
Abstract
The formation of a fistula between the internal mammary artery and the pulmonary vasculature (IMA-to-PV) is a rare anomaly. The etiology can be congenital; however, most recent cases have been associated with coronary artery bypass grafting, trauma, inflammatory conditions, chronic infections, or neoplasia. The knowledge base on the formation of these fistulas is derived primarily from case reports. To our knowledge, no systematic reviews or guidelines are available that provide information on how to manage these cases, and the treatment of an IMA-to-PV fistula is controversial. To our knowledge, this report is the first to review 80 cases of IMA-to-PV fistulas reported in the literature. We describe the etiologies, clinical presentation, and management of these fistulas.
CME Accreditation Statement
The University of Virginia School of Medicine designates this journal-based CME activity for a maximum of 1 AMA PRA Category 1 CreditTM per article. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Learners are expected to read this article along with any references and supporting material as appropriate, and complete the online post-test questions with an 80% pass rate to receive credit. Post-test questions are accessed through the member portal on the Society for Vascular Medicine (SVM) website (www.vascularmed.org). Please note that CME credits are only available to members of SVM with a journal subscription. This activity expires 2 years after the publication date, on October 1, 2019.
Heather Gornik has disclosed research support from AstraZeneca, intellectual property rights from Summit Doppler Systems, Inc, and intellectual property rights and stock/ownership from FlexLife Health (proceeds donated). Aditya Sharma has disclosed research support from National Institute of Health Sciences, AstraZeneca, Biomet Biologics, Portola Pharmaceuticals, and Pedra Technology. Valerie Clark has no financial affiliations to disclose.
Introduction
The formation of a fistula between the internal mammary artery (IMA) and the pulmonary vasculature (PV) is a rare anomaly. Historically, the first case of an IMA-to-PV fistula was reported at the Mayo Clinic in Rochester, MN, by Burchell and Clagett. Their findings were subsequently published by the American Heart Journal in 1947. 1 This case was described as an anomaly because from 1955 to 1965, only two other cases were reported at Mayo. 2 However, 10 cases were reported worldwide by 1980. 3 The early cases of IMA-to-PV fistulas were deemed congenital, but most recent cases have been associated with coronary artery bypass graft surgery (CABG), trauma, inflammatory conditions, chronic infections, or neoplasia.4–6
Current knowledge about the formation of these fistulas primarily comes from case reports; no consensus guidelines for the evaluation and management of IMA fistulas are available.7–18
Anatomically, most cases of congenital IMA-to-PV fistulas arise from the middle third of the IMA, while other cases of IMA fistulas to the internal mammary vein or the inferior vena cava arise from the proximal third of the IMA.19,20
The primary mechanism for developing an IMA fistula is not fully understood. Theories propose idiopathic and iatrogenic pleural and lung parenchymal injuries, improper surgical technique during left IMA branch ligation, or the use of electrocautery instead of ligation of side branches; infection and hematoma may lead to neovascularization and cause fistula formation.21,22
The treatment of an IMA-to-PV fistula is controversial. In this report, we review the risk factors and clinical presentation for the cases reported in the literature and discuss proposed treatment strategies.
Methods
We conducted a literature search for case reports and case series on IMA-to-PV fistulas in MEDLINE, PubMed, and Google Scholar, using the keywords: ‘internal mammary artery’, ‘pulmonary artery’, ‘pulmonary vein’, and ‘fistula’. All articles published from 1947 through 2016 were included in our search, and each case was reviewed. We included case reports that discussed a fistula between the IMA and PV. We defined an IMA-to-PV fistula as any abnormal communication between either of the IMA vessels to pulmonary arteries, veins, and bronchial arteries. Other arteriovenous fistulas were excluded. The following data were collected: sex, age of patient at onset of presenting symptoms, IMA fistula diagnosis time from surgery, and treatment methods, when applicable. Other possible contributing factors were also examined. Patient treatment and outcomes were compared when reported. Two authors (AP and NM) independently screened the case report titles. They obtained the full articles that met the criteria. Discrepancies were resolved in agreement with two other authors (SA and AA). Because these data were previously published, institutional board approval was waived. Our selection process followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement (Figure 1). The literature search was conducted between April 2015 and February 2016.
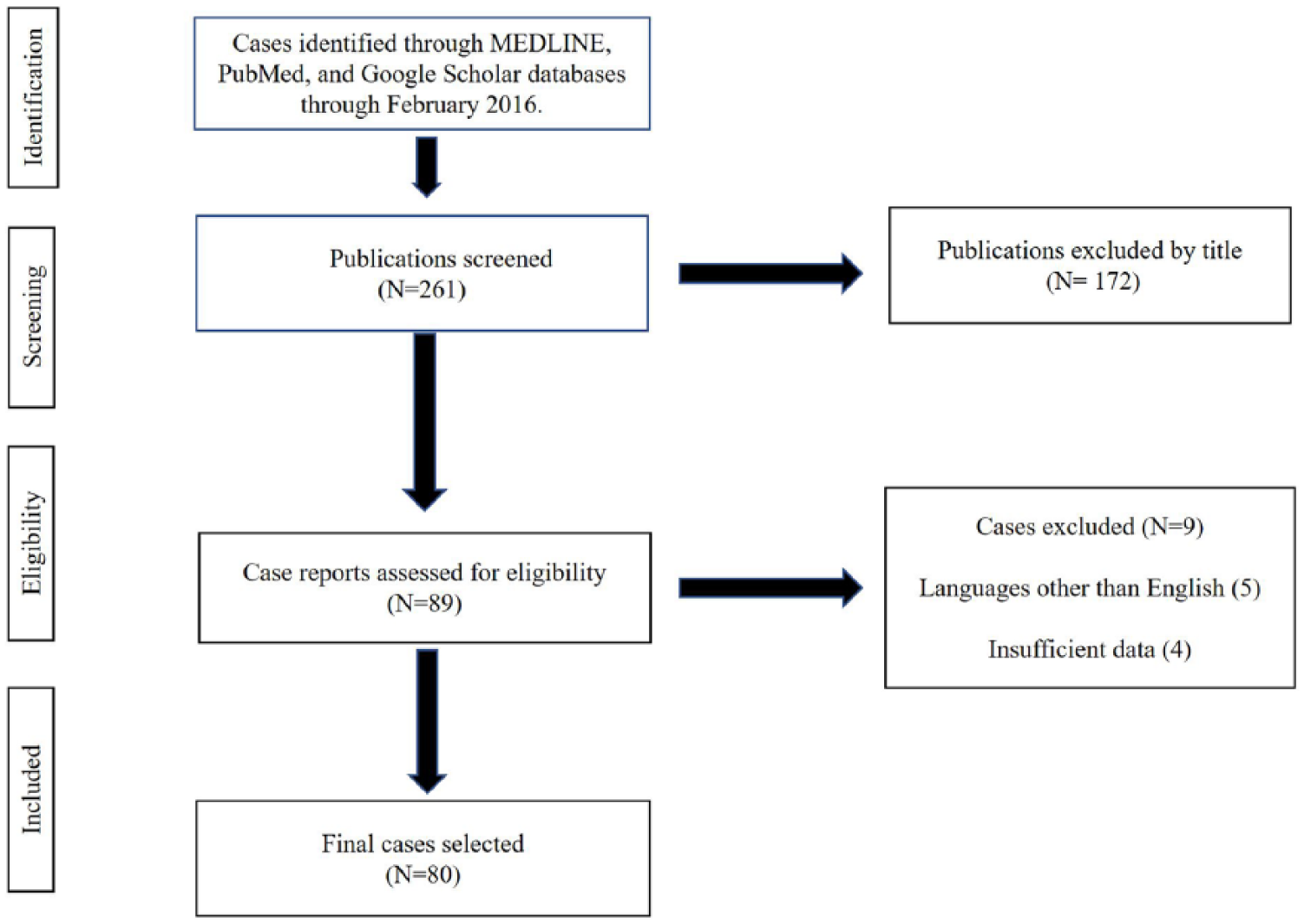
Study selection process.
Results
Our search initially yielded 89 published case reports of IMA-to-PV fistulas. Of those, nine case reports were excluded because of insufficient data or the language of publication. 23 The remaining 80 cases were published between 1970 and 2016.
Demographically, we found that the male-to-female ratio was 20:1 in post-CABG cases, and the mean age of these patients was 51 years at presentation. Only 15% of the fistulas were congenital; the rest were acquired. Interestingly, the left IMA and pulmonary artery were involved in 91% (75 cases, including two cases with bilateral IMA fistula) of all the cases we identified (congenital, postoperative, other causes). We found only five published cases of right IMA fistula. The mean age of presentation for congenital fistulas was 40 years, although a few outliers skewed the mean (median = 32 years). The female-to-male ratio in the congenital cases was 1:1 (Table 1).
Patient characteristics extracted from published case reports of IMA-to-PV fistulas.
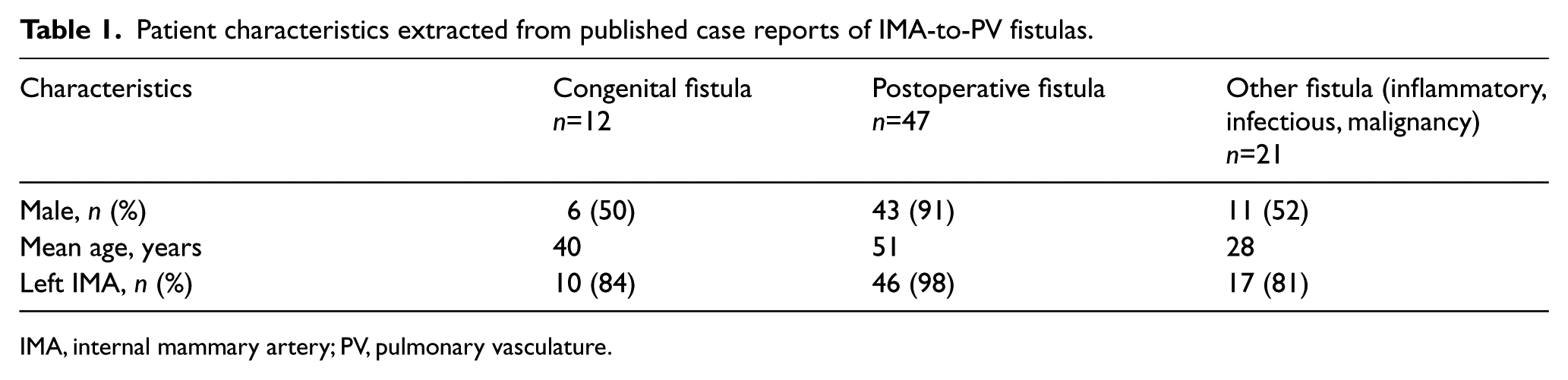
IMA, internal mammary artery; PV, pulmonary vasculature.
Etiology
CABG was the most reported etiology for the formation of fistula, accounting for 47 cases (59%). In the ‘other’ category (n=21), Takayasu arteritis accounted for four cases, and tuberculosis was reported in four case reports. One non-Hodgkin lymphoma case was reported. Finally, we identified five cases of postprocedural (other than CABG) fistulas that included video-assisted thoracoscopic surgery, chest tube placement, and mitral valve replacement surgery. A case of chest trauma was also identified (Table 2). Etiology was not identified for six cases.
IMA fistula etiology for the ‘other’ category (n=21).
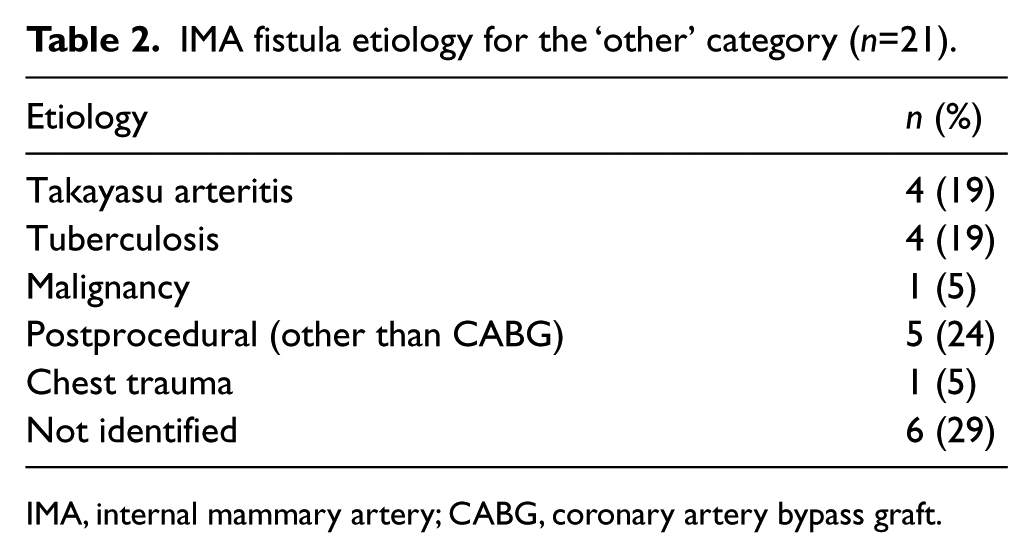
IMA, internal mammary artery; CABG, coronary artery bypass graft.
Clinical presentation
The timing of patient presentation following CABG ranged from as early as 2 months 24 to as late as 16 years following surgery. 25 Angina was the most common presenting symptom in the acquired cases (Table 3), reported by 88% of the postoperative patients in our review.3,26 –28 Other patients in the postoperative group presented with dyspnea (6%). Only two cases presented with myocardial infarctions. Continuous murmur was the primary clinical sign in patients with congenital IMA fistula (42%), but the clinical presentation was not clear in 50% of the cases. The majority of patients in the ‘other’ group (inflammatory, infectious, and malignancy cases) presented with dyspnea, angina, and murmur (62%), while presentations in the rest of the group were either unclear or incidental. Myocardial perfusion imaging was performed in only 11% of the cases; most CABG-related IMA fistula cases were diagnosed by selective angiography.
IMA fistula clinical presentations.
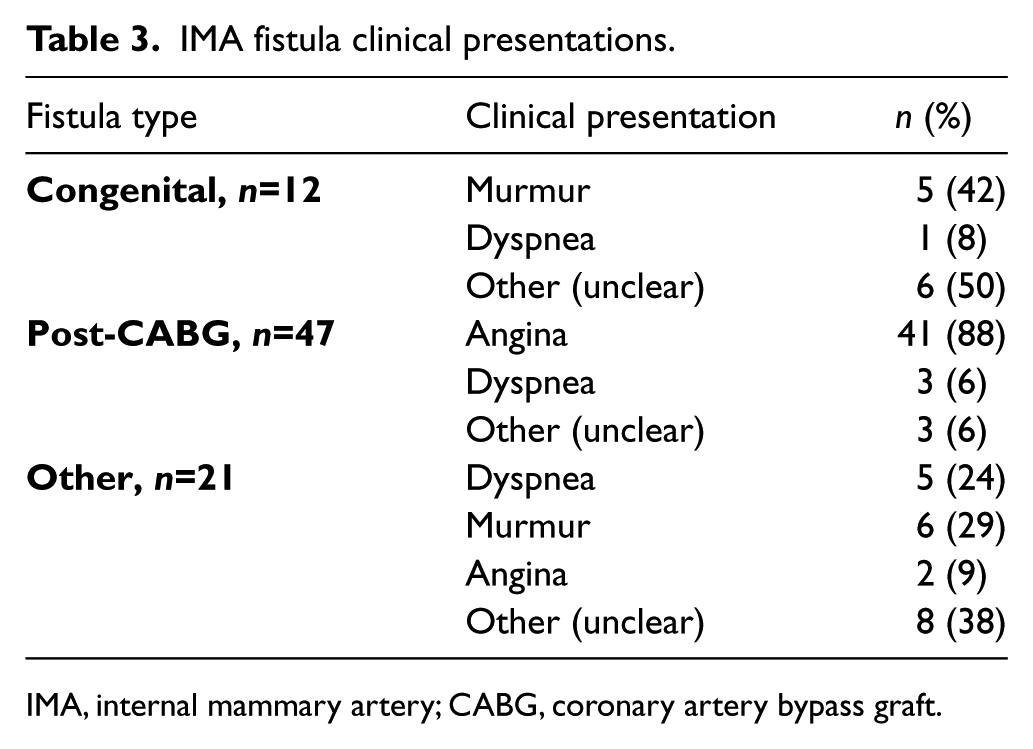
IMA, internal mammary artery; CABG, coronary artery bypass graft.
Management
Nineteen cases (24%) were treated surgically, 10 (12%) were managed with coil embolization, eight (10%) were treated with a covered polytetrafluoroethylene (PTFE) stent, and two patients had a re-grafting procedure. Twenty-five patients (31%) were treated medically; of those, 13 patients (52%) reported a symptomatic improvement. Management of the remaining 18 cases was not clear (Table 4).
Clinical management of IMA fistula.
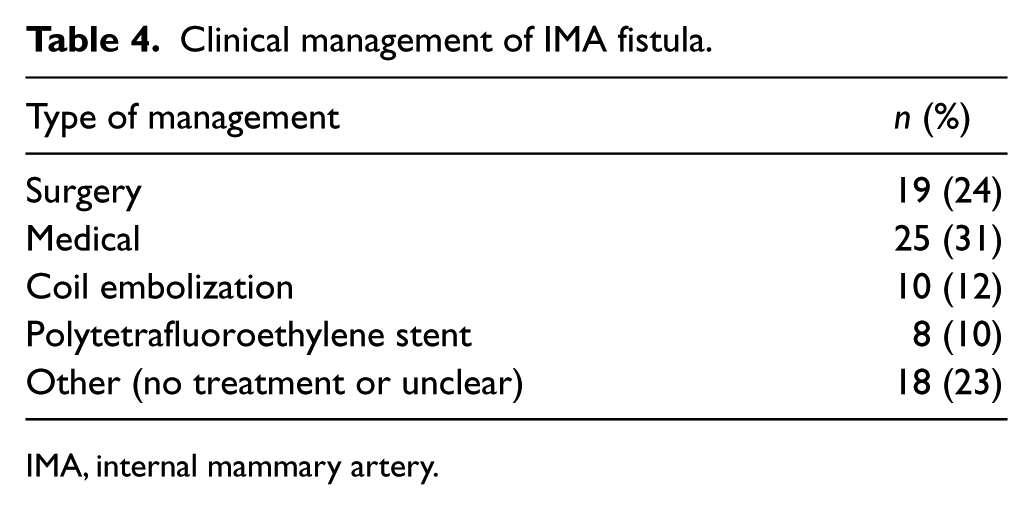
IMA, internal mammary artery.
Discussion
Even though the trend of case publication of these fistulas seems to be increasing, it is too early to conclude that cases of IMA fistulas are more common today than 40 years ago. In the most recent retrospective study, five of 537 patients (0.93%) undergoing cardiac catheterization after CABG were found to have IMA-to-PV fistulas, 27 which represents an increase from the previously reported data. 29 Figure 2 shows the increasing number of IMA fistula cases published from 1970 to 2009. The reason behind the low number of cases published from 2010 to 2016 is that we still have incomplete data; new data will likely be reported in the next 3 years.
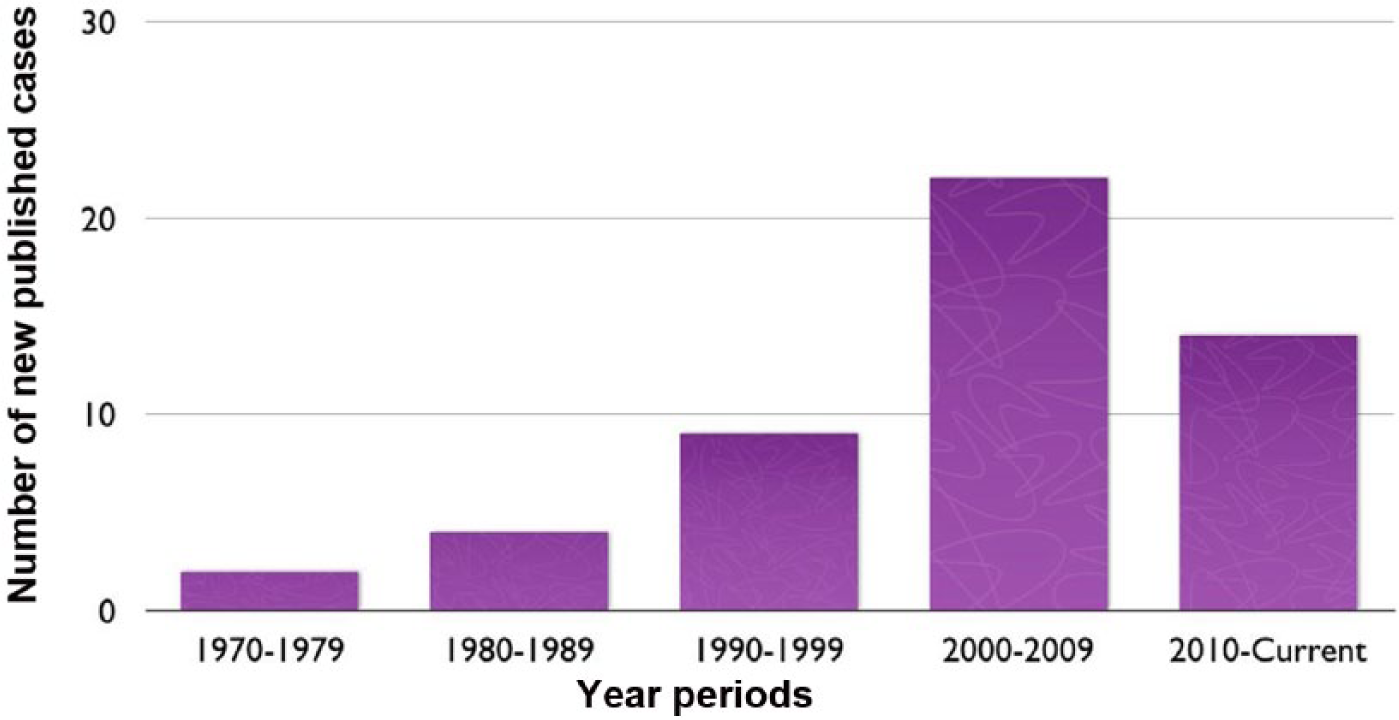
The number of internal mammary artery-to-pulmonary vasculature fistula cases reported by year.
We assume the reason behind the increasing number of identified non-congenital cases of IMA fistula is related to the increase in CABG surgeries during the last three decades and the improvement in imaging and angiography technologies and techniques. The number of identified congenital cases of IMA fistula has been stable for the last three decades and ranges from two to four cases per decade.
Congenital fistulas are detected incidentally when a continuous murmur is auscultated on physical examination; other patients will have a normal examination throughout their disease course.30,31 Although congenital fistulas are usually asymptomatic, acquired fistulas can present with a variety of symptoms including angina, dyspnea, heart failure, or coronary steal syndrome.30,32
Most cases of non-congenital (non-CABG) fistulous connections of the IMA to the nearby venous (internal mammary, innominate, jugular, and cardiac) and arterial (subclavian, carotid, and coronary) vasculature were post-laser extractions, cardiac and aortic surgeries, or percutaneous catheter placement.33–38
Although an IMA-to-PV fistula is uncommon, it should be considered in the differential diagnoses of worsening symptoms post-CABG, especially in patients on hemodialysis in whom the steal phenomenon from an ipsilateral arteriovenous fistula has been attributed to worsening angina symptoms. 39
The fact that the most reported cases of postoperative fistulas (91%) (Table 1) involved the left IMA likely represents a selection bias, because a left IMA selective angiogram is most commonly performed following CABG procedures. This does not explain the higher percentage of left IMA in cases of congenital fistulas, however. We found two cases of fistulas that involved both the right and left IMA.40,41
In cases of post-CABG fistula formation, the etiology is not well understood. Trauma from dissection of the IMA may lead to adhesion formation, neovascularization, and alteration of normal blood flow 42 that will ultimately lead to a fistula between the IMA and nearby PV. Progression of the disease may lead to dilation of the fistula and significant morbidities. 43 The fatal coronary-to-pulmonary steal syndrome has been described in a case report that discussed the indication of immediate medical intervention. 32
Different surgical techniques have been associated with the development of post-CABG fistulas. Electrocoagulation may increase the risk of neovascularization compared to surgical clipping. 44 Pericardial flap, minimally invasive CABG, or repeat CABG may also increase the risk of fistula formation. 24 Infection or trauma from sternal wires may play a role in the pathologic process. 43
Advanced imaging modalities such as computed tomography angiography can delineate the course of the fistula and be very informative when the anatomy is complex, but a selective angiogram contrast injection of the IMA graft at the time of cardiac catheterization is a more cost-effective way to establish the diagnosis in most cases of IMA-to-PV connections. 45 Both invasive and non-invasive modalities have been used to establish the hemodynamic significance of IMA-to-PV fistulas (Figure 3). 46
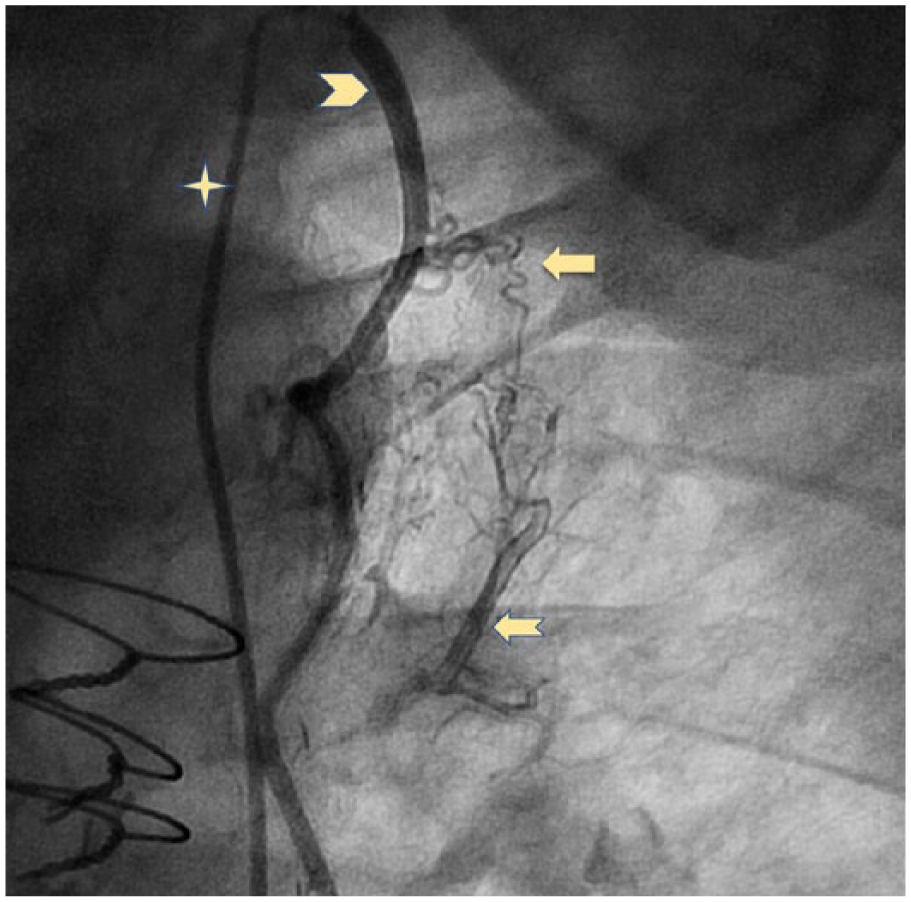
Selective angiogram of the left internal mammary artery (IMA) showing the abnormal communication (i.e. fistula) to the pulmonary artery. (Four-point star: catheter; arrowhead: IMA; solid arrow: fistulous communications; notched arrow: sub-segmental pulmonary artery.)
Conservative therapy is the most common treatment approach, and 52% of patients treated with medical therapy only (i.e. antianginal therapy) reported positive results. Other authors reported a wide range of percutaneous interventions to provide relief of symptoms. Endovascular approach with PTFE-covered stents, coil embolization, and bovine pericardium-covered stents were all used with positive results.47–51 Although surgical intervention has been implicated in fistula etiology, surgical clipping has been used successfully in the treatment of fistulas. 45
Limitations
Despite our extensive search, we were able to find 80 cases only. Case reports in non-English languages were excluded. Not all case reports were clear about management of the IMA fistula.
Conclusion
The appropriate treatment of IMA-to-PV fistulas remains a clinical judgment based on the severity of the presentation. Although conservative medical management is suitable for mild symptoms, percutaneous intervention with covered stents and coil embolization has been proven to be a feasible and effective therapeutic option for patients who fail medical therapy, have advanced symptoms, or are high-risk surgical candidates.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.