
Abstract

Keywords
In most cases, calf pain that occurs while walking and is relieved by rest is related to peripheral artery disease (PAD). In PAD, the arteries are narrowed due to atherosclerosis (plaque or hardening of the arteries). However, there are some less common causes of vascular leg pain that are not due to atherosclerosis. Popliteal artery entrapment syndrome (PAES) is a condition that has similar symptoms to PAD but tends to affect a younger age group. While PAD is associated with smoking, high blood pressure, high cholesterol, and diabetes, 1 PAES is more common in athletes.
What is popliteal artery entrapment syndrome (PAES)?
Popliteal artery entrapment syndrome (PAES) refers to a condition in which the popliteal artery is compressed by one of the calf muscles. The popliteal artery is the main artery running behind the knee; it supplies blood flow to the calf and foot. When it is compressed, the blood supply is reduced. This reduction in blood flow, and thus lack of oxygen, can lead to calf cramping and pain during exercise. The pain usually resolves when exercise is stopped, but, over the long term, repeated compression and release of the popliteal artery can cause permanent damage to the artery wall. This can lead to narrowing of the popliteal artery, called stenosis, that may result in pain and cramping even with just walking. In the most severe cases, permanent damage to the muscles and nerves of the leg is possible.
Who is at risk for popliteal entrapment?
PAES can either be congenital (from birth) or acquired (develops later in life). In the congenital form, one of the calf muscles, most commonly the gastrocnemius muscle, takes an abnormal position during fetal development, which results in an abnormal path of the popliteal artery. In the acquired form, enlargement of one of the calf muscles results in compression of the popliteal artery.
Regardless of the cause, the symptoms of PAES usually do not occur until people are in their late teens or 20s. A typical patient is a young athlete without any of the traditional atherosclerotic risk factors (e.g. no smoking or diabetes). People who do activities that promote rapid muscle growth, such as weight resistance training or high-intensity circuit training, are at the highest risk. Although PAES can affect both men and women, 83% of cases occur in men, 2 probably due to the rapid muscle growth that occurs during puberty in this group.
What causes popliteal entrapment?
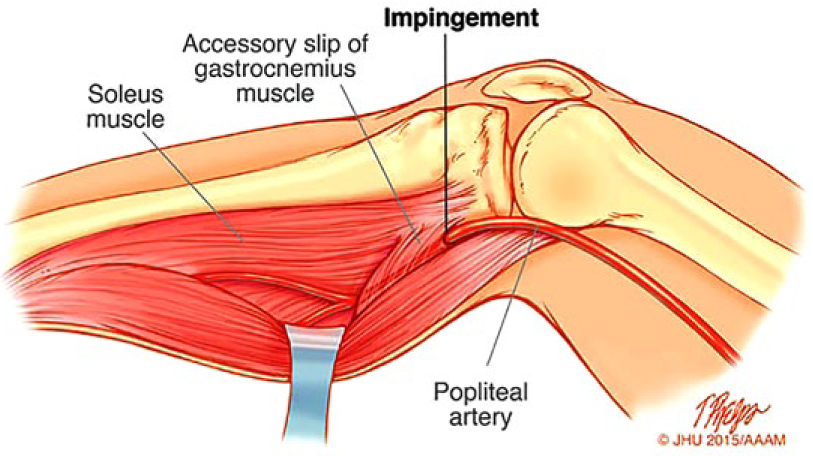
PAES is most commonly caused by compression of the popliteal artery by the medial head of the gastrocnemius muscle, which is the inner portion of the calf muscle that inserts at the level of the knee (Figure 1). When the gastrocnemius muscle is stressed, such as during exercise, it causes a reduction in the blood flow through the popliteal artery to the lower leg.
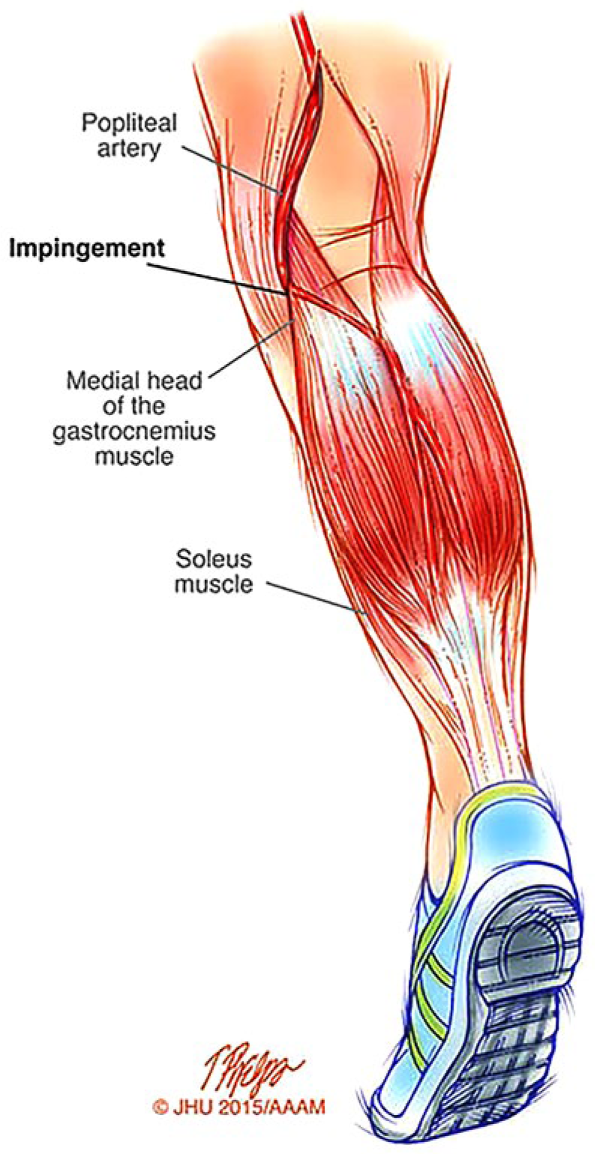
Popliteal artery entrapment.
What are the signs and symptoms of PAES?
The characteristic symptom of PAES is pain or cramping in the calf that is brought on by exercise. In the acquired form, the calf muscles can press on the nearby popliteal vein and nerve in addition to the artery, so discoloration, swelling, and numbness may also be present. PAES does not usually result in pain in the legs at rest. In fact, rest usually resolves the symptoms. Importantly, the pain or cramping usually affects younger people who are otherwise healthy; it is rarely the cause of exertional calf pain in patients over 40 years of age.
How is PAES diagnosed?
The diagnosis of PAES can often be challenging to make because it is a relatively uncommon condition that affects otherwise healthy young adults. Most PAES patients retain good pulses in their feet at rest because the arteries themselves are normal. Therefore, the physical exam is usually normal. 2
The first step in making the diagnosis is the exercise ankle–brachial index (ABI). This non-invasive blood flow test is performed before and after exercise. Blood pressure cuffs are used to measure the pressures in both arms and legs at rest. 3 The blood pressure at the ankle should be higher than the arm pressure; this ratio (ankle pressure divided by arm pressure) is the ABI and it should normally be higher than 1.0. The patient is then asked to walk on a treadmill until the cramps occur. The ankle and arm pressure measurements are then repeated after the patient stops to rest. In patients with normal blood flow to the legs, the ABIs should generally stay the same with exercise. In a patient with PAES, the ABI will decrease with exercise because the popliteal artery is being compressed, causing the ankle pressure to drop (Figure 2).
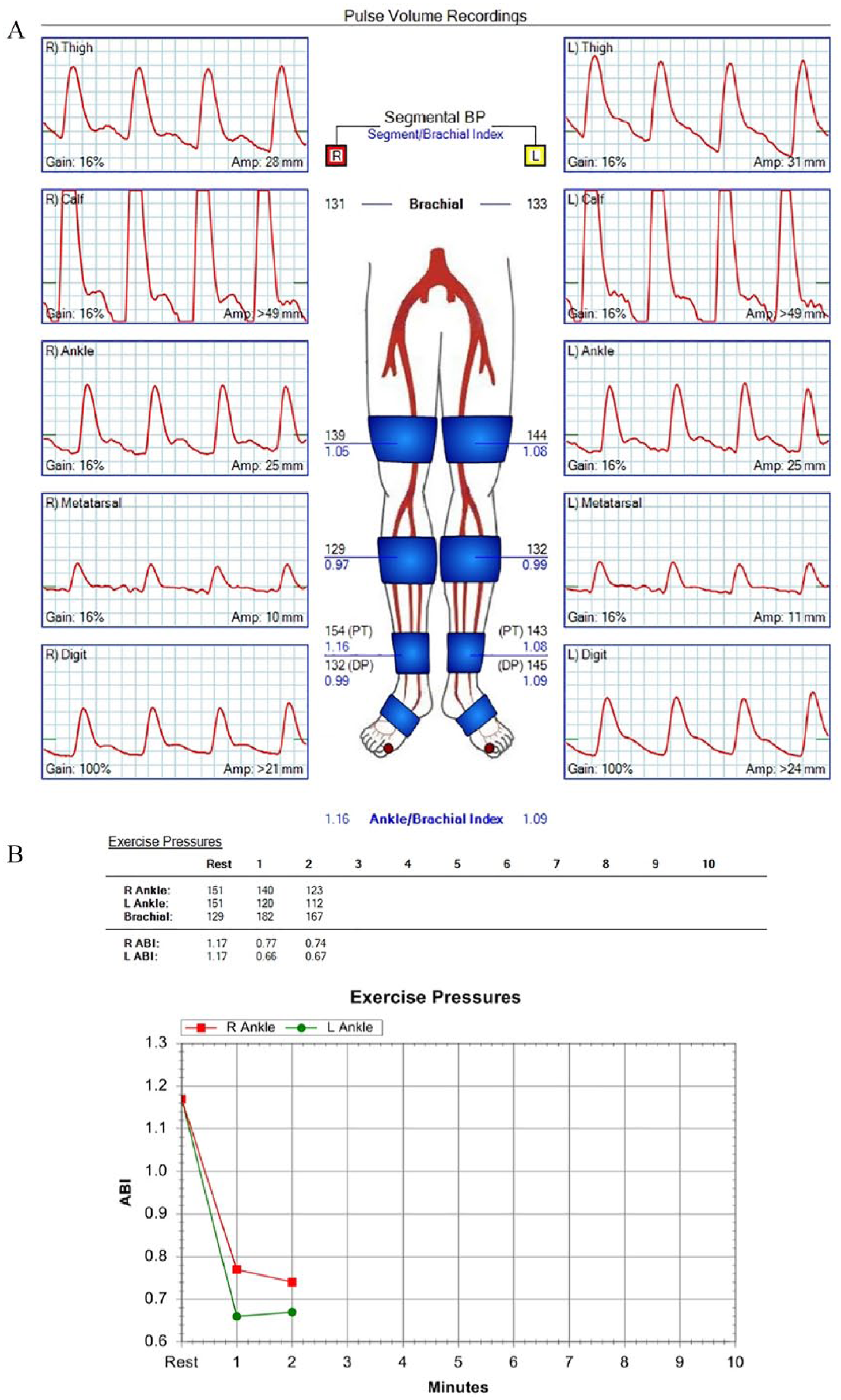
A 33-year-old man with a history of PAES. (A) Resting arterial testing and (B) post-exercise ABIs. The top panel (A) is relatively normal at rest; however, there was a significant drop in the ABIs (B) on both sides after treadmill exercise (from 1.17 to 0.77 on the right and from 1.17 to 0.66 on the left) due to popliteal artery entrapment.
Duplex ultrasound is another non-invasive study that can assist in making the diagnosis of PAES. Duplex ultrasound shows the speed of blood flow through the arteries and can be used to measure changes in blood flow before and after exercise or with maneuvers that are known to make popliteal compression worse (e.g. flexing the ankles).
Magnetic resonance angiography (MRA) or computed angiography (CTA) are also commonly used types of imaging that can help make the diagnosis of PAES. Both MRA and CTA can show the relationship of the popliteal artery with the gastrocnemius muscle and can be performed either in one position (static) or before and after maneuvers. For example, patients may undergo an initial set of images while lying on their back with their feet pressed against a board, and then again with their toes pointed downward. In patients with PAES, the first position usually results in normal-appearing arterial anatomy and blood flow, whereas the second results in popliteal narrowing or lack of blood flow. The benefit of MRA over CTA is that it avoids radiation exposure, but the test can take more time.
If the diagnosis of PAES remains unclear after completing the above imaging studies, a diagnostic angiogram can be performed. This study is more invasive than the others, but it allows the doctor to visualize blood flow through the popliteal artery in real time. Similar to the other studies, maneuvers that are known to make popliteal compression worse in patients with PAES can be performed during the angiogram to evaluate changes in blood flow in certain positions. If the arteries otherwise appear normal but there is a narrowing in the popliteal artery behind the knee with the maneuvers, then the diagnosis of PAES is confirmed (Figure 3). Angiography with maneuvers can confirm a diagnosis of PAES in 97–100% of cases. 4

A 23-year-old man who developed severe calf pain while running. Symptoms began after he started intensive exercise training when he joined the military. He was running a 6-minute mile and over 30 miles per week. The angiogram shows impingement of the popliteal artery (arrow).
If the diagnosis is not PAES, what else could it be?
Because PAES usually occurs in young athletes, many affected patients are presumed to have muscle strains or tears initially. This is especially true because PAES often does not appear until affected people begin intense athletic or weight training regimens. As a result, patients with PAES commonly see several different doctors about their symptoms before the diagnosis is finally made. Other conditions that have similar symptoms to PAES include stress fractures and compartment syndrome, which occurs when a rapid growth in the calf muscles causes tightness in the lower leg. The average time from the onset of symptoms to the diagnosis of PAES has been estimated to be 12 months (range 4 hours to 120 months). 4
The symptoms of PAES are also very similar to symptoms of PAD. Although the causes of the two conditions are different, both can result in narrowing of the popliteal artery and subsequent calf pain with exercise. However, patients with PAES are usually young and healthy, whereas patients with PAD are usually older and have risk factors associated with atherosclerotic cardiovascular disease.
What about compartment syndrome?
Compartment syndrome is a condition when the space in the deep tissues below the knee is too small to accommodate the size of the muscles within it. This results in elevated compartment pressures, which can cause a sensation of tightness or pain in the calf. Similar to PAES, compartment syndrome can be caused by excessive growth of the calf muscles and is usually seen in athletes.
Compartment syndrome has similar symptoms to PAES but its causes and treatment are different, so making the correct diagnosis is critical. Compartment syndrome can be diagnosed by measuring the pressures in the tissues below the knee with a small needle. This test is often performed by an orthopedic surgeon. Patients with compartment syndrome will have elevated compartment pressures, especially after exercise. The surgical treatment of compartment syndrome is a fasciotomy. A fasciotomy is a surgery in which a cut is made on both the inside and outside parts of the lower leg, allowing the surgeon to open the compartments underneath the skin and release the pressure.
How is PAES treated? When is surgery recommended?
Surgery is recommended for PAES if a patient’s symptoms are significantly affecting his or her lifestyle or athletic activities. Surgery can be performed by two different approaches. 4 The first is a medial (inside) approach: a 4- to 6-inch incision is made on the inner calf just below the knee to allow for release of the popliteal artery (Figure 4). In the second approach, a similar incision is made on the back of the knee to release the artery completely. In both procedures, the part of the gastrocnemius muscle that is causing compression of the popliteal artery is released. The procedure usually has no effect on overall leg function, but prevents the muscle from compressing the popliteal artery, thus resolving the pain and cramping symptoms. Rarely, an arterial bypass is needed to reconstruct the popliteal artery. Bypass surgery is reserved for patients with long-standing PAES who have developed a narrowing of their popliteal artery as a result of chronic compression and release.
Surgery for release of the popliteal artery.
Are stents an option?
The use of metallic stents for treating PAES should be avoided in most cases. Patients with PAES usually have normal arteries, so placing a stent does not address the main cause of the problem. In addition, there is a risk of the stent cracking or becoming blocked in areas with lots of movement, such as behind the knee. Instead, releasing the muscle that compresses the popliteal artery is a more durable solution.
What are the risks and what is involved with having PAES surgery?
The surgery for treating PAES usually takes about 1 hour. Patients undergo general anesthesia and spend one to two nights in the hospital. Walking is usually encouraged starting the day after surgery, and recovery involves physical therapy exercises, including stretching and progressive exercise, after patients return home. Most patients have a favorable response to the surgery and are able to return to their normal activities, including exercise, within 4–6 weeks. A complete resolution of symptoms occurs in approximately three-quarters (75%) of patients after surgery (range 70–100%). 4
What follow-up is recommended after surgery?
After hospital discharge, regular outpatient follow-up should occur with a vascular specialist with experience in the care of patients with PAES. A duplex ultrasound and/or exercise ABIs are usually repeated 4–6 weeks after surgery to establish a new baseline. After that initial follow-up, vascular studies are usually not repeated unless symptoms recur, at which point the same tests that were used for making the initial PAES would be repeated.
Are there any restrictions on activity with PAES?
Because PAES tends to occur in patients who engage in regular exercise and/or weight training regimens, excessive strenuous activity or muscle overuse could make PAES symptoms worse. However, regular exercise is important for overall cardiovascular health, and the true cause of PAES is an anatomic abnormality of the calf muscle. Thus, no specific activity restrictions are required for patients with PAES.
Summary
Symptoms of PAES include pain and cramping of the calf muscles during exercise. Unlike PAD, PAES occurs in younger athletic patients who do not have traditional atherosclerotic risk factors. The diagnosis is often challenging because affected individuals have no obvious signs of the condition on physical exam. The use of testing with maneuvers is essential for diagnosing PAES. The treatment, if needed, involves surgery to release compression of the artery. Overall, patients tend to have good results with popliteal entrapment release and are able to return to their normal activities and exercise.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.