
Abstract

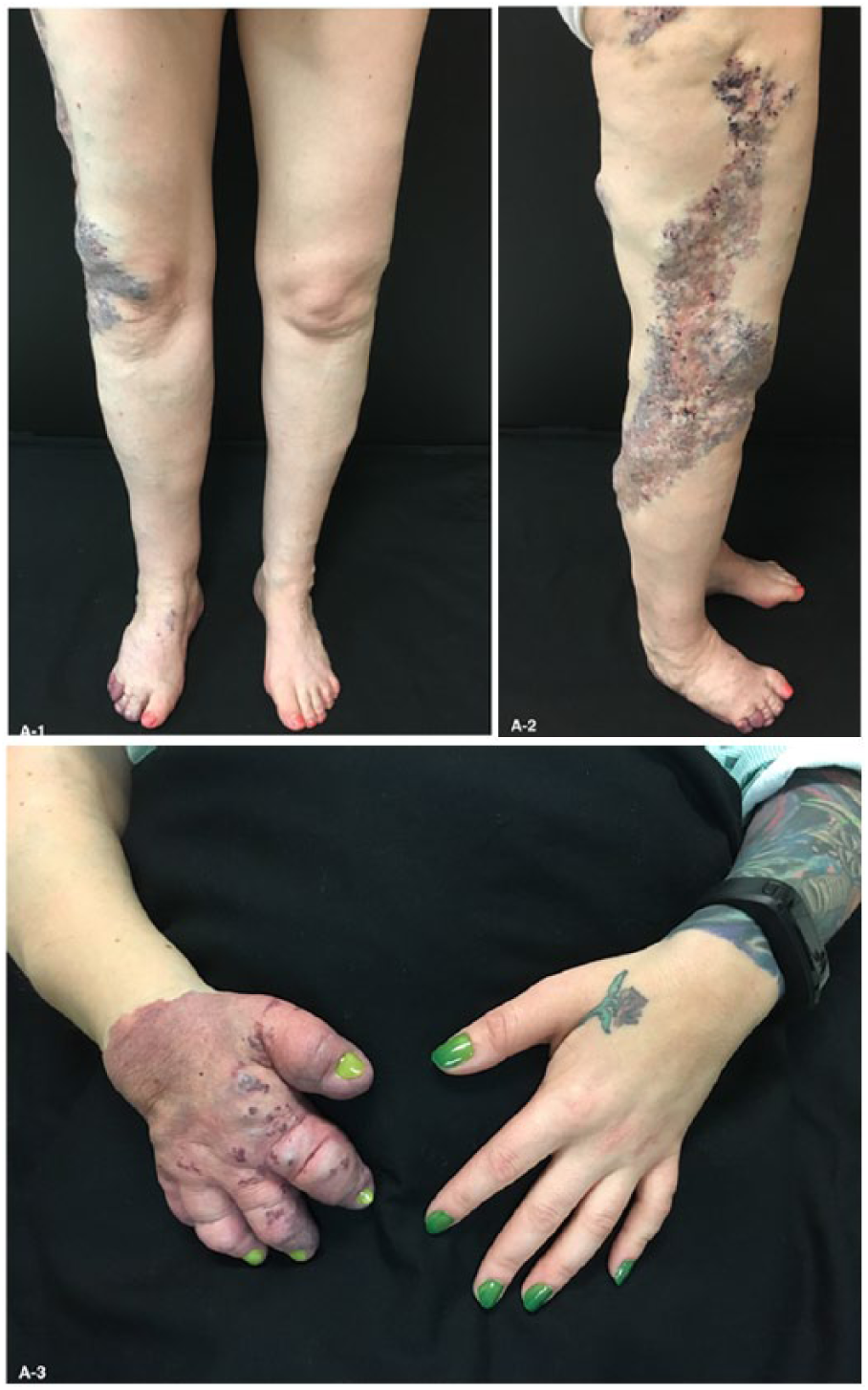
A 35-year-old woman presented in follow-up of congenital right hemihypertrophy including prominent venous and capillary malformations (Panels A-1 and A-2). The right arm was shortened and the right hand manifested extreme deformation (Panel A-3). The right foot displayed similar albeit less severe disfigurement. No thrills or bruits were detected. Venous duplex ultrasonography documented patent but ectatic refluxing deep veins, and magnetic resonance angiography illustrated diffusely infiltrating serpiginous venous malformations. No arteriovenous malformations suggestive of Parkes–Weber syndrome (PWS) were identified. Radiographs of the right hand displayed diffuse osseous hypotrophy, cortical attenuation, and phleboliths (Panel B). Although her long-standing putative diagnosis was Klippel–Trenaunay syndrome (KTS), a diagnosis of Servelle–Martorell syndrome (SMS) or angio-osteohypotrophic syndrome was correctly rendered. Intervention with sclerotherapy was offered, which she deferred, and she opted for use of continued gradient compression stockings.

As this case illustrates, SMS is frequently misdiagnosed as other vascular malformations such as KTS and PWS. Common features of vascular malformation syndromes include combinations of cutaneous capillary–lymphatic–venous malformations resulting in port-wine stains, limb overgrowth, soft tissue swelling, and varicose veins. In contradistinction to the osseous hypertrophy and limb lengthening typically encountered in KTS and PWS, SMS manifests bony hypotrophy and hypoplasia with limb shortening. Additionally, grotesque limb distortion and unusually numerous radiographic phleboliths are more likely to complicate SMS. High-flow arteriovenous malformations are typically absent in SMS and, when present, suggest the diagnosis of PWS. 1
When one of these syndromes is suspected, a meticulous history and physical examination should be performed. Diagnostic testing should begin with duplex ultrasonography and standard plain X-ray. Subsequent contrast-enhanced magnetic resonance imaging assists in defining the subtype of vascular malformation and in planning intervention. 2
The preferred treatment of vascular malformations is conservative management, which includes skin care and compression therapy. Intervention should be reserved for those with severe symptoms or complications. A multidisciplinary team approach at an experienced center should be used when considering intervention. Sclerotherapy is typically first-line, with surgery reserved for correction of hemodynamic derangements. 3
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.