
Abstract

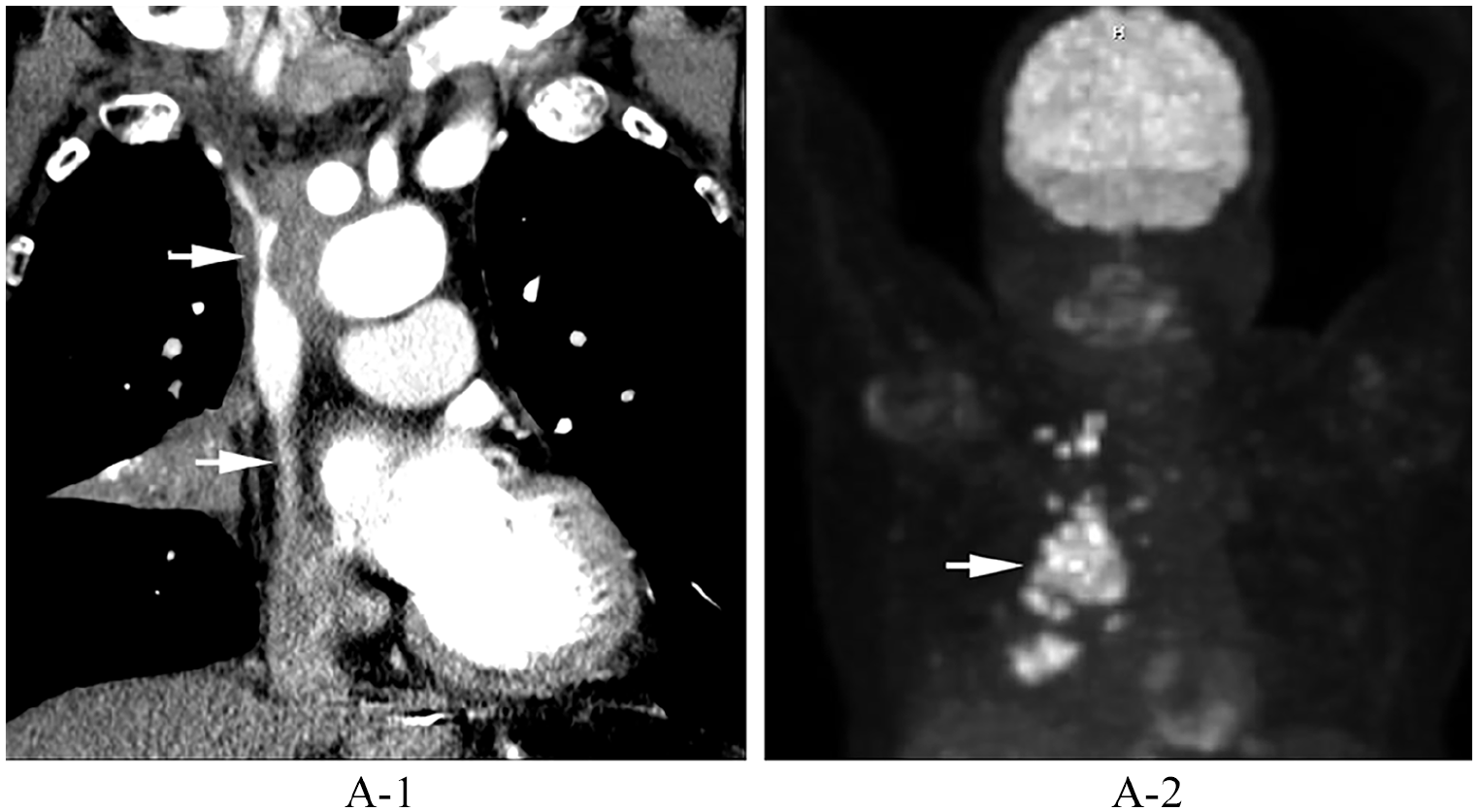
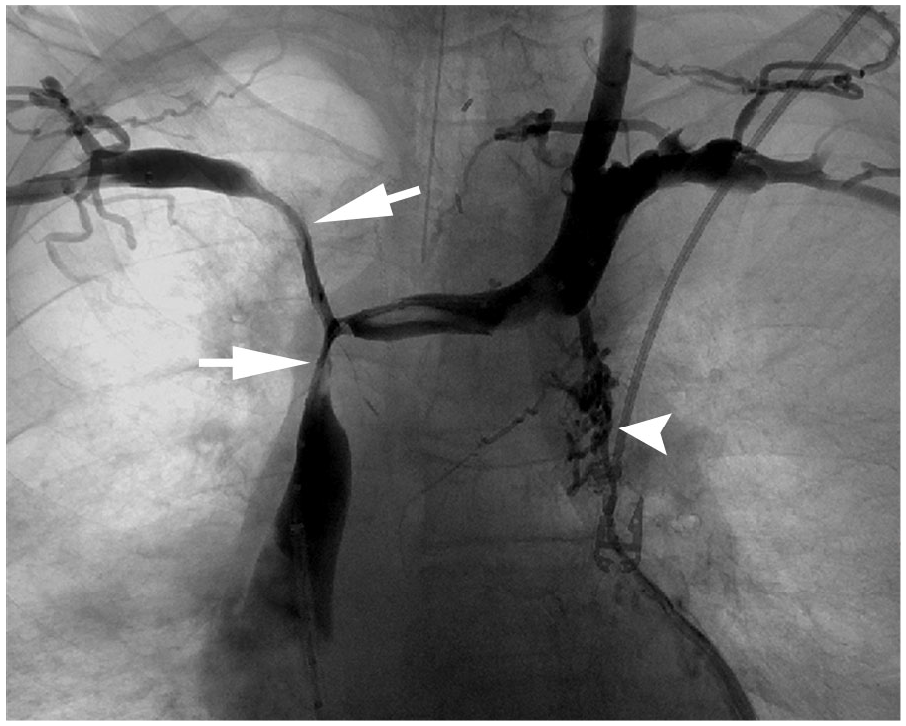
An 80-year-old man with non-small cell lung cancer presented with worsening facial swelling, dizziness, and stridor. A contrasted computed tomography (CT) scan of the chest demonstrated a large lung mass compressing the superior vena cava (SVC) and central bilateral brachiocephalic veins (Panel A-1: arrows). Fluorine-18-fluorodeoxyglucose positron emission tomography (PET) confirmed a massive lung malignancy (Panel A-2: arrow) with distal metastases. Owing to the acuity of symptoms, he underwent diagnostic venography, which revealed flow-limiting stenosis near the confluence of the brachiocephalic veins and SVC (Panel B: arrows). Additional tortuous collateral veins were seen arising from the brachiocephalic veins just peripheral to the stenoses (Panel B: arrowhead). Venous recanalization with balloon angioplasty was performed along the stenotic regions followed by placement of bilateral kissing stents extending from the SVC into each brachiocephalic vein (Panel C). Completion venography confirmed recanalization (Panel D). The patient’s symptoms improved within 24 hours.


SVC syndrome is characterized by facial and upper extremity swelling, headache, dyspnea, and in severe cases, cerebral and laryngeal edema. Malignancy, most commonly lung cancer and lymphoma, accounts for 70% of cases by either external compression or direct tumor invasion. 1 Arterial enhancement of SVC thrombus on contrast-enhanced CT is highly suggestive of direct tumor invasion rather than bland thrombus. 2 Malignancy-associated SVC occlusion typically develops over a period of time and allows for the body to initially compensate with the formation of collateral venous return that can be seen on CT and venography. Symptoms develop when the inflow stenosis reaches a critical point where collateral vessels cannot sufficiently compensate for the obstruction or thrombose. Conventional treatment for SVC syndrome includes chemotherapy and radiation, but these modalities may not provide immediate symptomatic relief or treatment of life-threatening manifestations such as stridor. 1
Endovascular stenting successfully treats obstruction and results in symptom relief within 5 days in up to 93% of patients. 3 Short segment disease can be treated with SVC stenting alone, whereas bilateral brachiocephalic occlusion can be sufficiently treated with either unilateral SVC to brachiocephalic stenting or bilateral kissing brachiocephalic vein stents.1,3 Rare but serious complications include stent migration or caval rupture resulting in tamponade. 1 Stent restenosis is a more common delayed complication due to tumor progression and can usually be treated with repeat angioplasty and stenting. 3 Reopacification of collateral vessels is an early CT finding of subclinical stent restenosis. 2 Although there is no improvement in mortality, endovascular stenting significantly improves morbidity in advanced-stage thoracic cancer.1,2
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.