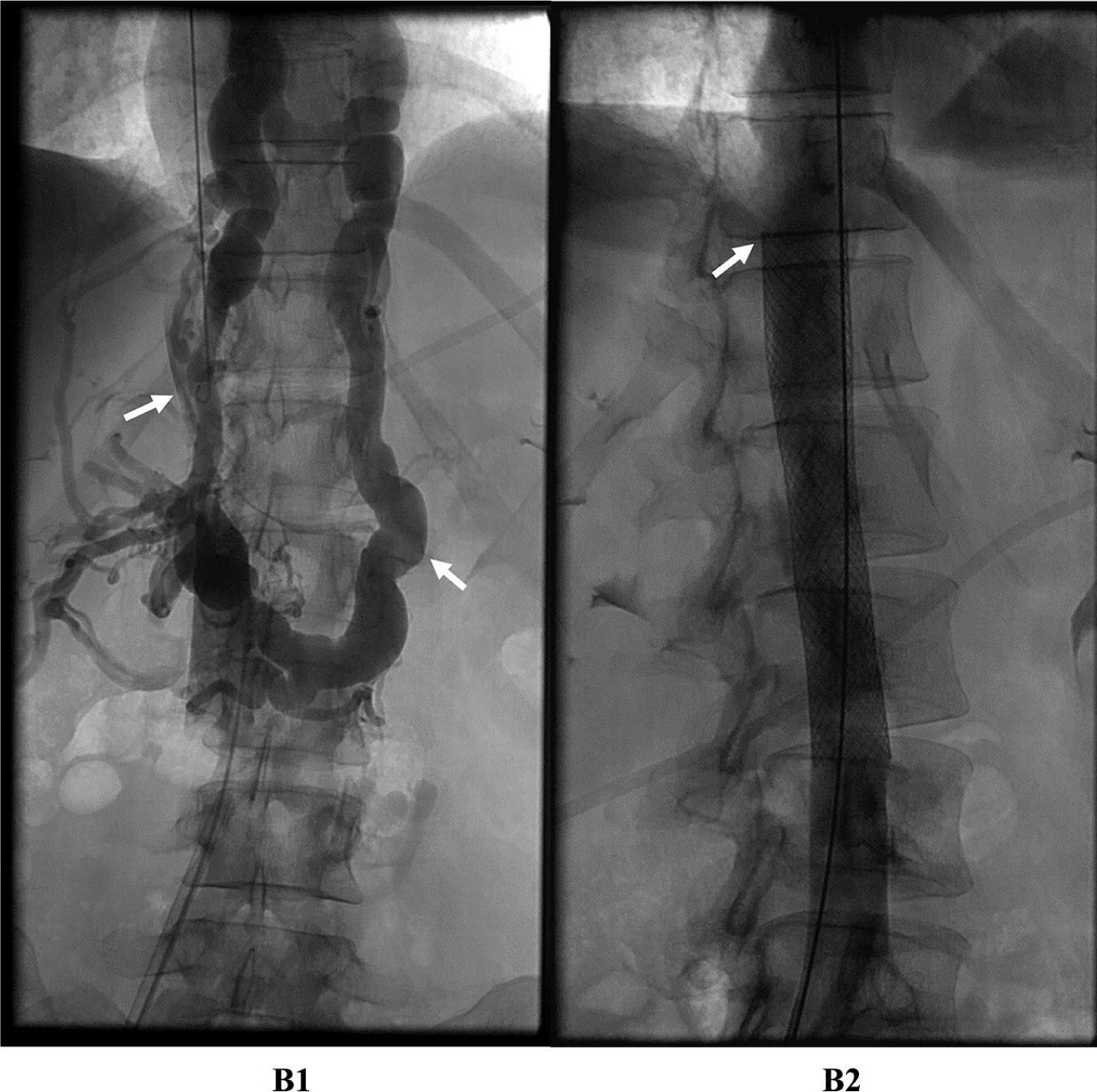
A 37-year-old woman with stage IV retroperitoneal leiomyosarcoma status post-chemotherapy and radiation presented with severe lower extremity edema that was refractory to diuretic therapy. Magnetic resonance imaging (MRI) revealed tumoral encasement of the inferior vena cava (IVC), aorta, celiac trunk, superior mesenteric artery (SMA), bilateral renal veins, and right renal artery (Panel A2, arrowheads). There was a 2 cm segment of thrombosed suprarenal IVC (Panel A1 and A2, arrow) with extensive collateralization via azygos (Panel A1, arrowhead) and lumbar veins. An inferior cavogram demonstrated severe stenosis of juxtarenal IVC with marked collateral flow through the azygos and hemiazygos systems (Panel B1, arrows). A 22 × 70 mm Wallstent (Boston Scientific, Malborough, MA, USA) was deployed just inferior to the cavoatrial junction (Panel B2, arrow). A final cavogram demonstrated good flow through the IVC and cessation of preferential flow through azygos and hemiazygos systems.

Sixteen months later, the patient presented with severe worsening of abdominal pain, increasing lower extremity edema, and sudden onset abdominal distention. MRI demonstrated encasement of the main portal vein with severe stenosis and large volume ascites. An inferior vena cavogram demonstrated severe in-stent thrombosis, which was successfully relined with a Venovo stent (Bard, New Providence, NJ, USA). Transjugular portography demonstrated high-grade stenosis of the portal vein, which was successfully stented with Protégé stents (Medtronic, Dublin, Ireland) (Panel C1 and C2, arrows). Finally, an aortogram demonstrated high-grade stenosis of the mid-right renal artery, which was successfully stented with Herculink stents (Abbott, Chicago, IL, USA) (Panel D).


Central venous obstruction in the setting of malignancy can be caused by a hypercoagulable state, extrinsic compression by tumor, or by direct invasion of vasculature, and can be associated with significant morbidity and mortality. Patients may present with a broad spectrum of symptoms, ranging from asymptomatic to severe, which typically correlates with the chronicity of the occlusion. 1 IVC occlusion classically presents with severe, debilitating lower extremity edema refractory to diuretic therapy with superimposed abdominopelvic symptoms such as pelvic pain, scrotal edema, ascites, renal insufficiency, and hematuria depending on the level of occlusion. 1 Patients with malignant vascular occlusion have such advanced disease that treatment is typically aimed at palliation; thus, endovascular therapies are their only options given the grave morbidity and mortality associated with open surgical reconstruction. 2 Data on endovascular management of IVC occlusions in the setting of malignancy are extremely limited; however, Razavi et al. demonstrated primary and secondary patency of 80% and 97%, respectively. 2
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.