
Abstract

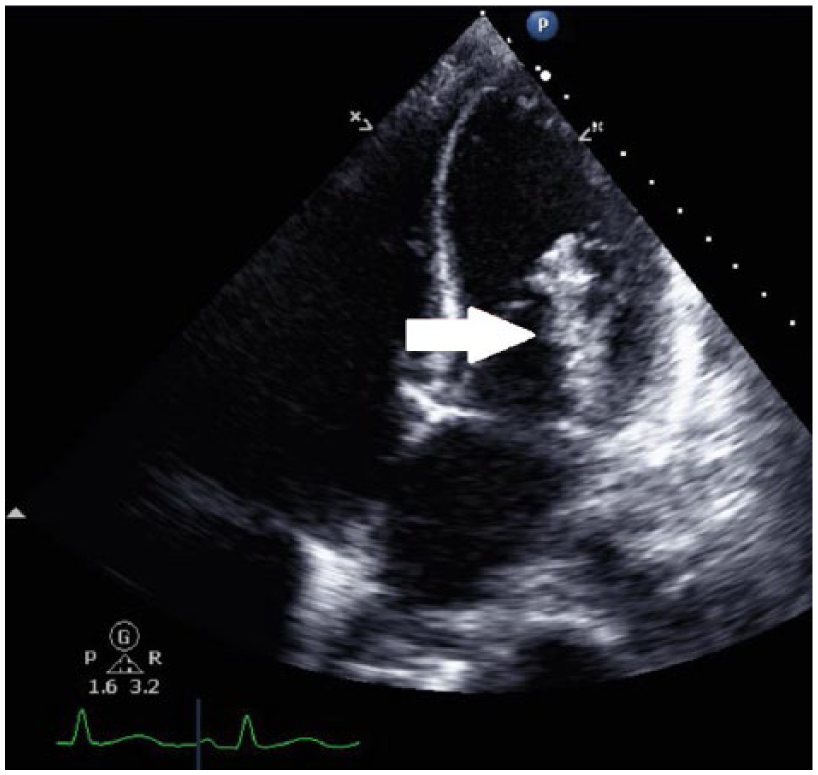
A 24-year-old female was transferred to our facility with a 3-month history of bilateral lower extremity hemiparesis, loss of bowel and bladder control, decubitus ulcers, unexplained weight loss, and fever of unknown origin. Upon arrival, she appeared emaciated with significant dysarthria and a fever of 102°F (38.9°C). She was unable to move her lower extremities on command. Magnetic resonance imaging revealed numerous infarcts in the brain and abdomen. An echocardiogram ordered to assess for the source of emboli revealed a 4.5-cm-long mitral valve vegetation along with severe mitral regurgitation (Panel A: arrow). Mitral valve tissue analysis revealed the bacteria Streptobacillus moniliformis, the causative agent for rat bite fever. 1 The bacteria is acquired from bites, scratches, consuming contaminated food, or by handling infected rodents. Symptoms include fever, rigors, migratory polyarthralgias, headache, nausea, vomiting, sore throat, and severe myalgias. 2
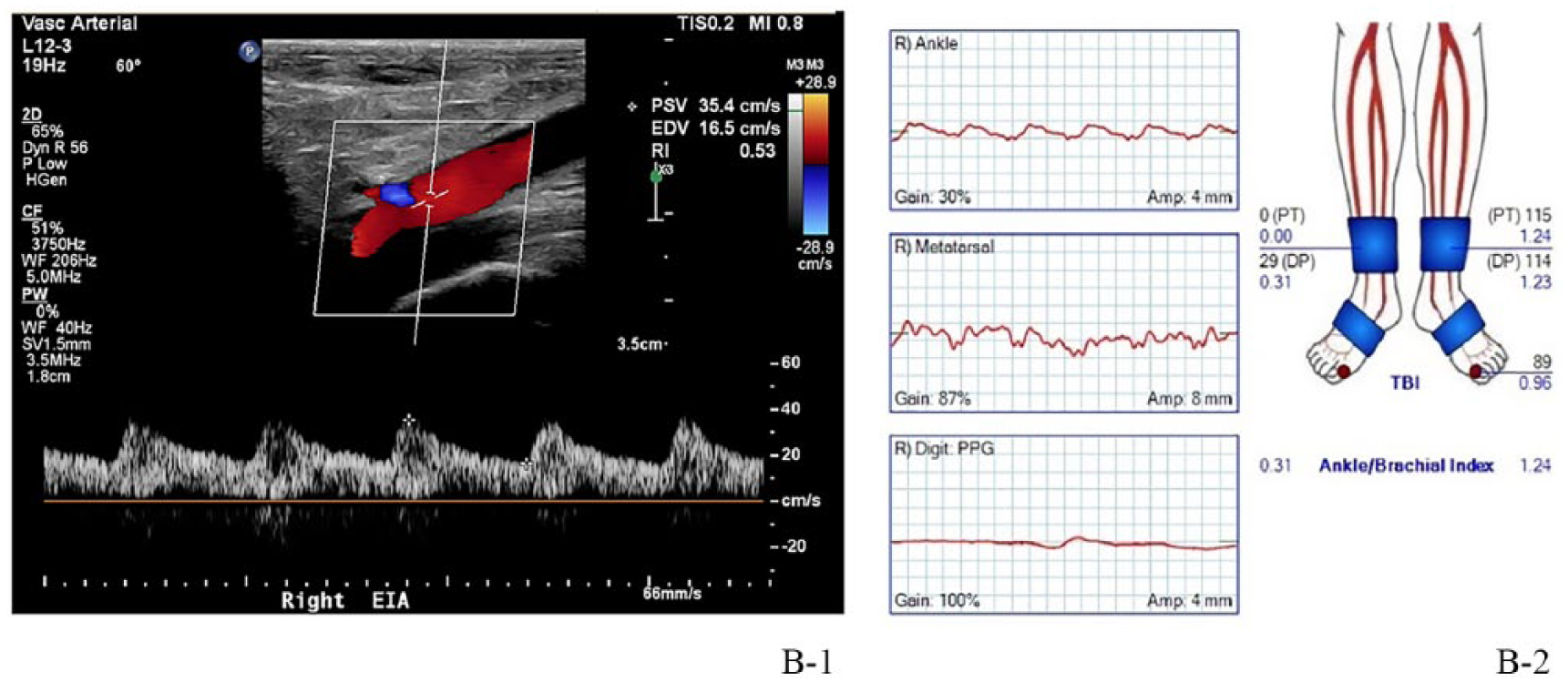
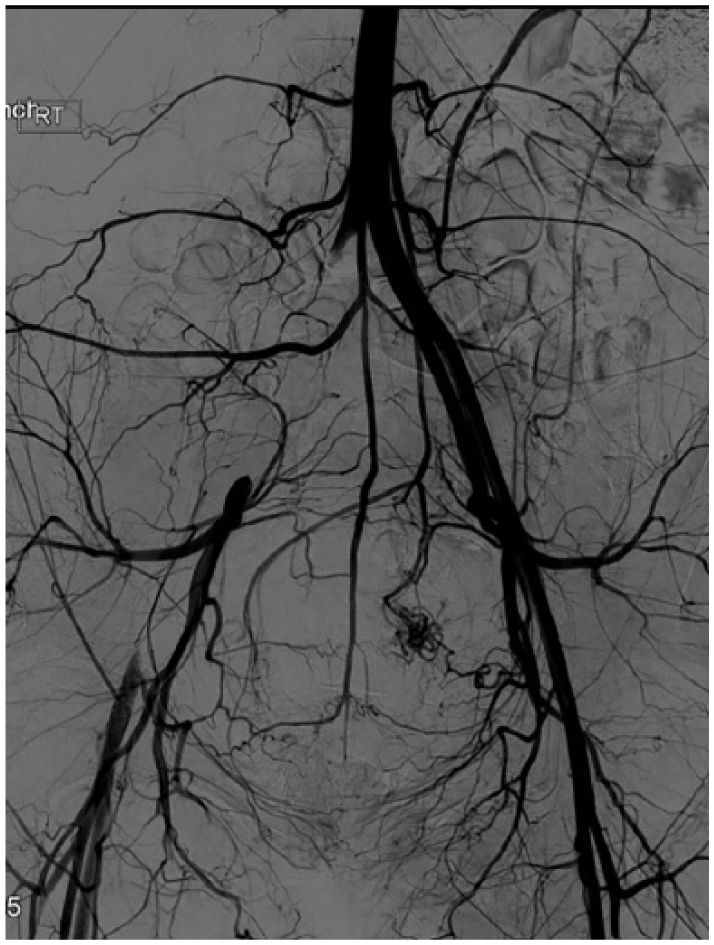
Prior to emergency mitral valve replacement, the right lower extremity was cool to touch along with delayed capillary refill and diminished pulses. The day after surgery, an arterial duplex demonstrated tardus parvus flow from the distal external iliac artery (EIA) to the ankle, suggestive of proximal occlusion (Panel B-1: peak systolic velocity; end diastolic velocity; EIA). Ankle–brachial index (ABI) was 0.31 with absent pulse volume recordings at the transmetatarsal and great toe levels, indicating severe ischemia. 3 (Panel B-2: posterior tibial; dorsalis pedis; toe brachial index; photoplethysmograpy) The patient was emergently taken for an angiogram that confirmed occlusion of the right common and external iliac arteries (Panel C). She subsequently underwent surgical embolectomy. The postoperative ABI demonstrated normal with an ABI of 1.0. The embolic event in the iliac artery was attributed to the underlying mitral valve endocarditis, secondary to rat bite fever, since other causes of embolic occlusion were ruled out after extensive work up.
She received an outpatient extended antibiotic course as per infectious disease consultants. She had digital ischemia (Panel D), which required a preplanned amputation of the first three digits of the right foot. We report the first documented case of acute limb ischemia as a sequela of rat bite fever.

‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.