
Abstract

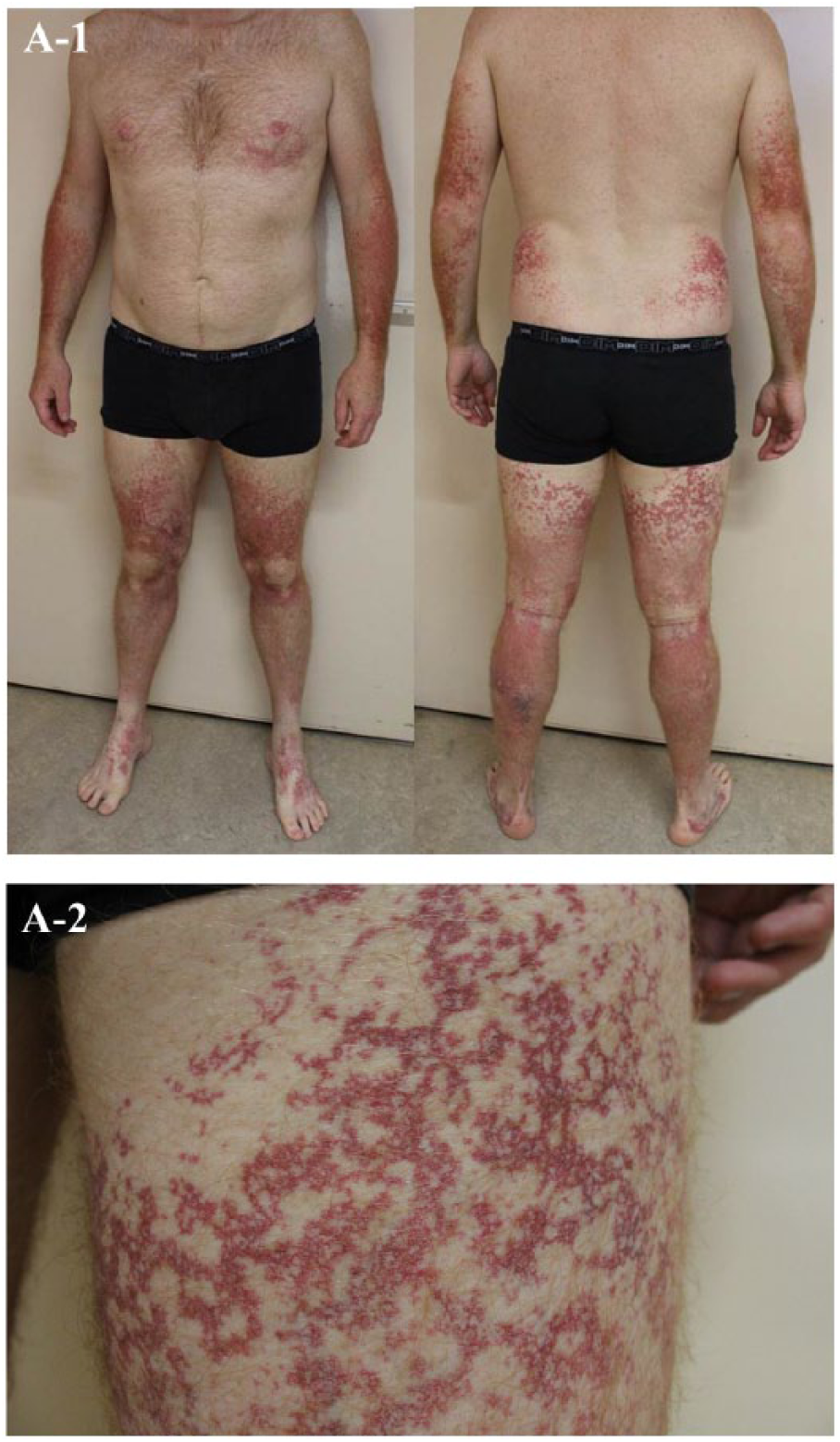
A 38-year-old man presented with a 25-year history of asymptomatic multiple telangiectasias on his trunk, arms, and legs. These initially appeared on his feet and ankles, and gradually spread to reach his trunk and arms (Panel A-1; Panel A-2: detail of the thigh). Clinical examination was otherwise normal without rash or itching. No relevant family history and no clinical evidence of systemic disease were apparent.
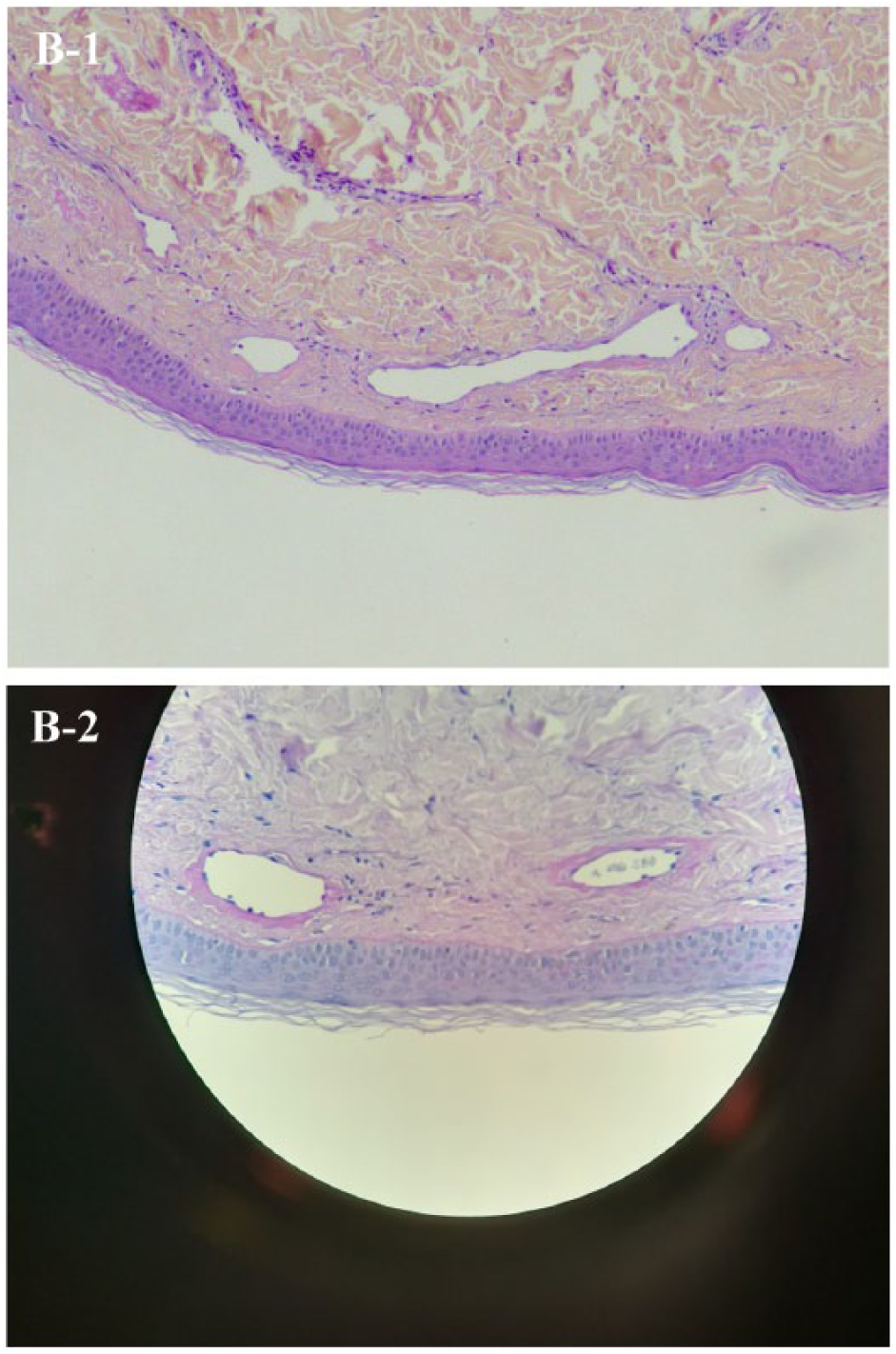
Routine blood analyses were within normal limits. Venous Doppler ultrasonography was normal without venous insufficiency. A biopsy specimen obtained from the thigh wall revealed dilated vascular spaces in the upper dermis, with perivascular hyalinization, highlighted with period acid–Schiff (PAS). Collagen IV deposition around the basal lamina of the telangiectasia was observed. There was no perivascular inflammatory infiltrate, no microvascular arteriovenous anastomoses, a normal numbers of mast cells, and no indication of amyloid deposition. Histopathological examination with May–Grünwald–Giemsa (MGG) coloration shows some large vessels in the upper dermis, with thick hyalinized walls (Panel B-1); PAS shows collagen deposition (Panel B-2).
The clinical, histopathological and immunohistochemical findings were consistent with cutaneous collagenous vasculopathy (CCV). 1 The first case was reported in 2000 by Salama et al. 2 CCV is characterized by the progressive development of asymptomatic symmetric telangiectasias that typically arise in the lower extremities and gradually spread to the trunk and upper limbs, sparing the mucosal surface. No difference between men and women is reported in the literature. Principal differential diagnoses are hereditary hemorrhagic telangiectasia (HHT), hereditary benign telangiectasia (HBT), and generalized essential telangiectasia (GET). 3
Clinically, CCV is indistinguishable from these three pathologies, but histologic analysis reveals the characteristic thickening of capillary walls. HHT is characterized by a family history of similar telangiectasias and/or abnormal bleeding, with mucosal involvement in the cutaneous biopsy. HBT has a dominance inheritance and is characterized by extensive telangiectasia on the upper body, which starts in childhood, without systemic lesions. In this case, the first appearance of telangiectasia at 13 years old and the lack of familial cases do not support this diagnosis.
GET is characterized by symmetrical telangiectasia on the lower body, which starts in late childhood or early adult life, much more in women than men. Mucosal and conjunctival lesions have been reported. Histopathology is characterized by dilatation of post-capillary venules on the upper horizontal plexus, without collagen deposition around the basal lamina of the vessels.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.