
Abstract
Unruptured intracranial aneurysms often have a relatively benign clinical course. Frequently, they are found incidentally during workup for an underlying, possibly related or unrelated, symptom or condition. Overall, brain aneurysms are considered to have a relatively low annual risk of rupture. However, should it occur, aneurysmal subarachnoid hemorrhage can lead to significant morbidity and mortality. Our understanding of the natural history and treatment outcomes of cerebral aneurysms has significantly increased over the last few decades, but choosing the optimal management for each patient requires the careful consideration of numerous medical, clinical and anatomic factors. The purpose of this review is to help physicians and caregivers, who may participate in the diagnosis, counseling and triage of patients with brain aneurysms, understand the basic elements of decision making. We discuss natural history, risk factors, screening, presentation, diagnosis, and their implications on aneurysm management and long-term follow-up. We also provide an overview of the risks and benefits of currently available treatment options.
The University of Virginia School of Medicine designates this journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit™ per article. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Learners are expected to read this article along with any references and supporting material as appropriate, and complete the online post-test questions with an 80% pass rate to receive credit. Post-test questions are accessed through the Society for Vascular Medicine website (www.vascularmed.org/VMJ-CME). Please note that CME credits are only available to members of SVM with a journal subscription. This activity expires 2 years after the publication date, on June 1, 2020.
Heather Gornik has disclosed research support from AstraZeneca, intellectual property rights from Summit Doppler Systems, Inc., and intellectual property rights and stock/ownership from FlexLife Health (proceeds donated). Aditya Sharma has disclosed research support from National Institute of Health Sciences, AstraZeneca, Biomet Biologics, Portola Pharmaceuticals, and Pedra Technology. Valerie Clark has no financial affiliations to disclose.
Introduction
Brain aneurysms represent an abnormal dilatation on the arterial wall of the cerebral vessels. Aneurysms usually develop in a vessel segment, most often near a bifurcation point, with an underlying structural abnormality. There is a thin or a lack of tunica media, and often times no or fragmented internal elastic lamina in the vessel wall. The tunica adventitia is present, sometimes with associated fibrinous material. They are a heterogeneous group of lesions with the most common (about 90% of all aneurysms) being saccular or berry aneurysms. Other types include fusiform (involving a longer vessel segment), traumatic, mycotic (related to an underlying infectious process), dissecting, and microaneurysms (usually seen on small perforator vessels due to chronic hypertension). Approximately 85% of aneurysms are located in the anterior circulation of the circle of Willis. 1 Aneurysms represent a significant health concern, predominantly because of significant morbidity and mortality associated with rupture and subarachnoid hemorrhage (SAH).
Demographics
Aneurysms are most prevalent between the ages of 35 and 60 years. The female to male ratio is 3:2, but before age 40, males and females equally affected. Approximately 10–30% of patients can have multiple aneurysms. 1 Approximately six million people (or 1 in 50) in the United States are affected. The mean overall unruptured aneurysm prevalence is estimated to be about 2.8% (95% CI: 2.0–3.9%) in the entire population. 2
Approximately 3-5% of new strokes are due to aneurysm rupture related subarachnoid hemorrhage (SAH). On average, only approximately 0.25% of aneurysms are thought to end up in rupture. Still, approximately 500,000 people die in the world annually due to ruptured aneurysms. 3 The incidence varies between 2.0 and 22.5 cases per 100,000 population in the world, 4 with the highest numbers seen in certain populations (e.g. Finland and Japan). The incidence gradually increases each decade, and peaks in the sixth decade. 5
Risk factors for aneurysm formation
Several risk factors have been associated with aneurysm development, growth and rupture (Table 1). Genetic contribution to aneurysm development is strongly supported by studies through multiple pathophysiologic pathways mainly relating to vascular endothelial maintenance. However, the relationship of genetic variants to aneurysm size, rupture risk and location still need large cohort studies. 6 Hereditary syndromes or high risk conditions (Table 2) should be considered when there are more than one family member harboring intracranial aneurysms. The pathophysiology of intracranial aneurysm formation in most of these inherited syndromes stems from the weakness in the arterial wall connective tissue. The prevalence of incidental intracranial aneurysms in first-degree members of families with familial aneurysms has ranged from 4% to 9% depending on study population, but this is higher than in the general population.7,8 In addition, aneurysms in first-degree relatives tend to rupture at a smaller size and younger ages compared to patients with sporadic aneurysms. 9 Cigarette smoking and hypertension are independent risk factors for intracranial aneurysms, with an odds ratio of 3.0 and 2.9, respectively, and combined have an odds ratio of 8.3. 10 Similarly, individuals who both smoked and had hypertension have a 15-fold increased risk of subarachnoid hemorrhage. 11 There is some evidence that regular physical exercise and hypercholesterolemia (likely due to treatment with HMG-coenzyme inhibitor therapy) may be protective with regards to intracranial aneurysm formation. 10 The higher prevalence of subarachnoid hemorrhage in post-menopausal women compared with pre-menopausal women, along with the reduction in risk with the use of hormone replacement therapy in post-menopausal women in earlier studies was suggestive that estrogen deficiency might play a role in development of intracranial aneurysms.12,13 However, a more recent analysis suggested that hormone replacement therapy in post-menopausal women might actually increase the risk of SAH. 14 There may be higher prevalence of intracranial aneurysms in individuals with aortic aneurysms 15 and coarctation of the aorta. 16 As mentioned earlier, certain geographic areas and populations appear to have a higher incidence and prevalence than others (e.g. Japan and Finland).
Potential risk factors for aneurysm growth and rupture.
Genetic and other medical conditions associated with intracranial aneurysms.
Clinical presentation
Intracranial aneurysms can be incidentally found, or may be associated with clinical symptoms (Table 3). An estimated 10-15% of unruptured aneurysms are symptomatic. 17 In the International Study of Unruptured Intracranial Aneurysms (ISUIA) trial, the diagnosis of the target unruptured aneurysm was made during evaluation of hemorrhage from another aneurysm (30.4%), headache (23.7%), ischemic cerebrovascular disease or transient ischemic attack (10.6% and 10.5%, respectively), cranial nerve palsy (8.0%), seizures (2.9%), symptoms of mass effect (2.7%), subdural or intracerebral hemorrhage (1.2%), brain tumor (0.8%), central nervous system degenerative disorders (0.4%), and undefined ‘spells’ (7.1%). 18 Symptomatic unruptured intracranial aneurysms are mainly diagnosed due to mass effect (large size), and can present with headaches, cranial neuropathy, seizures, visual disturbances, pyramidal tract signs and facial pain. 17 Extradural aneurysms, if symptomatic, may also cause symptoms due to mass effect; if they do rupture, they may lead to epistaxis or local hematoma, but rarely present as subarachnoid hemorrhage. The most feared clinical presentation of intracranial aneurysms is subarachnoid hemorrhage. Often the rupture is spontaneous, but trigger factors may include activities associated with a sudden increase in blood pressure, such as nose-blowing, sexual activity, defecation, vigorous physical exercise, and anger/emotional outbursts. 19 Headaches account for 4.5% of emergency room (ER) visits, 20 and about 2-3% of these have SAH. 21 Sentinel headache, a severe head pain occurring days to weeks before aneurysm rupture, may be seen in 10-43% of subarachnoid hemorrhage patients in some series, 22 and may carry a higher risk of rerupture. 23 Abrupt loss of consciousness may also raise suspicion of sentinel hemorrhage or frank aneurysm rupture. Misdiagnosis of SAH remains common, especially in ‘good grade’ (Hunt and Hess grades I and II: headache, nuchal rigidity, and no neurologic deficit other than possible cranial nerve palsy) patients. Misdiagnosis may result in worsening of the condition, often from rebleeding, before definitive treatment can be performed.
Clinical presentation of unruptured intracranial aneurysms (based on the ISUIA trial 18 ).
Diagnosis and imaging
Most intracranial aneurysms are found incidentally, during screening, due to subarachnoid hemorrhage, or during workup for associated symptoms.
A reliable and simple diagnostic test for ruptured aneurysms is non-contrast head computed tomography (CT), which is positive in 98-100% of cases for up to 12 hours after onset, and is positive in 93% of cases in the first 24 hours. Positive results decrease with time. 24 When the initial head CT is negative, but strong clinical suspicion exists, certain magnetic resonance imaging (MRI) sequences (FLAIR, SWI, GRE) may be sensitive enough to show even small amounts of subarachnoid blood. If definitive imaging findings are lacking, the gold standard for detection remains lumbar puncture, although ‘traumatic tap’ may occur in up to 20% of cases. Released hemoglobin from red blood cells metabolizes to pigmented molecular oxyhemoglobin and bilirubin, resulting in xanthochromia. Oxyhemoglobin can be detected within hours. The formation of bilirubin, an enzyme-dependent process, is diagnostically more reliable, but may require up to 12 hours to occur.
CT angiography (CTA) is a widely used modality for imaging and screening for intracranial aneurysms. Based on meta-analysis, the sensitivity of CTA ranged from 53% (95% confidence interval (CI): 44-62%) for 2 mm aneurysms to 95% (95% CI: 92-97%) for 7 mm aneurysms, while the overall specificity was 98.9% (95% CI: 91.5-99.99%). 25 With a small pretest probability, the positive likelihood ratio for unruptured aneurysms ranged from 15 for 2 mm aneurysms to 61 for 5 mm aneurysms. The positive likelihood ratio for ruptured aneurysms with an intermediate pretest probability (50%) ranged from 3.9 to 56 for 2 to 5 mm aneurysms. 25
MRI angiogram (MRA) is another useful modality; however, the sensitivity for smaller aneurysms (< 3 mm) is lower. Pooled sensitivity of MRA was 95% (95% CI: 89-98%), and pooled specificity was 89% (95% CI: 80-95%). False-negative and false-positive aneurysms detected on MRA were mainly located at the skull base and middle cerebral artery. Freehand three-dimensional (3D) reconstructions performed by the radiologist significantly increased diagnostic performance. 26 However, MRI and CT do provide additional information about the brain tissue and adjacent structures in relationship to the aneurysm. There are data to support that MRIs may be useful in follow-up studies post treatment. 27
Digital subtraction angiography (DSA) remains the gold standard imaging modality for intracranial aneurysms. Using techniques like 3D rotation, small aneurysms can be identified. 28 Another advantage of DSA is morphological assessment of the aneurysms and relationship of small branches and perforators near the aneurysms. DSA may also help distinguish between true infundibula and aneurysms. DSA does have some, albeit very small, risk with the procedure, including ischemic stroke, dissection, bleeding, and radiation side effects. 29
Screening
Screening for intracranial aneurysms must be tailored to specific populations in order to be cost effective and beneficial. Potential risks of the screening test would also have to be considered, such as radiation and contrast use with CTA. In a mathematical screening model, screening resulted in a quality adjusted life year (QALY) loss, which equated to a negative clinical impact. The threshold for 5-year risk of rupture at which screening resulted in a gain in QALYs was 13%. This held true for any prevalence of aneurysms between 1% and 25%. The risk of rupture had a greater impact on outcome than prevalence. Halving the risk of intervention (either surgery or coiling) reduced the threshold 5-year risk of rupture at which screening resulted in gain of QALYs to 6%. This study was suggestive that non-invasive screening for intracranial aneurysms is beneficial only in populations with a higher than normal expected prevalence and risk of rupture. 30 Current guidelines do not support widespread screening for intracranial aneurysms in the general population, 31 but they do recommend the use of CTA/MRA screening for intracranial aneurysms in individuals with two or more family members with intracranial aneurysms or subarachnoid hemorrhage. In addition, for patients with a history of autosomal dominant polycystic kidney disease, fibromuscular dysplasia (FMD), aortic aneurysms, coarctation of the aorta and microcephalic osteodysplastic primordial dwarfism, particularly those with a positive family history, it is reasonable to offer screening.15,31,32
Aneurysm management options and decision-making
Aneurysm treatment options
Aneurysm clipping, which was first reported by Walter Dandy in 1938, 33 remains a reliable and efficient way of treating cerebral aneurysms. Endovascular coiling (Figures 1A and 1B) was first reported in 1990 and 1991.34–36 The first self-expandable neuro-specific intracranial stents became available in the early 2000s, followed by several others later on (Figures 2A and 2B). Flow diverter therapy (Figure 3 and Figures 4A and 4B) first appeared around the mid-2000s for investigational use, and has become widely popular after the initial safety and feasibility trials were completed. Since then, upgraded versions of previously available coils, stents, balloons, flow diverters, as well as many other new adjunctive intra- and extraluminal devices, have been developed for the treatment of intracranial aneurysms. 37
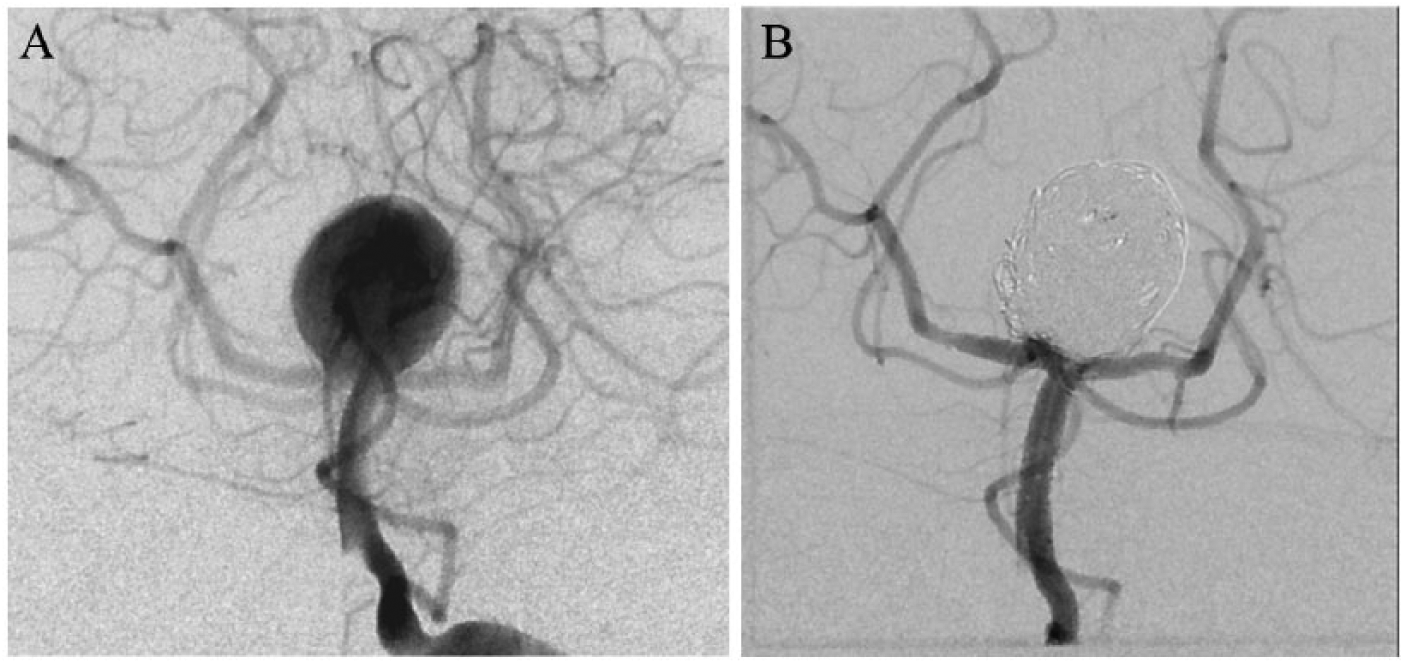
DSA images of a ruptured giant basilar apex aneurysm before (A) and after (B) coil embolization, demonstrating complete aneurysm occlusion.DSA, digital subtraction angiography.
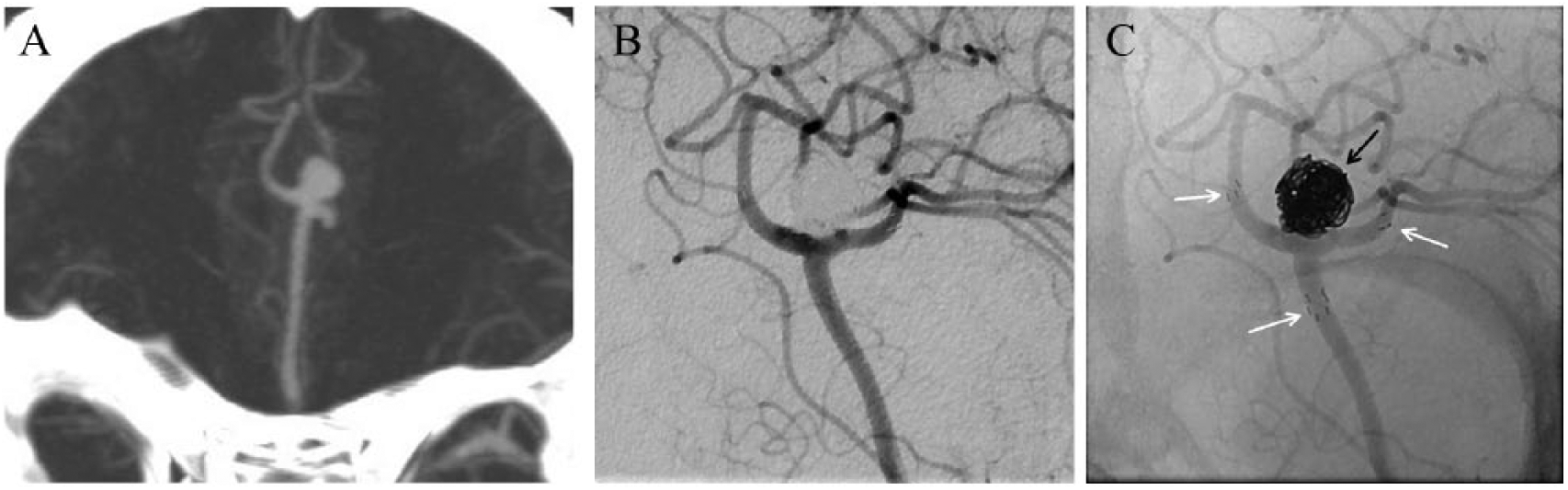
(A) Saccular aneurysm at the A2/A3 segment bifurcation of an azygos ACA on CTA. (B) DSA images after successful Y-stent-assisted coil embolization of the aneurysm without residual filling. (C) Unsubtracted DSA images demonstrate the large coil mass (black arrow), and the proximal and distal stent tines in the parent vessels (white arrows).
Photograph of 2 Pipeline flow diverter embolization devices (Medtronic, Irvine, CA, USA).
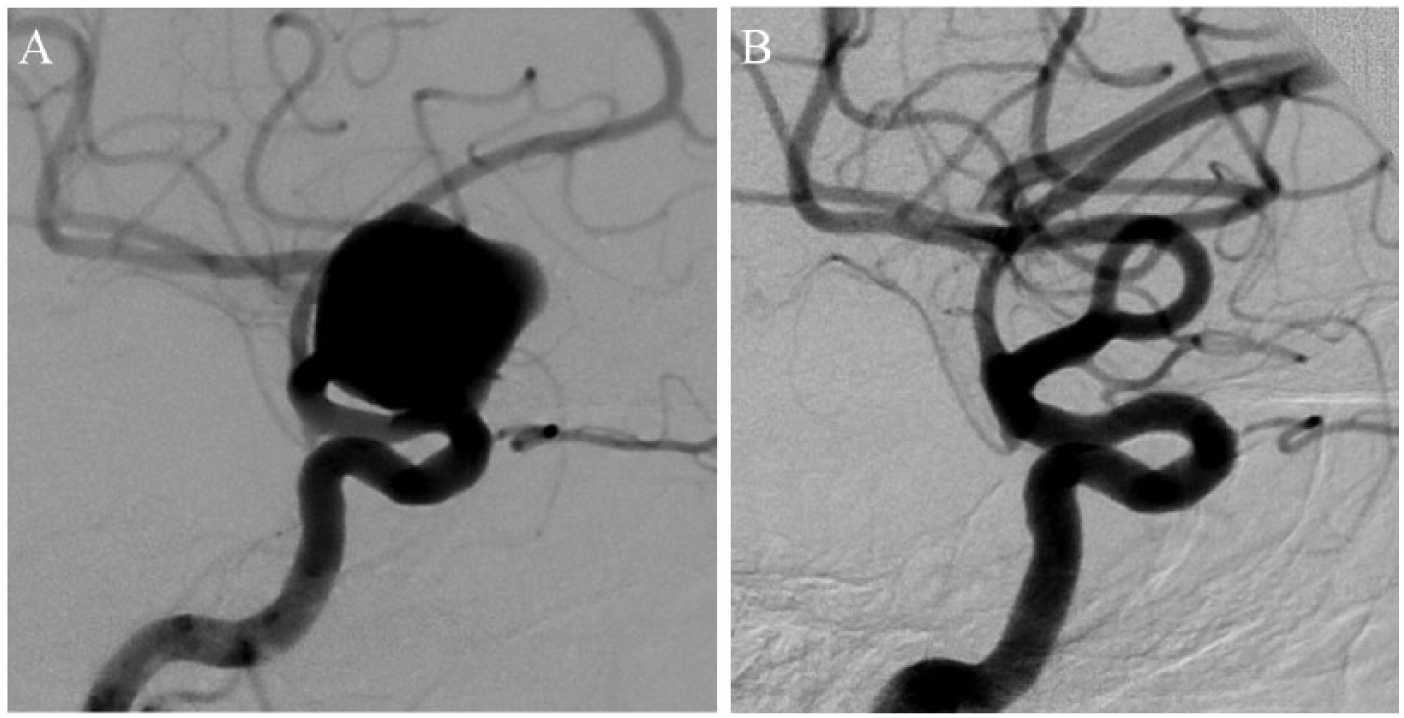
DSA images of an unruptured giant aneurysm off the ophthalmic segment of ICA before (A) and 1 year after (B) flow diverter treatment, showing complete aneurysm occlusion.
Unruptured cerebral aneurysms
Aneurysm growth and rupture
Several large studies have looked at the natural history of unruptured intracranial aneurysms (Table 4).18,38–40 One of the largest aneurysm trials remains the International Study of Unruptured Intracranial Aneurysms (ISUIA), which included two patient groups depending on no prior SAH (group 1) versus prior SAH from a different aneurysm (group 2). The first part of this trial, published in 1998, 38 included 2621 patients and had a retrospective (1449 patients) and prospective (1172 patients) arm. The retrospective arm analyzed natural outcomes, whereas the prospective arm studied treatment related morbidity and mortality. There were 32 ruptures (1.2%) over the 8.3 years of mean follow-up, and 28 ruptures occurred within 7.5 years of follow-up. Posterior circulation location carried an elevated risk of rupture in both groups. In the group with no prior SAH, larger aneurysm (> 10 mm) size was also a significant predictor of rupture, but not in group 2. On the other hand, in group 2, older patients had a slightly elevated rupture risk, which was not seen in group 1. Aneurysms of less than 10 mm in diameter were 11 times more likely to rupture if there was a prior SAH versus not.
Natural history of unruptured aneurysms in large clinical studies (see details in text).
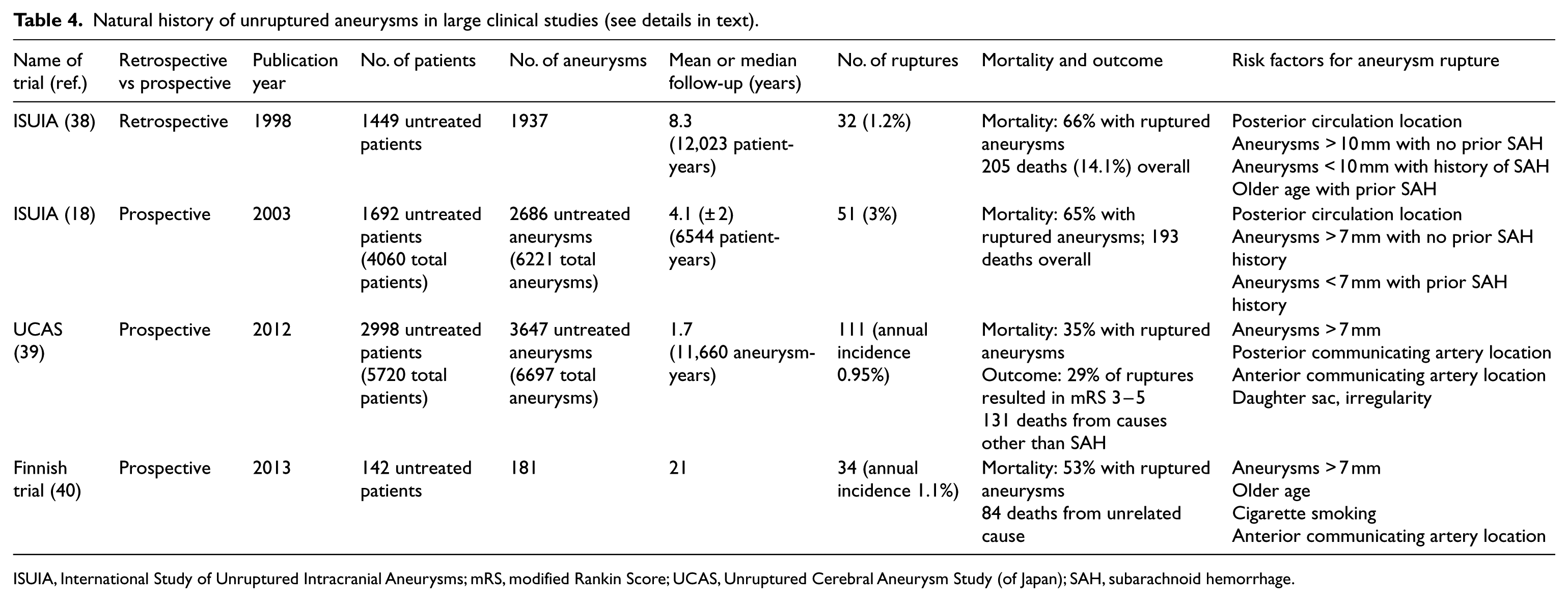
ISUIA, International Study of Unruptured Intracranial Aneurysms; mRS, modified Rankin Score; UCAS, Unruptured Cerebral Aneurysm Study (of Japan); SAH, subarachnoid hemorrhage.
The second, prospective part of the ISUIA trial was published in 2003 18 with 4060 patients, and a mean follow-up of 4.1 ± 2 years. In the untreated arm (1692 patients), only 3% of patients had a rupture during the follow-up period, and almost all of them within 5 years. Posterior circulation location was a predictor of rupture in both groups, while larger aneurysm size only in group 1, but the number of large aneurysms in group 2 was small. Patients with prior SAH had a higher risk of aneurysm rupture if the size was less than 7 mm, but this difference was not seen for larger aneurysms between groups 1 and 2. The Unruptured Cerebral Aneurysm Study (UCAS) from Japan, conducted between 2001 and 2004, enrolled 5720 patients with 6697 unruptured > 3 mm aneurysms, 91% incidentally discovered. 39 Surgical repair was done in 2722 patients with 3050 aneurysms before rupture. There were 111 ruptures over the mean follow-up of 1.7 years, resulting in an annual rupture rate of 0.95%. Factors that were found to be associated with rupture included daughter sac, larger size, and posterior communicating artery and anterior communicating artery location.
In the Finnish aneurysm study by Juvela et al., only 142 patients with 181 unruptured aneurysms were enrolled, with multiple aneurysms in 23% of patients. 40 However, the median follow-up was one of the longest at 21 (range 0.8-52.3) years. The follow-up was until death, SAH event, or the year 2011–2012, whichever was the latest. Aneurysm rupture rates decreased with very long-term follow-up, with no aneurysm rupture after 25 years. There was a total of 34 (24%) aneurysm ruptures, and 18 (53%) patients with SAH died. The annual incidence was 1.1%. This study found that cigarette smoking (adjusted hazard ratio (HR) 2.44; 95% CI: 1.02-5.88), location of the aneurysm in the anterior communicating artery (HR 3.73; 95% CI: 1.23-11.36), patient age inversely (HR 0.96 per year; 95% CI: 0.92-1.00), and aneurysm diameter ≥ 7 mm (HR 2.60; 95% CI: 1.13-5.98) independently predicted subsequent aneurysm rupture.
Despite numerous studies showing a definitive correlation between larger aneurysm size and rupture risk, there is evidence that aneurysms smaller than 10 mm do rupture. 41 One possibility is the presence of aneurysmal irregularity or daughter sac, which was shown to be a risk factor in the UCAS trial mentioned above. This suggests that there may be other factors playing a role in the risk of rupture (HR 1.63; 95% CI: 1.08-2.48). 39 In addition, familial intracranial aneurysms had an almost 17 times higher risk of rupture compared to matched size and location in the ISUIA trial. 9
Not surprisingly, the risk factors associated with aneurysm growth are similar to the risks associated with rupture, and aneurysm growth itself has been associated with risk of rupture as well.42,43 Other potential risk factors for aneurysm growth and rupture include aneurysm morphology and aspect ratios.44,45 There has been an increasing interest in newer radiological imaging techniques to study aneurysmal wall inflammation, and the use of computational flow dynamic studies to identify wall shear stress, which may also aid in understanding the characteristics that lead to aneurysm rupture.45-48
Unruptured aneurysms: treatment and outcomes
The decision making for unruptured aneurysm treatment is usually more complex, and has to be tailored to the individual patient based on multiple factors. It involves careful consideration and interpretation of the clinical history and presentation, sex, individual risk factors, medical comorbidities, imaging studies, prior subarachnoid hemorrhage, aneurysm size and location, vessel anatomy, family history, genetic conditions, and the natural history of cerebral aneurysms.
In the prospective treatment arm (1172 patients, 1301 aneurysms) of the first ISUIA trial, 38 surgical morbidity and mortality in group 1 (no prior SAH) was 17.5% at 30 days and 15.7% at 1 year; in group 2 (prior SAH) it was 13.6% at 30 days and 13.1% at 1 year. Older age was a predictor of poor surgical outcome. Endovascular treatment was underrepresented in this study with open surgery comprising 83% of group 1 and 94% of group 2.
Endovascular therapy comprised only 19% of all aneurysm treatments in the second, prospective part of the ISUIA trial, published in 2003. 18 The rates of morbidity and mortality at 1 year in group 1 were 12.6% and 9.8% for those treated with clipping and coiling, respectively. In group 2, these rates for surgery and endovascular therapy were 10.1% and 7.1%, respectively. Older age, large aneurysm size (> 12 mm), and posterior circulation location appeared to predict worse surgical and endovascular outcome.
A large systemic review and meta-analysis of 71 endovascular trials included 5044 patients with 5771 unruptured aneurysms that were treated, and found 1.2% mortality and 4.8% unfavorable outcomes, including death. 1 Periprocedural complication reports were available in 3699 patients, and demonstrated thromboembolism in 7.6%, perforation or rupture in 2.6%, and device related problems in 3.0%, resulting in unfavorable outcomes in 4.3% and death in 1.9%. Crude data analysis showed that patients with an unfavorable outcome were older. Immediate complete aneurysm occlusion or only a neck remnant was achieved in 86.1%. Mean follow-up angiography ranging from 0.4 to 3.2 years in 1521 patients showed an overall recanalization rate of 24.4%. A retreatment rate of 9.1% was calculated in 1699 available patients. Mean clinical follow-up, ranging from 0.3 to 3.7 years, was available for 2013 patients with an annual bleeding risk of 0.2%.
Microsurgical clipping for unruptured aneurysms in another meta-analysis showed a low 1.7% mortality and 6.7% overall morbidity. 49
Several scoring systems have also been developed to aid the decision making process for unruptured aneurysms. Examples include the unruptured intracranial aneurysm treatment score (UIATS), which accounts for 29 key factors, and the PHASES (population, hypertension, age, size of aneurysm, earlier subarachnoid hemorrhage from another aneurysm, site of aneurysm) score.42,50
Unruptured aneurysms: medical management and other considerations
There are no prospective blood pressure control studies to show prevention of aneurysm development. However, in a Finnish study, patients with incidental unruptured aneurysms had more frequent antihypertensive medication use than the ruptured aneurysm group. 51 Smoking has been associated with aneurysm rupture.39,52 Further studies about the correlation between modifiable risk factors, such as hypertension and smoking, and aneurysm rupture are also described in the ‘Risk factors’ and ‘Aneurysm growth’ sections of this paper, and emphasize the importance of counseling patients about lifestyle modifications, smoking cessation, and blood pressure control.
Data regarding the use of aspirin for unruptured intracranial aneurysms is sparse and conflicting. An initial study found an increased risk of subarachnoid hemorrhage in women using aspirin. 53 A subset study of the ISUIA population found that patients who used aspirin three times weekly to daily had significantly lower odds of hemorrhage (adjusted OR, 0.27; 95% CI: 0.11-0.67; p = 0.03) compared with those who never took aspirin. 54 Subsequently, a preliminary study showed that aspirin was successful in reducing aneurysm wall inflammation, measured through surrogate imaging markers, which may contribute to this protective phenomenon. 55 With regards to severity of subarachnoid hemorrhage on current aspirin use, no significant worsening of outcomes was seen. 56 There are no large studies looking at the safety of concurrent use of anticoagulation and unruptured aneurysms. In a study, patients on anticoagulants were more often comatose on admission; however, the frequency of rebleeding, secondary ischemia, and hydrocephalus were not higher. In the stratified analysis, worse outcomes in the anticoagulant group were not influenced by differences in sex, age, cardiovascular history, site of aneurysm, amount of cisternal blood, or extension of hemorrhage into the ventricles. 57
Ruptured intracranial aneurysms
The initial decision making for aneurysms presenting with rupture and subarachnoid hemorrhage is well established: to avoid a dreaded rerupture, the aneurysm has to be secured. Aneurysm rerupture is a significant, often lethal complication with 4–13.6% occurring within 24 hours; about half of these occur within 6 hours of symptom onset. The risk remains about 1.5% per day for up to 2 weeks (~20% total), and about 50% by 6 months without treatment. Re-hemorrhage carries a 50-85% risk of mortality. 58 Microsurgical and endovascular modalities for the treatment of ruptured aneurysms have been compared in large trials (Table 5).
Milestone aneurysm treatment trials (see details in text).
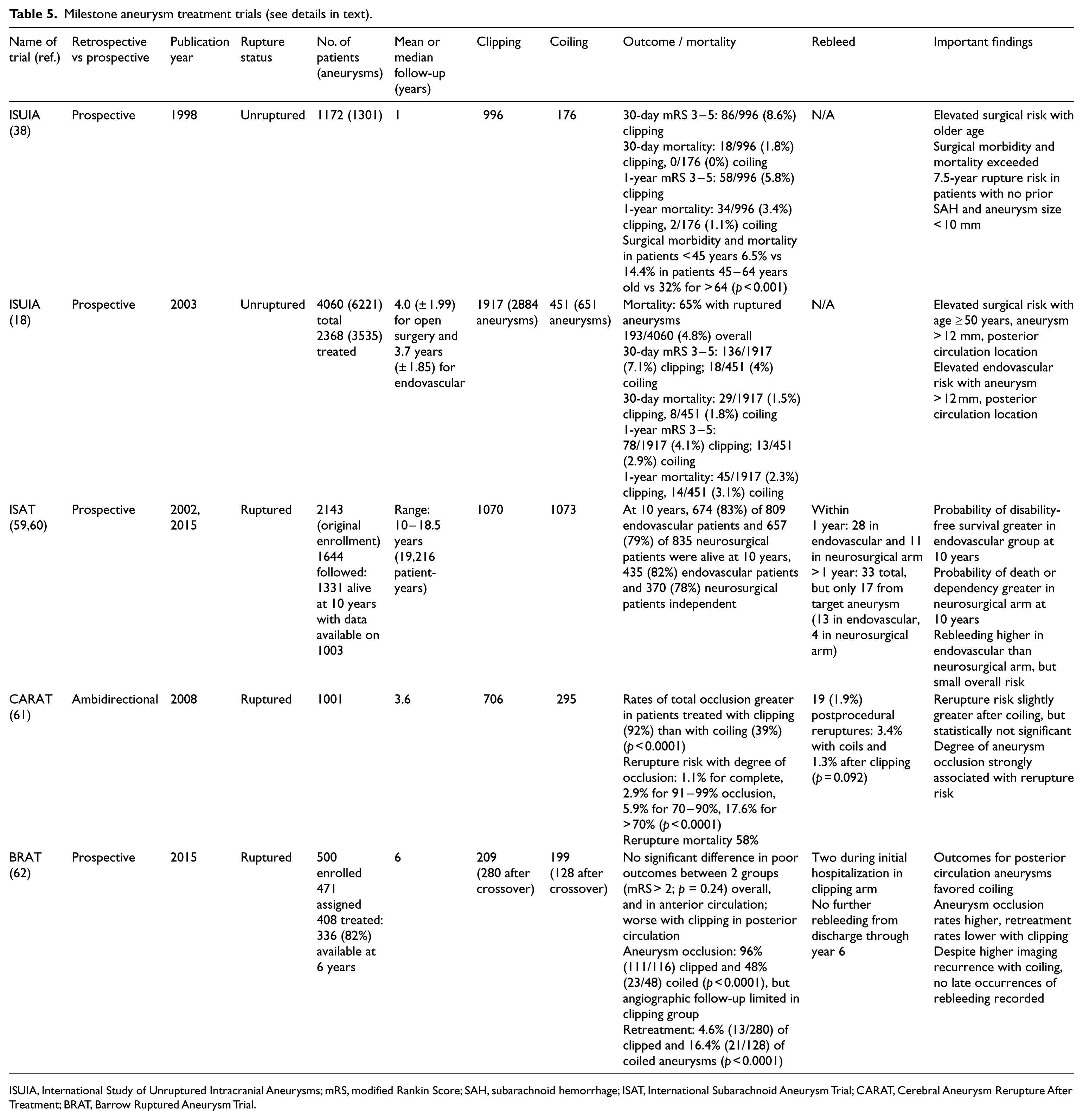
ISUIA, International Study of Unruptured Intracranial Aneurysms; mRS, modified Rankin Score; SAH, subarachnoid hemorrhage; ISAT, International Subarachnoid Aneurysm Trial; CARAT, Cerebral Aneurysm Rerupture After Treatment; BRAT, Barrow Ruptured Aneurysm Trial.
The International Subarachnoid Aneurysm Trial (ISAT) was a prospective, randomized, controlled trial, comparing surgical clipping against endovascular coiling for ruptured aneurysms, with 2143 patients enrolled between 1994 and 2002 in 43 centers. 59 Of the surgically (1070) and endovascularly (1073) treated patients, follow-up was available in 2118 patients at 1 year. Slightly more patients in the endovascular arm had better clinical outcomes. Less complete occlusion was seen with endovascular therapy, but angiograms were completed in only less than half of surgical patients. A higher risk of rebleeding was seen with endovascular therapy at 1 year, but the overall numbers were very low. In the final ISAT publication in 2015, 60 with a follow-up range of 10–18.5 years, endovascular patients were more likely to be alive and independent at 10 years (OR 1.34, 95% CI: 1.07–1.67). Rebleeding more than 1 year after the initial hemorrhage remained very low, seen in only 33 patients, 17 from the target aneurysm: 13 in the endovascular group and four in the neurosurgical group.
The Cerebral Aneurysm Rerupture After Treatment (CARAT) ambidirectional cohort study included 1001 patients from nine high volume centers, 61 who were either coiled (295) or clipped (706) over a mean follow-up of 4 years. There were 19 (1.9%) postprocedural reruptures: 3.4% with coils and 1.3% after clipping. The degree of aneurysm occlusion was strongly associated with the risk of rerupture (overall risk: 1.1% for complete occlusion, 2.9% for 91–99% occlusion, 5.9% for 70–90%, 17.6% for < 70%; p < 0.0001). The overall risk of rerupture was slightly greater after coil embolization, but statistically not significant between the two groups (3.4% vs 1.3%; p = 0.092). This slight difference did not persist after adjustment for confounders (HR 1.09; 95% CI: 0.32–3.69; p = 0.83).
The Barrow Ruptured Aneurysm Trial (BRAT), a randomized trial, included 408 patients with SAH from ruptured aneurysms: 209 (280 after crossover) in the surgical clipping arm versus 199 (128 after crossover) in the endovascular coiling arm, and 82% of patients had a 6-year follow-up. 62 The investigators found no significant difference in poor outcomes between the two groups (mRS > 2; p = 0.24) overall and in the anterior circulation, but outcomes for posterior circulation aneurysms favored coiling. Complete aneurysm obliteration at 6 years was seen in 96% (111/116) of clipping versus 48% (23/48) of coiling patients (p < 0.0001), but the availability of follow-up angiogram was limited in the clipping group. Retreatment was required in 4.6% (13/280) of clipping versus 16.4% (21/128) of coiling patients (p < 0.0001). Despite higher imaging recurrence with coil embolization, however, other than two early reruptures in an incompletely clipped and another wrapped dissecting aneurysm, no late occurrences of rebleeding were recorded.
Ultimately, the optimal treatment for aneurysmal SAH depends on the open surgical and endovascular expertise of the treating institution, aneurysm location, admission SAH grade, potential early vasospasm, and the presence of any associated space occupying hematoma, which may need concurrent surgical evacuation.
Ruptured aneurysms: vasospasm, medical management, and other considerations
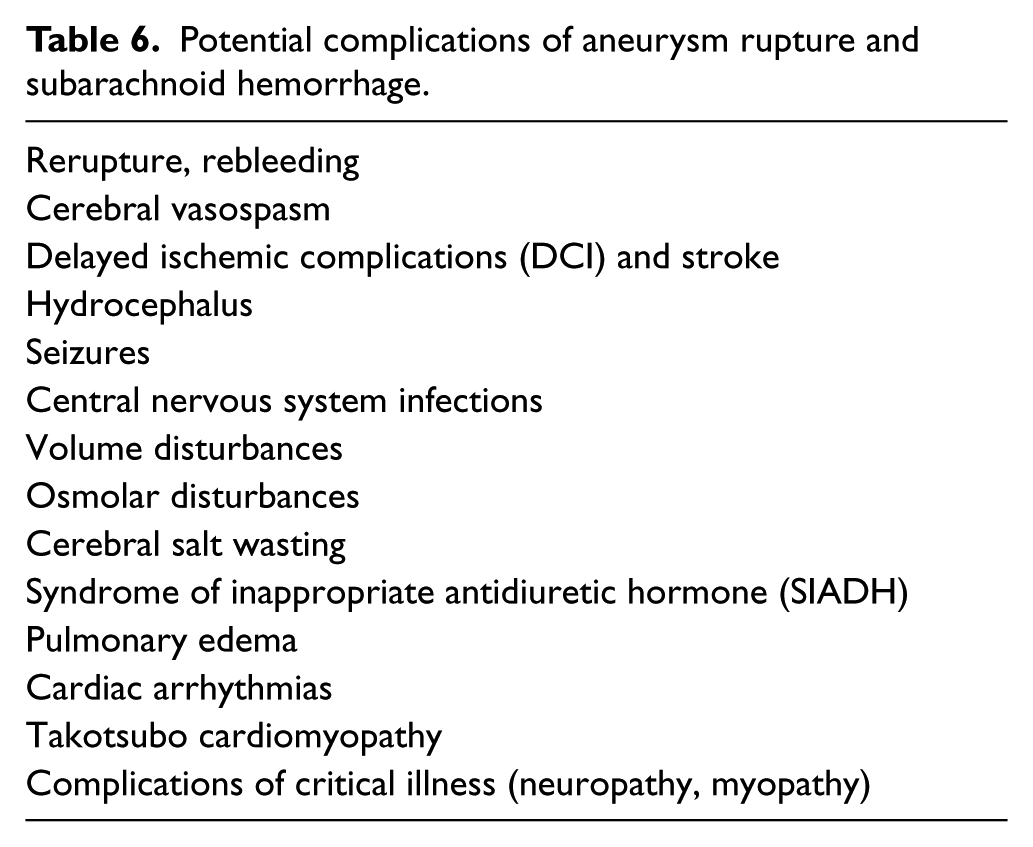
Vasospasm, or angiographically visible narrowing of the cerebral arteries, is a common complication after subarachnoid hemorrhage, which is seen in up to 40–70% of patients. It peaks approximately 7–10 days after aneurysm rupture, and usually resolves by 21 days. It is thought to be possibly related to oxyhemoglobin coming into contact with the vessel walls. 63 Vasospasm can be symptomatic or asymptomatic, and may lead to delayed ischemic complications (DCI), including stroke. 64 Treatment with the calcium channel blocker nimodipine has been shown to improve neurologic outcome, but does not reduce angiographic vessel narrowing and mortality. 65 Current guidelines recommend maintaining euvolemia and transcranial Doppler monitoring for vasospasm in patients with SAH. Induced hypertension (if cardiac status safely allows), and possible cerebral angioplasty and/or intra-arterial vasodilator therapy, may be considered for patients with vasospasm at high risk for DCI, and not readily responding to medical treatment. 66 Other possible, and often severe, complications of SAH include cardiac arrhythmias, pulmonary edema, hydrocephalus, seizures, and several others, as listed in Table 6.
Potential complications of aneurysm rupture and subarachnoid hemorrhage.
Aneurysm studies with adjunctive therapy and newer devices
A recent meta-analysis of 14 studies comparing 2698 conventional stent-assisted coiling and 29,388 coiling-only patients found that the immediate occlusion rate for stent-assisted coiling was 57.7% (range: 20.2–89.2%) versus 48.7% (range: 31.7–89.2%) for coiling-only, with no statistically significant difference between the two (OR 1.01; 95% CI: 0.68–1.49). However, progressive thrombosis was significantly more likely in stent-assisted coiling (29.9%) versus coiling-only (17.5%) (OR 2.71; 95% CI: 1.95–3.75). Aneurysm recurrence was significantly lower in stent-assisted coiling (12.7%) versus coiling-only (27.9%) (OR 0.43; 95% CI: 0.28–0.66). There was no significant difference between the two techniques for all complications, permanent complications or thrombotic complications. Mortality was higher in the stent-assisted group (1.4%; range: 0–27.5%) versus the coiling-only group (0.2%; range: 0–19.7%) (OR 2.16; 95% CI: 1.33–3.52), but remained overall very low in both groups. 67
The Pipeline for Uncoilable or Failed Aneurysms (PUFS) trial was a multicenter, prospective, single-arm interventional trial of the Pipeline flow diverter device (Medtronic, Irvine, CA, USA) for uncoilable or failed aneurysms of the internal carotid artery. 68 Of the 108 patients with 110 aneurysms enrolled, 109 aneurysms in 107 patients were treated. The primary effectiveness endpoint of the study was complete occlusion of the aneurysm without major (> 50%) stenosis of the parent artery or adjunctive use of complimentary embolic agent as seen on 6-month angiography, which was reached in 73.6% of patients. Aneurysm occlusion for those patients with angiographic follow-up progressively increased over time to 86.8% (79/91), 93.4% (71/76), and 95.2% (60/63) at 1, 3, and 5 years after treatment, respectively. Six aneurysms (5.7%) were retreated. The primary safety endpoint of major ipsilateral stroke or neurological death within 6 months was reached in six patients. There were four (3.7%) deaths. No delayed neurological deaths or cerebrovascular events were reported beyond 6 months. Seventy-eight (96.3%) of 81 patients with 5-year clinical follow-up had a modified Rankin Scale score of ≤ 2. Importantly, no recanalization of a previously occluded aneurysm was observed. The PUFS and other studies reported no significant long-term in-stent stenosis with the device. 69
Flow diverter use in the posterior circulation remains controversial, although more data has become available in recent years. Unfavorable results have been seen, especially with long fusiform aneurysms affecting the entire basilar segment. 70 However, in cases of posterior circulation dissecting aneurysms, sidewall aneurysms, and saccular aneurysms, results have been more promising. 71
Lessons learned from aneurysm studies: management options and decision-making
Observation and conservative management with vascular risk factor control (e.g. smoking cessation, blood pressure lowering) may be a reasonable option for many unruptured aneurysms, especially in patients with smaller aneurysms without high risk features (Table 4) and no family history. If aneurysm treatment is considered, the efficacy, safety and feasibility of surgical and endovascular modalities have been well established (Table 5). Slightly lower morbidity and mortality rates were seen with endovascular therapy for unruptured aneurysms. Endovascular coiling appeared to have lower procedural morbidity, mortality and greater disability-free survival, but a higher risk of recurrence than surgical clipping in early trials for ruptured aneurysms. Despite more recurrent aneurysms with endovascular treatment, however, the incidence of rebleeding was still very small. The degree of aneurysm occlusion appeared to be a predictor of rerupture. Later studies found that adjunctive methods (e.g. balloons and stents), or newer devices (e.g. flow diverters) may further improve the efficacy of endovascular therapy, and may reduce the recurrence rate that was seen with primary coiling. In high volume centers with both endovascular and open surgical capabilities, the risks, benefits, efficacy, and recurrence rates of all available treatment modalities should be reviewed with the patient and family.
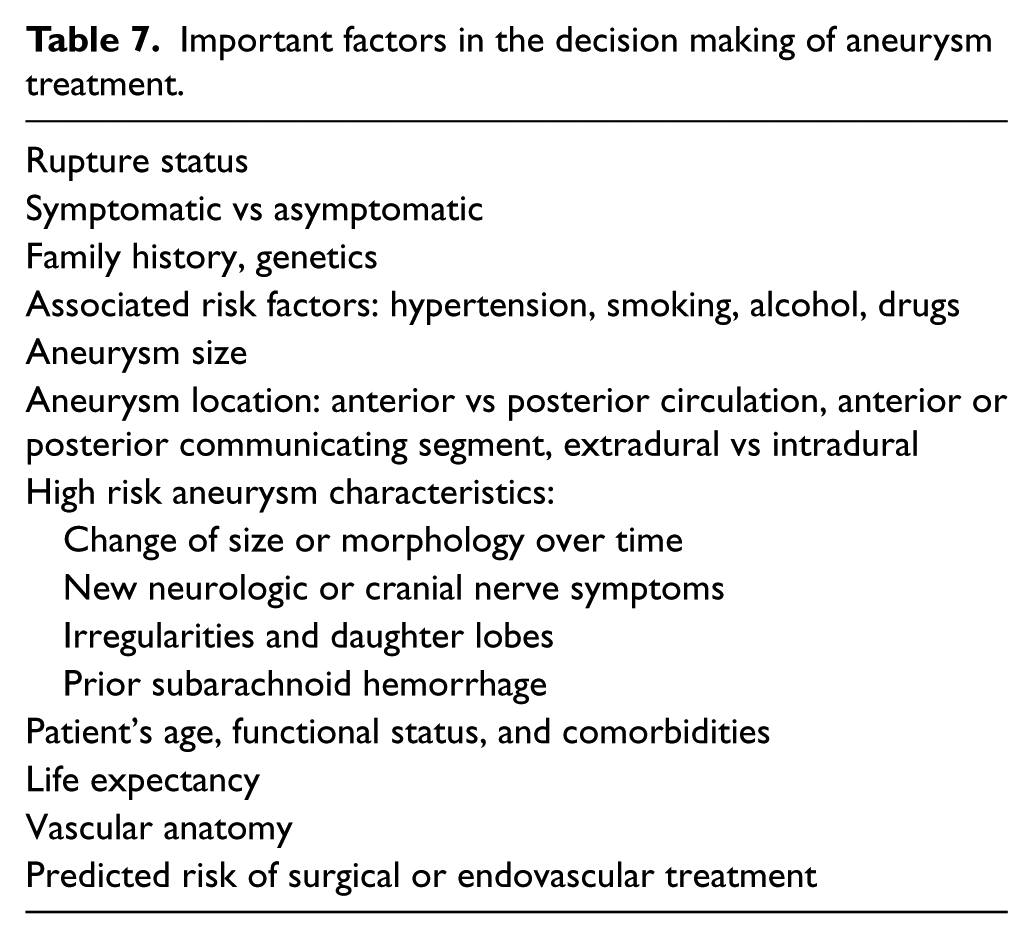
In most large institutions, for patients with poorer SAH grade, older age, and/or posterior circulation (especially basilar apex) location, endovascular therapy is favored. Middle cerebral artery aneurysms, large concomitant hematomas, and younger age may prompt the consideration of surgical clipping. The most important factors in the decision making of aneurysm treatment are summarized in Table 7.
Important factors in the decision making of aneurysm treatment.
Aneurysm follow-up
The modality, timing and duration of follow-up for previously treated, ruptured, and unruptured aneurysms are not standardized.31,66 Non-invasive studies are preferred by most institutions for surveillance and screening. DSA remains the gold standard for both endovascular and neurosurgical planning purposes if (re)treatment becomes necessary. Artifact from prior coils, clips, or stents may limit the ability to interpret CT or MR based imaging. In the absence of high risk features, surveillance for unruptured, untreated aneurysms is usually pursued at 6–12 months initially, followed by repeat imaging every 1–2 years. The follow-up intervals for treated aneurysms are often guided by institutional guidelines, and typically depend on the treatment modality and prior rupture status. Long-term follow-up (e.g. beyond the initial 2–3 years after treatment) is often considered for younger patients with long life expectancy, and/or predisposition for de novo aneurysm formation.
Conclusions
Our understanding of the natural history and treatment outcomes of cerebral aneurysms has significantly increased over the last few decades. Decision making about optimal management requires the consideration of rupture status, location, size, morphology, change over time, as well as the patient’s symptoms, functional status, vascular anatomy, risk factors, age, family history, SAH history and grade. It is key to establish the predicted risks and efficacy of the proposed treatment, and balance it against natural history. Aneurysms should be evaluated in high volume centers with advanced endovascular and surgical capabilities, and the risks and benefits of all management options should be discussed in a multidisciplinary setting. Rapid advancements in endovascular and surgical therapies are expected to result in improved efficacy, decreased recurrence, and better patient outcomes.
Footnotes
Declaration of conflicting interests
The authors disclosed the following: Gabor Toth is a Data Safety Monitoring Board member for the COMPASS (acute stroke intervention) trial. Russell Cerejo has disclosed no financial relationship or interest with any proprietary entity producing healthcare goods or services.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.