
Abstract
The primary objectives of this work were: (1) to describe trends in HIV prevalence among those undergoing carotid intervention (carotid endarterectomy or carotid artery stenting) in the United States; and (2) to determine if HIV infection is independently associated with symptomatic carotid atherosclerotic disease or age at the time of carotid intervention. In a nationally representative inpatient database from 2004 to 2014, HIV infection was associated with younger age at the time of carotid intervention (59 years [SE 0.2] vs 71 years [SE 0.01], p < 0.001), male sex (83% vs 58%, p < 0.001), black race (21% vs 4%, p < 0.001), and symptomatic carotid atherosclerotic disease (18.8% vs 11.0%, p < 0.001). Among those undergoing carotid intervention, there was a significant increase in the prevalence of HIV from 0.08% in 2004 to 0.17% in 2014 (p < 0.001). After adjustment for patient demographics, comorbidities and other covariates, HIV infection remained significantly associated with younger age (–8.9 years; 95% CI: –9.7 to −8.1; p < 0.001) at the time of carotid intervention, but HIV infection was not independently associated with symptomatic carotid atherosclerotic disease.
Background
Owing to advancements in HIV care, survival alone is no longer an acceptable outcome for persons living with HIV. As fewer AIDS-defining illnesses claim the lives of persons with HIV in the United States (US), this population now contends with the increased risk of ischemic stroke, 1 among other cardiovascular diseases. Indeed, the proportion of cardiovascular disease-related deaths among persons with HIV in the US has more than doubled between 1999 and 2013. 2
Persons with HIV have a higher prevalence of traditional ischemic stroke risk factors including cigarette smoking, 3 hypertension,4,5 and diabetes mellitus. 6 Antiretroviral therapy (ART) also influences many of these risk factors, 7 while the virus itself contributes to stroke risk through chronic inflammation-mediated mechanisms.8,9 Prevention of first or recurrent ischemic stroke can take the form of medical therapy or carotid intervention, defined here as carotid endarterectomy (CEA) and carotid artery stenting (CAS). There are, however, few data that describe the characteristics of persons with HIV at the time of CEA or CAS. To that end, the primary objectives of this analysis were: (1) to describe trends in prevalence of HIV infection among those undergoing carotid intervention; and (2) to determine if HIV infection is independently associated with symptomatic carotid atherosclerotic disease or younger age at the time of surgery. A secondary objective was to visualize and compare trends in age, comorbidity burden and the prevalence of symptomatic carotid atherosclerotic disease at the time of carotid intervention between those with and without HIV infection.
Methods
Dataset
For this retrospective, serial, cross-sectional study, we used the 2004 through 2014 National Inpatient Sample (NIS) 10 / Nationwide Inpatient Sample11,12 (Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality). The NIS is an all-payer, administrative, discharge-level database of hospitalizations. It is stratified on hospital characteristics, clustered by hospital, and contains 20% of discharges in the target universe. The NIS defines its target universe as all discharges from community hospitals in the US, and its sampling frame is > 95% of the target universe. Using supplied trend weights, 13 the NIS can describe national trends. The database is de-identified and meets the criteria of the Health Insurance Portability and Accountability Act to protect personal information. This study was approved and exempted from the consent requirement by the University of California, San Diego institutional review board.
Study population, outcomes, and covariates
The study sample was defined as all admissions of patients aged 18 years or greater, during which a CEA or CAS was performed. CEA and CAS were identified using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes 38.12 and 00.63, respectively. HIV-associated admissions (‘HIV+’) were identified by Clinical Classification Software (CCS) code ‘5’, and all other admissions in the sample were defined as ‘HIV–’. Symptomatic carotid atherosclerotic disease was defined by having any of the following ICD-9-CM diagnosis codes as an admission diagnosis: 362.30, 362.31, 362.32, 362.33, 362.34, 362.84, 433.11, 433.31, 433.91, 435.8, 435.9, 436, 434.11 and 434.91. Descriptions of these ICD-9-CM codes are shown in Supplementary Table 1. Records that were not associated with any of the aforementioned ICD-9-CM codes were classified as having asymptomatic carotid atherosclerotic disease. The NIS reports patient age, sex, race, primary payer, median household income of a patient’s ZIP code by quartile, admission year and month, elective admission (yes/no), weekend admission (yes/no), hospital region, hospital ownership, hospital type, and hospital bed size for each hospitalization. Using the Elixhauser comorbidity index,14,15 we calculated a van Walraven comorbidity score, which has been validated as a measure for disease burden in hospitalized patients and was predictive for inpatient mortality. 16 From the Elixhauser comorbidity index, we adapted hypertension (uncomplicated and complicated), diabetes (uncomplicated and complicated), peripheral vascular disease, obesity, hypothyroidism and drug use as covariables. We further identified history of/current tobacco use (ICD-9-CM diagnosis codes 30.51, V15.82), lipid disorders (272.0, 272.1, 272.2, 272.3, 272.4, 272.5, 272.9), and coronary artery disease (414.01, 414.2, 414.3, 414.4, 414.8, 414.9).
Statistical analysis
Statistical analysis was performed using R version 3.4.1. 17 The two-tailed significance level was set at p < 0.05, with the exception of baseline comparisons between categorical variable levels, for which a Bonferroni correction was applied. All data were weighted using NIS trend weights as mentioned above.
Missing data were handled using multiple imputation with chained equations (using R package ‘MICE’ 18 ) with five imputations and five iterations. Missing variables in the final sample were race (missing in 17.17% of cases), admission month (8.09%), median household income of patient’s ZIP code by quartile (1.97%), elective admission (0.28%), primary payer (0.13%), sex (0.05%), age (0.01%) and weekend admission (< 0.01%). Statistical tests involving any imputed variables were performed using imputed datasets, and reported as per Rubin’s rules. The analyses described below were also performed on a sample after listwise deletion of cases with missing pertinent variables, as a sensitivity analysis. The significance of statistical outcomes did not differ between the two methods of missing data handling, and therefore all findings are reported using imputed data.
Baseline characteristics between HIV+ and HIV– admissions were compared using random-intercepts, fixed-slopes mixed-effects models in order to account for the NIS’s clustered design. The random terms were hospital identifiers, and the fixed term was HIV-status. Linear models were used for continuous dependent variables, while binary logistic models were used for binary or categorical dependent variables (using yes/no for each variable level). Time trend analysis was performed using linear mixed-effects models (for continuous outcomes) or logistic mixed-effects models (for binary outcomes) with year and month of admission as the predictor variable; hospital identifier was the random term in each model. The significance of the difference in trend slopes by HIV-status was determined by the interaction term between time and a dummy variable representing HIV infection.
Multivariable mixed-effects models were used to determine the independent association between HIV infection and two outcomes: (1) age at the time of carotid intervention; and (2) symptomatic carotid atherosclerotic disease. For each outcome, four successive models were used to assess the degree of effect attenuation attributable to each cluster of variables. Model 1 was adjusted for patient sex (and age, when the outcome was ‘symptomatic carotid atherosclerotic disease’). Model 2 was further adjusted for patient race, primary payer and quartile of median income of the patient’s ZIP code. Model 3 was further adjusted for tobacco use, uncomplicated hypertension, complicated hypertension, uncomplicated diabetes, complicated diabetes, lipid disorders, coronary artery disease, peripheral vascular disease, obesity, hypothyroidism, drug use, and the van Walraven comorbidity score. Finally, Model 4 was further adjusted for weekend admission, elective admission, and hospital-level variables (region, ownership, location/teaching status, and bed size). Hospital identifier was used as the random term in all models.
Results
Baseline characteristics
A case selection flow chart is shown in Figure 1. From 2004 through 2014, 1,314,938 hospitalizations that involved a CEA or CAS were included for analysis. Among those, 1649 admissions (0.13%) had an associated HIV diagnosis.
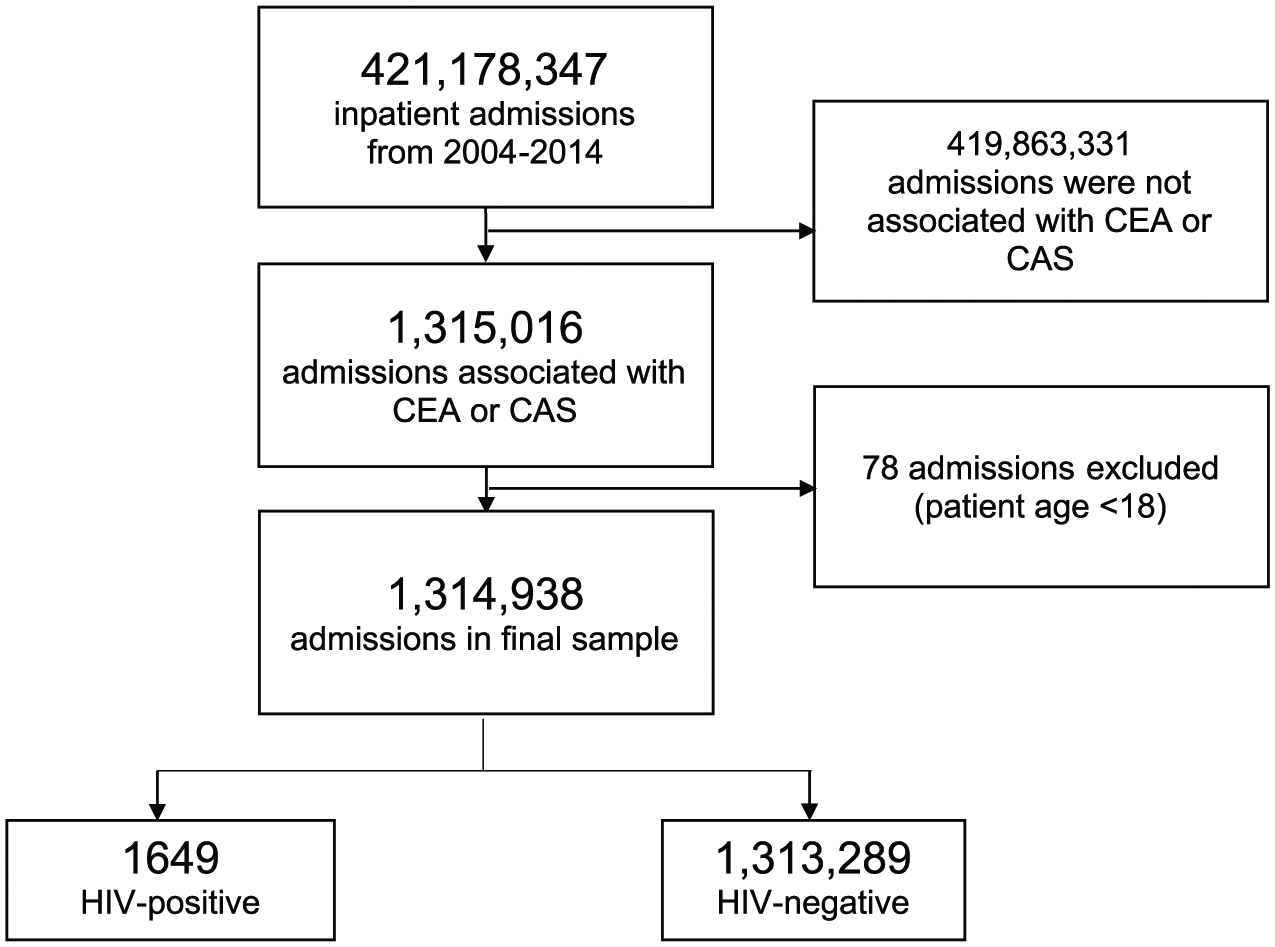
Case selection flow chart from the NIS.
Baseline characteristics compared by HIV-status are shown in Table 1, and a relative frequency histogram for age at the time of carotid intervention is shown in Figure 2. Among hospitalizations that involved a carotid intervention, HIV+ admissions were more likely to be young, male, and black. HIV+ admissions were less likely to be elective, and more likely to be a weekend admission. HIV+ admissions were also more likely to occur in the South, and less likely in the West. Van Walraven comorbidity scores were significantly greater among HIV+ admissions than HIV– admissions (median 3 [IQR, 0–8] vs 2 [0–5], p < 0.001). A comparison of comorbidities between HIV+ and HIV– admissions is shown in Table 2.
Baseline characteristics.
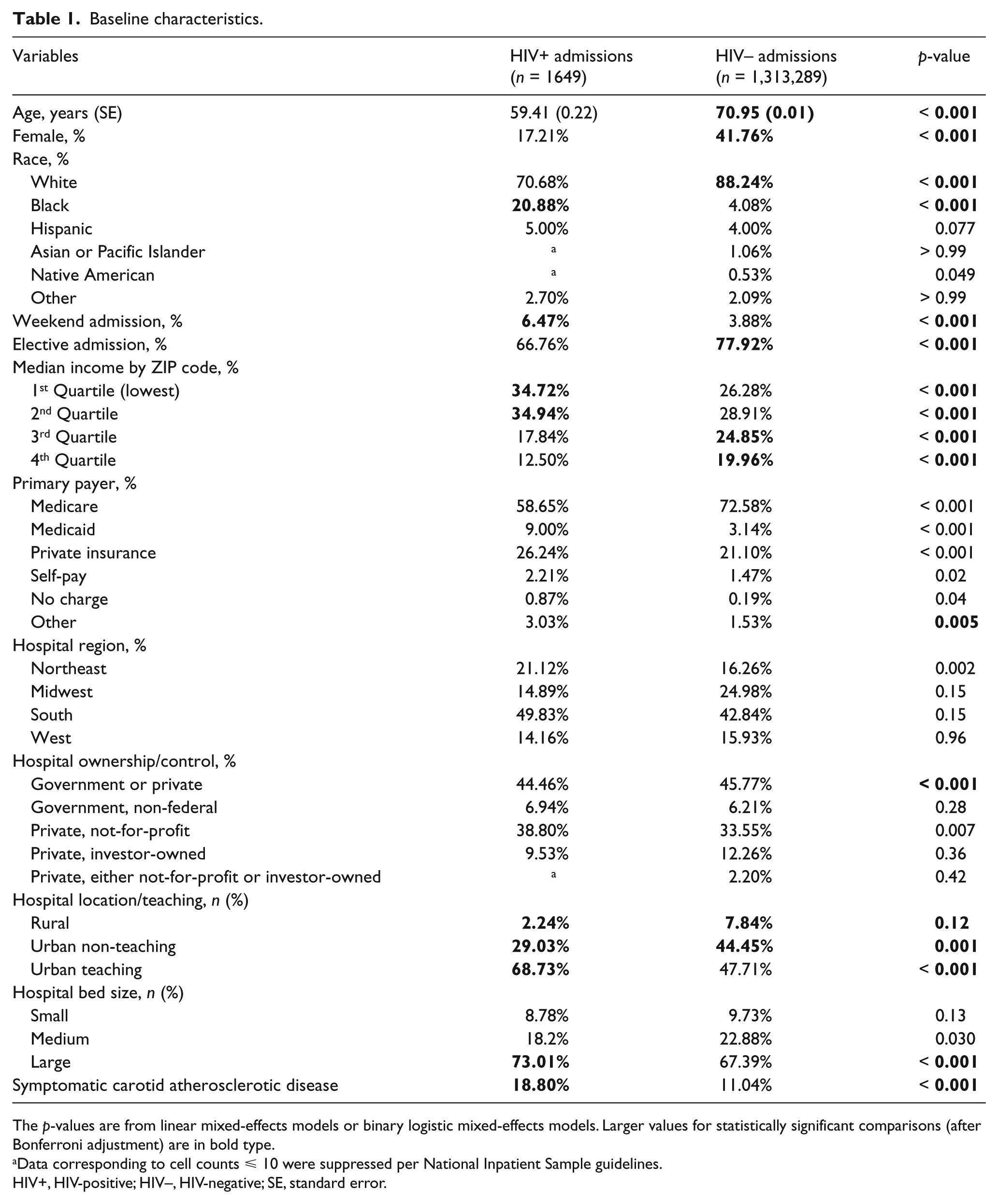
The p-values are from linear mixed-effects models or binary logistic mixed-effects models. Larger values for statistically significant comparisons (after Bonferroni adjustment) are in bold type.
Data corresponding to cell counts ⩽ 10 were suppressed per National Inpatient Sample guidelines.
HIV+, HIV-positive; HIV–, HIV-negative; SE, standard error.
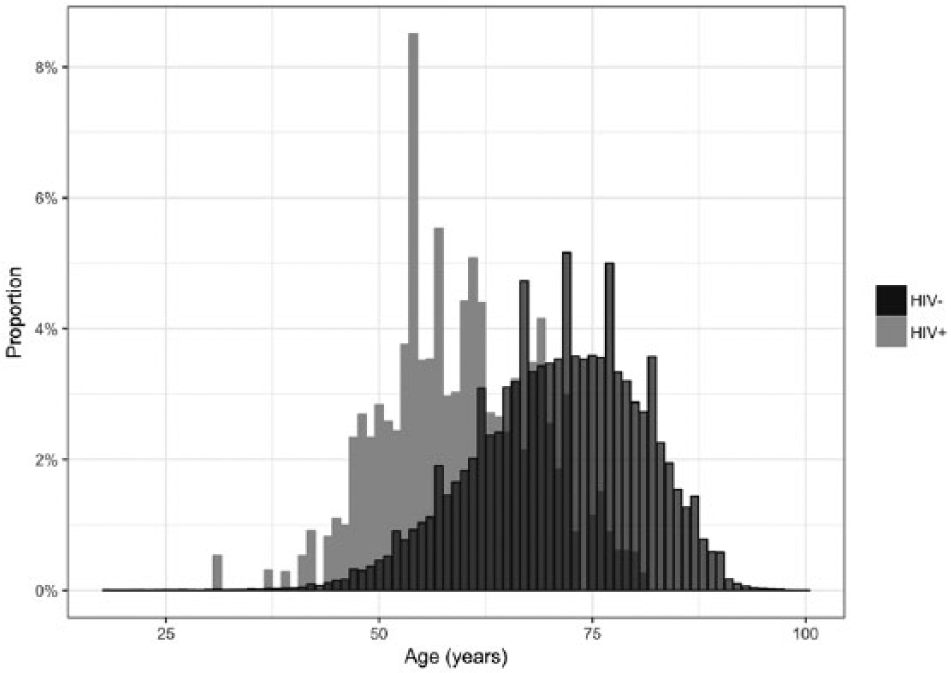
Relative frequency histogram of age at time of carotid intervention for HIV+ and HIV– admissions.
Comparison of the prevalence of comorbidities between HIV-positive and HIV-negative admissions.
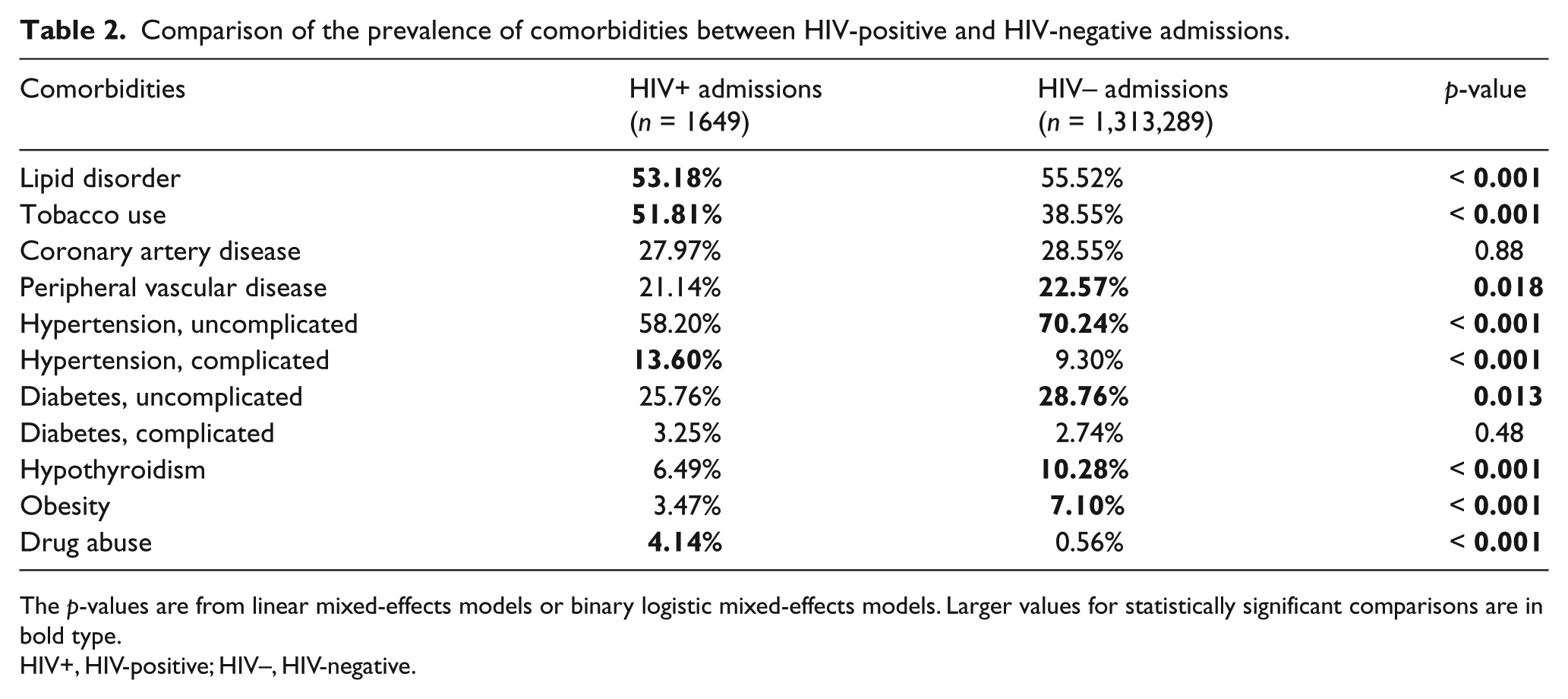
The p-values are from linear mixed-effects models or binary logistic mixed-effects models. Larger values for statistically significant comparisons are in bold type.
HIV+, HIV-positive; HIV–, HIV-negative.
Among hospitalizations that involved a carotid intervention, HIV+ admissions were more likely to have symptomatic carotid atherosclerotic disease than HIV– admissions (18.80% vs 11.04%, p < 0.001). In those with asymptomatic carotid atherosclerotic disease, HIV+ admissions were 10.85 years younger (95% CI: 9.75 to 11.95; p < 0.001), while in those with symptomatic carotid atherosclerotic disease, HIV+ admissions were 10.02 years younger (95% CI: 7.43 to 12.62; p < 0.001).
National trends
The proportion of carotid interventions associated with HIV infection significantly increased during the study period (+0.014% per year; 95% CI: 0.008% to 0.019%; p < 0.001). In 2004, 0.08% of carotid interventions were associated with HIV infection, and that figure increased to 0.17% in 2014.
Figure 3 shows trends over time for patient age, van Walraven comorbidity score, and having symptomatic carotid atherosclerotic disease at the time of surgery. There was an upward trend in age (+0.35 years per year; 95% CI: 0.04 to 0.65; p=0.028) among HIV+ admissions, and a downward trend in age among HIV– admissions (–0.02 years per year; 95% CI: –0.04 to −0.01; p=0.005); the difference in trend slopes was significant (p=0.028). Van Walraven comorbidity scores increased in both HIV+ admissions (+0.38 points per year; 95% CI: 0.14 to 0.62; p=0.002) and HIV– admissions (+0.12; 95% CI: 0.11 to 0.13; p < 0.001); the difference in trend slopes was significant (p=0.009). The odds of presenting with symptomatic carotid atherosclerotic disease increased among HIV+ admissions (15.14% increase in odds per year; 95% CI: 5.34% to 24.94%; p=0.003) and HIV– admissions (4.45% increase in odds per year; 95% CI: 4.24% to 4.48%; p < 0.001); the difference in trend slopes was significant (p < 0.001).
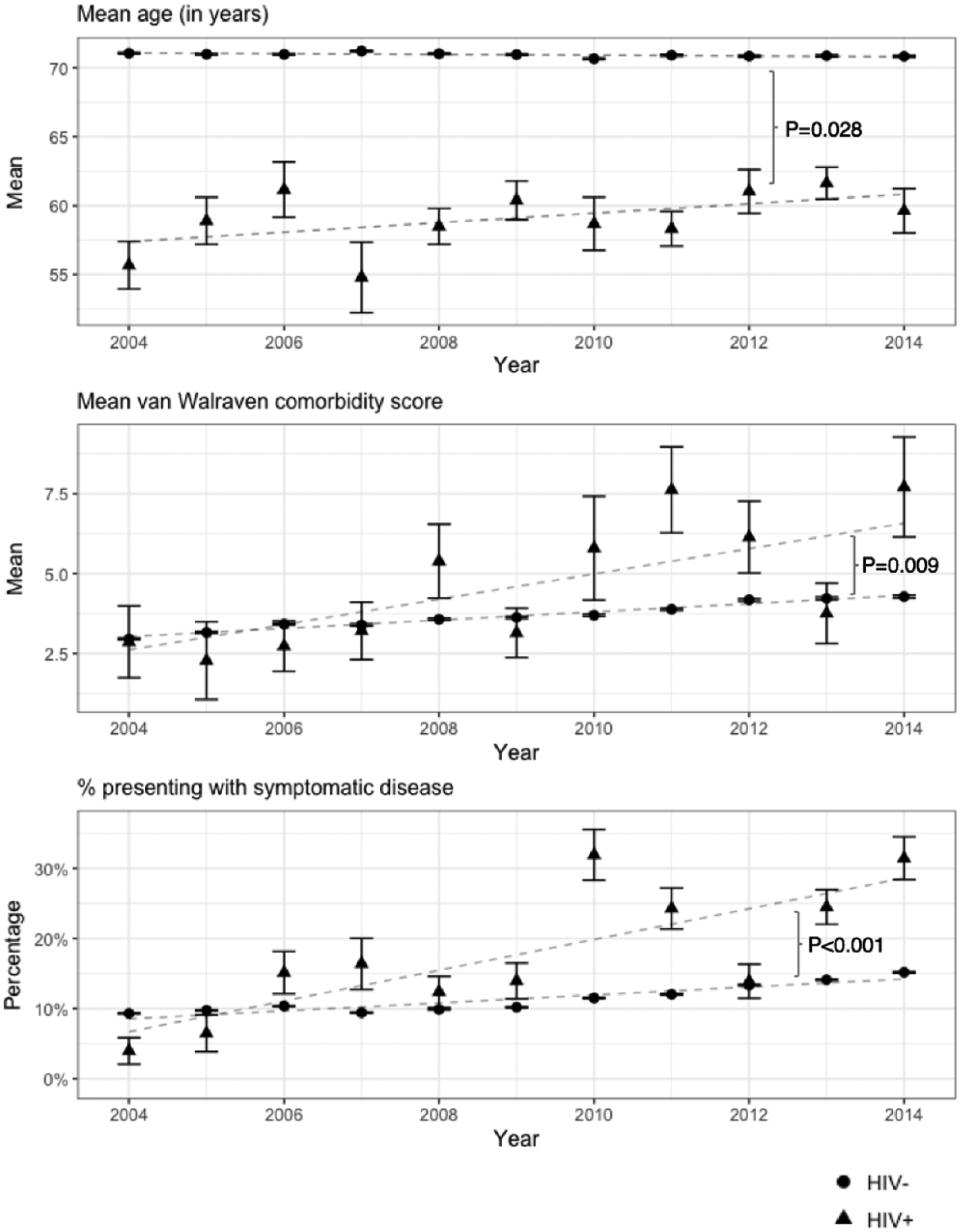
Trends from 2004 through 2014 among HIV+ and HIV– admissions.
Regression models
Results of multivariable mixed-effects regression models for age and symptomatic carotid atherosclerotic disease at the time of carotid intervention are shown in Table 3. HIV infection was significantly associated with younger age at the time of carotid intervention (–8.93 years; 95% CI: –9.73 to −8.13; p<0.001) in Model 4 (the fully adjusted model). A non-significant association between HIV infection and symptomatic carotid atherosclerotic disease (odds ratio 1.31; 95% CI: 0.99 to 1.74; p=0.055) remained after adjusting for patient age and sex, and this trend disappeared in the final adjusted model (odds ratio 1.00; 95% CI: 0.72 to 1.38; p=0.98).
HIV infection as a predictor for age and for symptomatic carotid atherosclerotic disease at the time of carotid intervention in mixed-effects regression models.
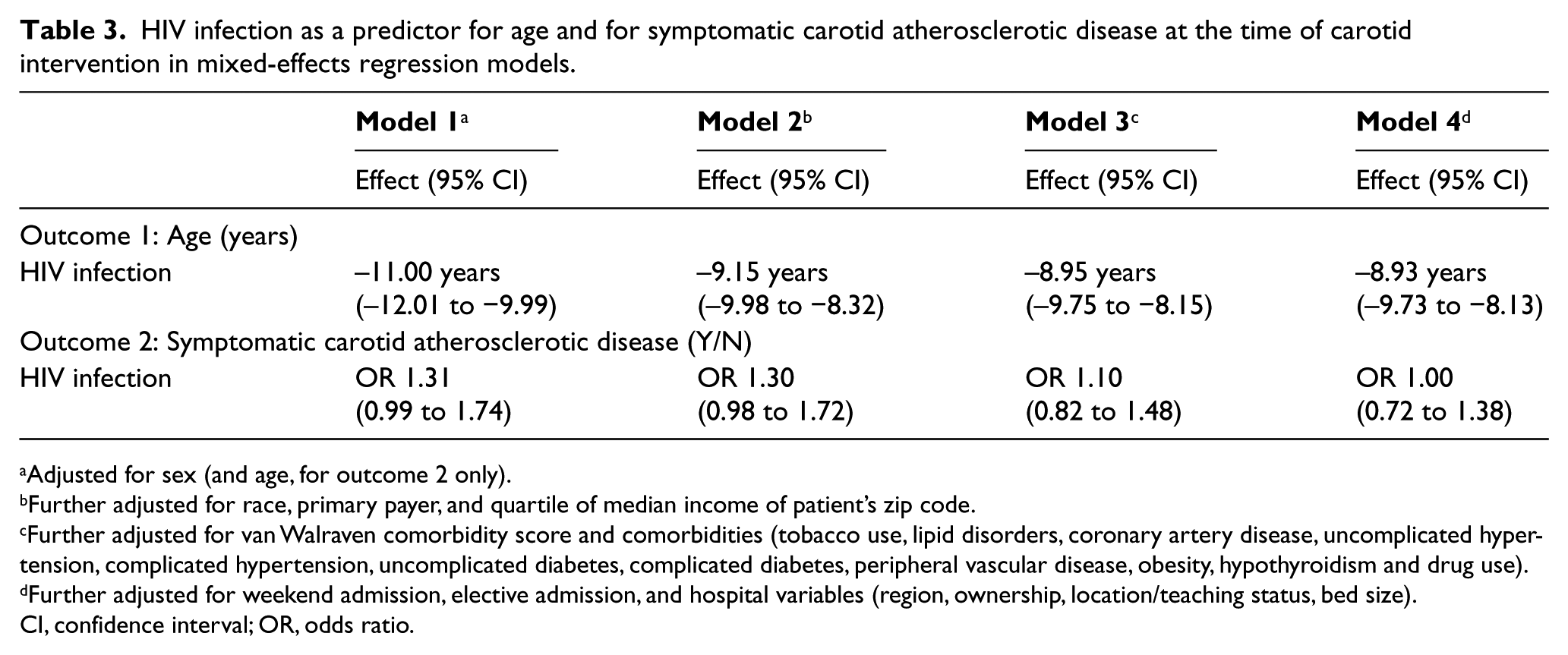
Adjusted for sex (and age, for outcome 2 only).
Further adjusted for race, primary payer, and quartile of median income of patient’s zip code.
Further adjusted for van Walraven comorbidity score and comorbidities (tobacco use, lipid disorders, coronary artery disease, uncomplicated hypertension, complicated hypertension, uncomplicated diabetes, complicated diabetes, peripheral vascular disease, obesity, hypothyroidism and drug use).
Further adjusted for weekend admission, elective admission, and hospital variables (region, ownership, location/teaching status, bed size).
CI, confidence interval; OR, odds ratio.
When regression analysis was performed after stratifying by symptomatic or asymptomatic carotid disease, similar associations between HIV infection and age at the time of surgery were seen. Among those with symptomatic disease, HIV infection was significantly associated with younger age at the time of carotid intervention in Model 4 (–8.71 years; 95% CI: –10.70 to −6.72). Among those with asymptomatic disease, HIV infection was also significantly associated with younger age at the time of carotid intervention in Model 4 (–8.97 years; 95% CI: –9.85 to −8.09).
Discussion
This is the first study to describe and compare persons with and without HIV infection who underwent carotid intervention across the US. HIV infection was associated with younger age at the time of intervention (by more than 10 years) among those with or without symptomatic carotid atherosclerotic disease. A clinically and statistically significant association with younger age at the time of intervention remained after adjustment for patient demographics, comorbidities, and hospital-level covariates. One possible reason why relatively young persons with HIV are undergoing surgery for asymptomatic carotid disease is that they are diagnosed with comorbid diseases, such as acute myocardial infarction 19 or peripheral artery disease, 20 at a younger age on average. These diagnoses then lead to work-ups that identify subclinical carotid disease. Data also show that HIV infection is associated with accelerated growth of carotid intima–media thickness 21 as well as greater relative risk of developing new focal plaque. 22 Accelerated subclinical disease can then of course lead to earlier manifestation of symptomatic disease. In a recent retrospective study with 120 patients (60 with HIV infection), Chow et al. (2017) 23 reported that HIV-infected individuals were approximately 10 years younger at the time of ischemic stroke than those without HIV infection, which closely mirrors our findings.
We also show that the proportion of patients undergoing CEA or CAS who have HIV infection has doubled from 0.08% in 2004 to 0.17% in 2014. As a reference, the prevalence of diagnosed HIV infection was estimated to be 0.30% in 2014. 24 This finding may be a function of prolonged survival among persons with HIV, which is also reflected in the upward trend in age at the time of intervention that we found. The prevalence of HIV infection among those undergoing carotid intervention will likely continue to approach that seen in the general population as the HIV-infected population ages. 25 As for the trends showing increasing comorbidity and odds of having symptomatic carotid atherosclerotic disease among persons with HIV, they appear consistent with a recent US-based cohort study of persons with HIV 26 showing that the prevalence of multi-morbidity (defined by the authors as two or more chronic conditions such as hypertension and type II diabetes mellitus) has tripled from 2000 to 2009. Even after controlling for age, the authors found a significant increase in multi-morbidity over time. Therefore, the trends we found are likely only partially attributable to increasing age at the time of intervention.
Our findings, together with the current literature, raise important questions regarding the risks and benefits of carotid interventions for persons with HIV with asymptomatic carotid stenosis. A Europe-based analysis 27 found that CEA is cost-effective for asymptomatic carotid artery stenosis compared to real-world adherence to best medical therapy for a base population of age 60 to 75. An important caveat is that cost-effectiveness is dependent on (1) the rate of perioperative mortality or disabling stroke, (2) the base stroke rate on medical therapy, and (3) the long-term rate of death or disabling stroke after CEA. Because there are currently no data on outcomes after carotid intervention in persons with HIV, and because persons with HIV still have shorter life expectancy than the general population, 25 we cannot assume that the risk and benefits for the general population are applicable to those with HIV infection. Other factors further complicate these calculations. One is the increasing comorbidity in persons with HIV that was previously discussed; this would factor into both background stroke rate as well as postoperative complication rate. Another is that, while persons with HIV are aging, and atherosclerosis is considered a disease of aging, there are studies to suggest that neither aging nor atherosclerotic disease offers a satisfactory explanation of why ischemic stroke is on the rise among persons with HIV.23,28–30 If that is the case, the benefit conferred by CEA or CAS, if any, may be less in persons with HIV than in the general population. Data in the form of randomized clinical trials or at least prospective studies are greatly needed to start to clarify the role of carotid intervention in persons with HIV with asymptomatic carotid disease.
The association of HIV with younger age at the time of carotid intervention and a trend towards greater likelihood of having symptomatic disease highlight two goals that can improve the health of persons with HIV infection: (1) to delay ischemic stroke or carotid intervention through primary and secondary prevention; and (2) to better identify those who would benefit most from carotid intervention in order to prevent symptoms or disability. With regards to the first goal, there are currently no specific predictive scores for persons with HIV and ischemic stroke that can guide statin use as primary prevention. The 2013 American College of Cardiology/American Heart Association recommendations, the 2004 Adult Treatment Panel III recommendations 31 as well as the Framingham Risk Score for Stroke 32 would all underestimate stroke risk or under-recommend statin use in persons with HIV infection. We look forward to the first results from REPRIEVE, a placebo-controlled trial examining pitavastatin for persons with HIV and its effects on major cardiovascular events, including stroke, as a start to more specific guidance. Meanwhile, continued and intensified efforts to partner with persons with HIV to reduce risks and promote healthy habits are direly needed. As for the second goal, the development of a scoring system that can stratify persons with HIV infection by ischemic stroke risk by taking into account traditional risk factors, carotid plaque features, and immunologic parameters would be a significant next step to informing medical therapy or decisions to recommend surgery. We also need data to show that the rationale for recommending against screening for carotid artery stenosis 33 is applicable to persons with HIV infection, in light of studies showing that well-controlled HIV patients with low Framingham Risk Scores have a high prevalence of subclinical carotid atherosclerosis, 34 and that carotid plaque is independently associated with stroke in otherwise healthy persons with HIV. 35
Study limitations and strengths
There are important limitations in this analysis. As an administrative and discharge-level database, important clinical information, such as CD4 count, viral load, ART treatment, other medical or non-medical treatments, lab values (e.g. lipid panel) or family history of cardiovascular disease, were not available. The use of ICD-9-CM codes to identify diagnosis or procedures can be prone to misclassification. Given that it is more likely that an admission is misclassified as being HIV–, rather than the converse, potential misclassification bias in HIV-status would bias results toward the null. Temporal relationships between ICD-9-CM diagnostic codes are not available in the NIS. Thus, there is a possibility that a patient who had suffered a remote stroke but is now undergoing CEA for an asymptomatic carotid lesion is misclassified as undergoing CEA for symptomatic disease in this analysis. Missing data were handled with multiple imputation, which has the potential to introduce bias, although this is less likely in our analysis for two reasons: (1) the most commonly missing variable, race, is most likely missing at random (MAR) as its missingness is dependent on specific hospital reporting policies 36 ; and (2) rates of missingness for other variables are quite low. Despite these limitations, we believe there are also significant strengths. The use of a large national sample with a sampling frame of > 95% of the US population allowed us to examine a rare exposure (HIV infection) and an uncommon endpoint (carotid intervention), and our analysis of data over an 11-year period also allowed us to visualize important trends.
Conclusion
The prevalence of HIV infection among those undergoing carotid intervention is growing. HIV infection is independently associated with younger age at the time of surgery, and trends show that there is increasing comorbidity and likelihood of having symptomatic carotid atherosclerotic disease in persons with HIV infection compared to the general population. Our findings highlight a need for better prevention or detection of carotid atherosclerosis in persons with HIV, and a deeper understanding of unique risks and benefits of carotid endarterectomy or carotid artery stenting in this population.
Supplemental Material
VMJ789783_Supplementary_Table_1 – Supplemental material for Association of HIV infection with age and symptomatic carotid atherosclerotic disease at the time of carotid intervention in the United States
Supplemental material, VMJ789783_Supplementary_Table_1 for Association of HIV infection with age and symptomatic carotid atherosclerotic disease at the time of carotid intervention in the United States by Timothy C Lin, Brittany N Burton, Andrew Barleben, Martin Hoenigl and Rodney A Gabriel in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by grants from the National Institutes of Health (grant numbers TL1TR001443 of the Clinical and Translational Science Award (CTSA) to TCL and BB; MH113477, AI106039 and AI036214 to MH).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.