
Abstract

A 31-year-old man with no past medical history presented with a 4-month history of worsening pain and swelling along his right medial thigh and calf. Initially, he presented following a mild ankle sprain which was quickly followed by intense erythema and swelling along the medial lower leg with rapid progression in a proximal and medial direction. He denied recent medical procedures or illicit injection drug use. He was treated in the emergency room with non-steroidal anti-inflammatory drugs and ultimately two separate rounds of antibiotics. A venous duplex demonstrated the absence of deep vein thrombosis but suggested thickening of his right great saphenous vein without evidence of thrombosis. His pain and swelling eventually waned but the significant scarring and disfigurement persisted. Physical exam demonstrated a well-circumscribed, pink, sclerotic, firm, non-tender, raised plaque in a linear distribution along the medial calf and thigh, with noticeable alopecia (Panel A). Pertinent laboratory analysis included complete blood count, complete metabolic panel, ESR, CRP, ANA, RF, C-ANCA, P-ANCA, and hepatitis viral serologies, all of which were within normal limits. A repeat venous duplex demonstrated no evidence of acute or chronic deep or superficial thrombophlebitis.

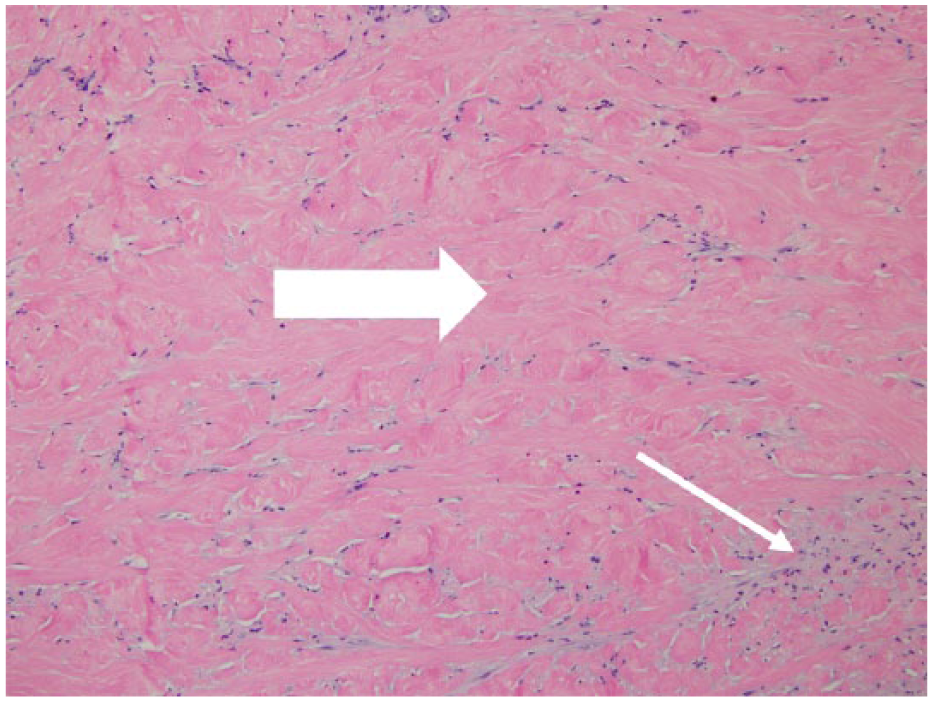
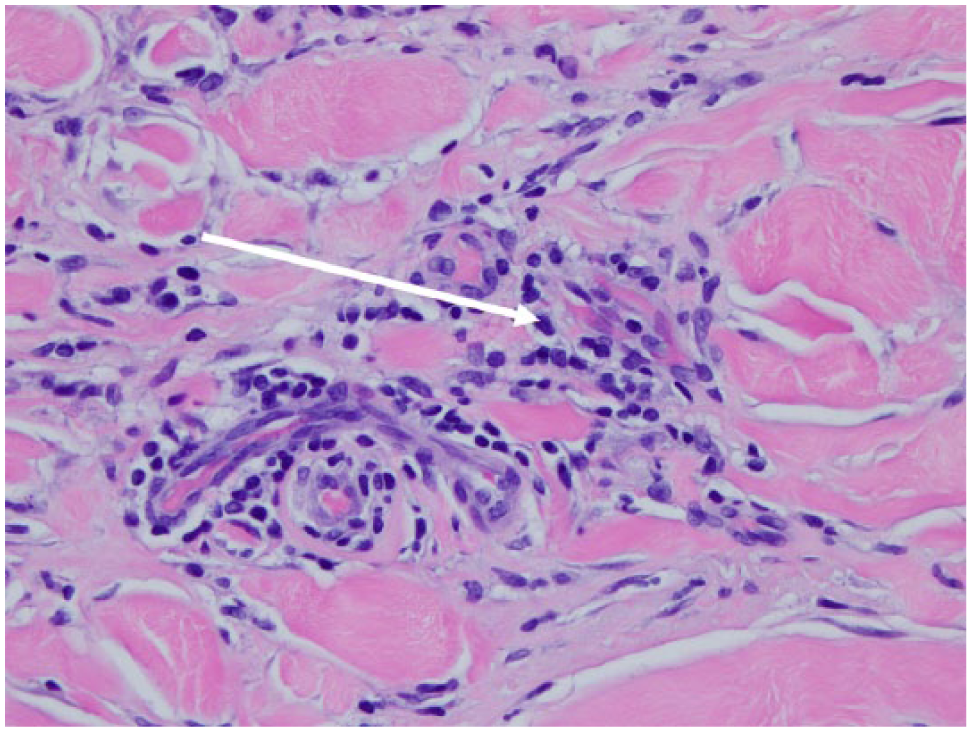
Dermatologic consultation was sought for a clinical suspicion of morphea, given the unusual presentation and lack of evidence for a primary vascular etiology. Panel B demonstrates a microscopic specimen of the biopsy showing both superficial and deep lymphoplasmacytic infiltration (small arrow) and diffuse dermal sclerosis (large arrow; hematoxylin and eosin, ×200). Magnified views also demonstrate perivascular lymphoplasmacytic infiltration (Panel C: arrow; hematoxylin and eosin, ×400). These features and his clinical presentation are consistent with morphea, or localized scleroderma.
Morphea is a relatively uncommon dermatologic disorder associated with inflammatory sclerosis involving the epidermal and dermal layers of the skin but can extend deeper and may even involve tendons. The etiology is not entirely understood but potential triggers may include trauma, friction, infection, radiation, or other environmental exposures. 1 Several subtypes exist and presentations may mimic other inflammatory vascular conditions, as in this case, which involved a distribution commonly seen with superficial thrombophlebitis. 2 Treatment is medical and may include phototherapy, topical calcineurin inhibitors and glucocorticoids, methotrexate, or systemic glucocorticoids. Disease activity can often persist for several years and long-term sequelae from the sclerosis may ensue and include contractures and atrophy. 3
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.