
Abstract
Although postoperative delirium is a common complication and increases patient care needs, little is known about the predictors and outcomes of delirium in patients having vascular surgery. This review aimed to determine the incidence, prognostic factors and impact of postoperative delirium in vascular surgical patients. MEDLINE and EMBASE were systematically searched for articles published between January 2000 and January 2016 on delirium after vascular surgery. The primary outcome was the incidence of delirium. Secondary outcomes were contributing prognostic factors and impact of delirium. Study quality and risk of bias was assessed using the QUIPS tool for systematic reviews of prognostic studies, and MOOSE guidelines for reviews of observational studies. Quantitative analyses of extracted data were conducted using meta-analysis where possible to determine incidence of delirium and prognostic factors. A qualitative review of outcomes was performed. Fifteen articles were eligible for inclusion. Delirium incidence ranged between 5% and 39%. Meta-analysis found that patients with delirium were older than those without delirium (OR 3.6, p<0.001). Prognostic factors predicting delirium included increased age (OR 1.04, p<0.001), pre-existing cognitive impairment (OR 9.8, p=0.01), hypertension, pre-existing depression and open aortic surgery. Delirious patients remained in hospital 6 days longer (p<0.001) and had more complications than patients without delirium. Data were limited on the impact of procedure complexity, endovascular compared to open surgery or type of anaesthetic. Postoperative delirium occurs frequently, resulting in major morbidity for vascular patients. Improved quality of prognostic studies may identify modifiable peri-operative factors to improve quality of care for vascular surgical patients.
Keywords
Introduction
Postoperative delirium is a frequent and often unrecognized complication of surgery. Delirium is defined as an acute fluctuation in cognitive status, with features of inattention and altered levels of consciousness. Delirium is known to contribute to increased peri-operative complications and length of stay, functional decline and mortality.1,2 Delirium is both preventable and treatable with environmental, supportive and pharmacological interventions. 2 For vascular surgery, where patients are often older, frail and generally more at risk of adverse outcomes, delirium represents a major potentially modifiable risk factor. The incidence and impact of postoperative delirium after major vascular surgery is unknown. Although there are many clinically applicable validated diagnostic tools for diagnosis of delirium, over 50% of inpatient delirium is unrecognized. 3 Research studies have shown that there are multiple contributing factors for the development of delirium, often with conflicting results.4,5
Prognostic factor research aims to identify and evaluate those factors that may become targets of modifiable outcome improvements, can be included as predictor variables in multivariable prognostic models that predict disease endpoints, or can be used to stratify patients and identify those most likely to benefit from a treatment or intervention. A prognostic factor is one that is present in people with a particular disease at a given start point, and that influences the clinical course and outcomes of a condition. 6 In contrast, risk factors are defined as those factors associated with the cause of a condition. Consideration of prognostic factors for delirium in patients having major vascular surgery is important so that specific interventions can be developed for this cohort to improve outcomes. Understanding the strength and consistency of the relationship of specific prognostic factors for delirium can assist in understanding the trajectories of illness and identify potentially modifiable factors that may influence outcomes.
This study aims to systematically review the medical literature to establish the incidence of peri-operative delirium after major vascular surgery, determine which vascular surgical procedures have the highest risk of delirium, and identify prognostic factors associated with developing delirium. It will also assess the impact that delirium has upon surgical outcomes such as length of stay and complication rates. This study will adhere to internationally recognized standards for systematic reviews of prognostic studies, incorporating the novel use of recently validated risk of bias assessment methods for prognostic studies.
Methods
Search strategy and selection criteria
A systematic search for all articles that measured delirium after major vascular surgery was conducted. MEDLINE and EMBASE were systematically searched for articles published between 1 January 2000 and 30 January 2016. MESH terms included delirium, cognitive disorders and vascular surgical procedures with a text word search designed to include all major vascular surgical procedures (see Online Supplemental Table 1). A hand search of contents lists of major vascular surgery journals was also performed. This review was registered with the Prospero Register of Systematic Reviews in April 2015. 7
Studies were eligible for inclusion if they reported original data on delirium after major vascular surgery. Clinical trials along with case–control, cohort studies and case-series (with more than 10 participants) were included. Case reports, review articles, editorials and conference proceedings were excluded. Patients who had aortic, carotid, peripheral or endovascular surgery formed the population of interest.
The search strategy was developed in conjunction with a medical librarian. Searches were limited to publications in English. Search results were recorded according to the PRISMA guidelines. After removing duplicates, titles and abstracts were screened using the inclusion/exclusion criteria. Remaining articles were assessed for eligibility by full text review (SJA, FB, VN) and the decision on inclusion decided by consensus. The references of included articles were searched to identify any additional relevant studies.
The primary outcome was the incidence of postoperative delirium, diagnosed by a validated diagnostic tool, such as the Diagnostic and Statistical Manual of Mental Disorders criteria (DSM-IV) or Delirium Observational Scale (DOS). The differential risk associated with surgery type (aortic vs other; open vs endovascular aortic) and anaesthesia type (general vs loco-regional) was also assessed. Secondary outcomes were prognostic factors predicting delirium, the association of delirium with advancing age, and outcomes of length of stay, mortality and morbidity.
Prognostic factors were defined as those that were primarily investigated as predictive factors for delirium incidence after major vascular surgery using multivariable analysis. Prognostic factors were categorized into patient, procedural and peri-operative management factors. Confounding factors were defined as other factors included in multivariable analysis that were not defined as prognostic factors in the study, but were included based on prior evidence and clinical knowledge of their relationship with the development of delirium.
Quality assessment (risk of bias)
Studies were assessed for risk of bias using the Quality in Prognostic Studies (QUIPS) tool, 8 a validated tool for assessing risk of bias in prognostic factor studies.6,8,9 QUIPS provides a qualitative assessment of six key areas – study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding and statistical analysis and presentation. 8 All three authors (SJA, FB, VN) independently assessed each study, ranking the risk of bias as high, moderate or low. If the authors disagreed on their risk of bias rating, a consensus agreement was reached by joint review and discussion of the article. This review has been conducted according to the quality checklist developed by the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines. 10 A full description on how this study complies with the MOOSE guidelines is provided in the Online Supplemental Table 2.
Statistical analysis
Study data were extracted using a pre-designed, standardized proforma (primary extraction by SJA; verification of accuracy assessed by FB and VN). This included information on study characteristics (Table 1), patient characteristics and quantification of results (odds ratio or hazard ratios of prognostic factors identified on multivariable analysis, mean and standard deviation of continuous variables).
Studies on the incidence of delirium in vascular surgery patients.

DOS, Delirium Observation Scale; NEECHAM, Neelon and Champagne Confusion Score; HDS-R, Revised Hasegawa Dementia Scale; CAM, Confusion Assessment Method; DRS, Delirium Rating Scale; DSM-III, IV, Diagnostic and Statistical Manual of Mental Disorders III, IV; MDAS, Memorial Delirium Assessment Scale; MMSE, Mini-Mental State Examination; TAMI, Transient Advanced Mental Impairment Score.
Results were collated in Review Manager v5.3 (RevMan, The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen). Meta-analysis of prognostic factors was considered where there were more than three studies reporting an association between the prognostic factor and delirium. Meta-analysis of prognostic factors was only deemed possible for those studies where the patient characteristics were significantly similar at baseline in terms of age, sex, procedural magnitude and study quality (design and confounders) and where multivariable analysis included similar variables. A random-effects inverse variance meta-analysis would be calculated in RevMan using individual odds ratios transformed to their logarithms to normalize their distribution, and standard errors (SEs) calculated from the 95% confidence intervals (CIs).8,11,12 Heterogeneity was anticipated to be high (defined by I2 statistic as greater than 50%), as is consistent with other meta-analyses of observational studies 13 due to the lack of randomization. The incidence of postoperative delirium was presented as a percentage range rather than an overall mean. Mean age, hospital length of stay and duration of intensive care stay data were collated in RevMan. Unadjusted mean difference was used for meta-analysis of age and length of stay. A qualitative review was performed of outcomes and prognostic factors that were not eligible for meta-analysis.
Results
The results of the search strategy are reported in Figure 1. Fifteen studies14–28 were eligible for inclusion and used to establish the incidence of delirium: eight studies were used to quantify hospital length of stay16,19–21,24–26,28, eight studies for assessing the association of age with delirium14,15,17,21,22,25–27 and 10 studies were used in the prognostic factor analysis.14,15,17–19,21,22,26–28 Three studies were included in the meta-analysis examining age as a prognostic factor for delirium,15,18,22 and three studies in the meta-analysis examining pre-existing cognitive impairment.14,29 Three studies were earlier publications which included the same patient cohort used in later publications.30–32 Where there were multiple publications related to one study, the most recent publication was selected unless different prognostic factors and outcomes were reported in separate publications.14,16,19,22,27 Rudolph et al. 23 was included only in the analysis of delirium incidence as this study had no analysis of prognostic factors. The major reasons for study exclusions were that procedures were not major vascular surgery, or due to study type (commentaries, editorials, or small case series).
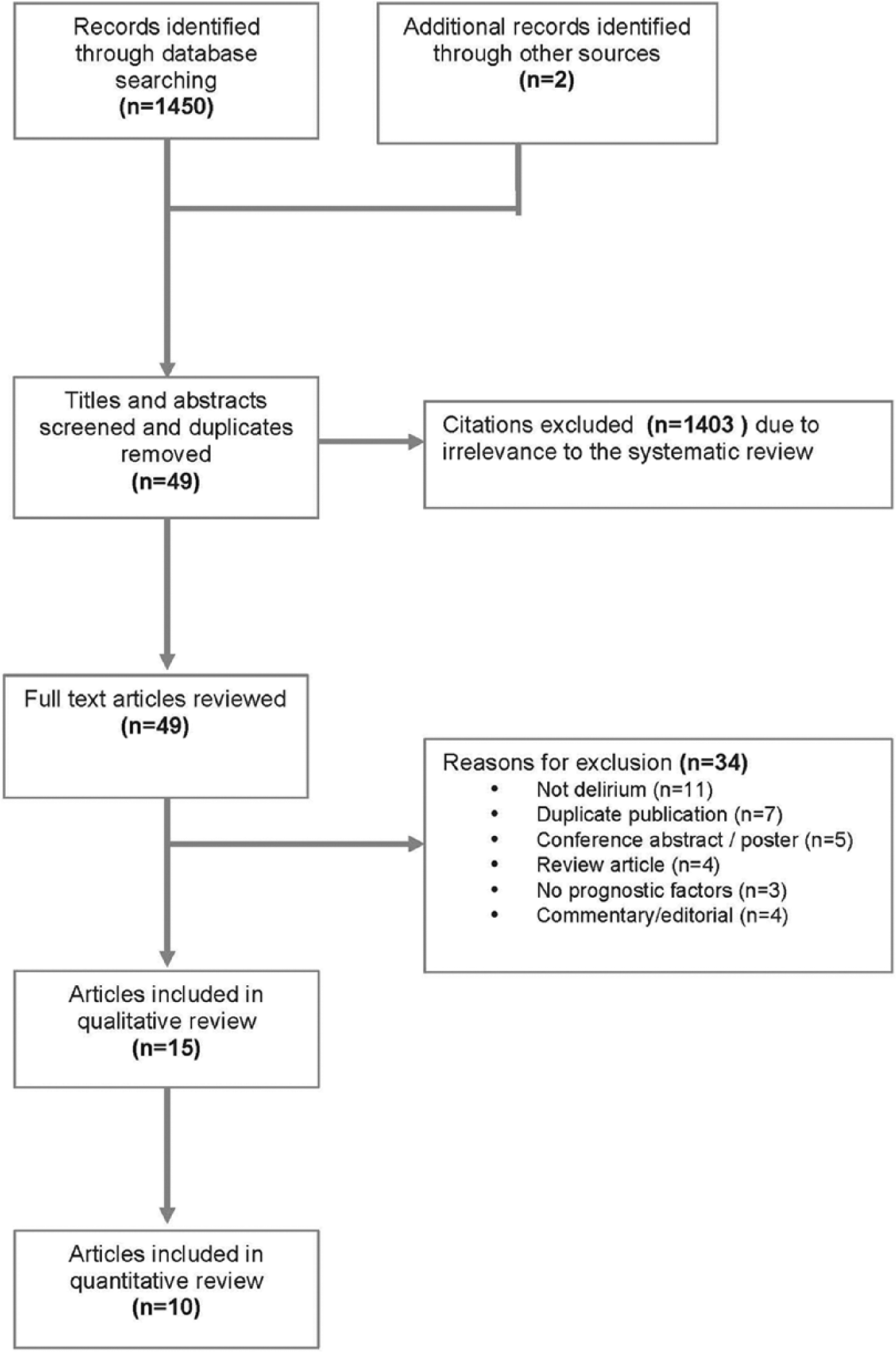
PRISMA flow diagram of search results.
The design and characteristics of the included studies are shown in Table 1. All were observational studies, with the majority (n=9, 64%) being prospective cohort studies. The median study size was 197 participants (range 35–582) and the total number of participants was 2650 (excluding duplicate studies).
Study quality and risk of bias
QUIPS ranking did not vary by more than one category between raters for any criteria for each publication and consensus was achieved for all rankings. Table 2 presents the QUIPS analysis for risk of bias. Study quality was variable. The most common reasons for studies having a moderate or high risk of bias were poorly described study participation (36%, n=5) and attrition rates (29%, n=4), inadequate adjustment for confounders (79%, n=11) and inadequate statistical analyses (43%, n=6).
Risk of bias assessment using the Quality in Prognostic Studies (QUIPS) tool 8 for included studies.
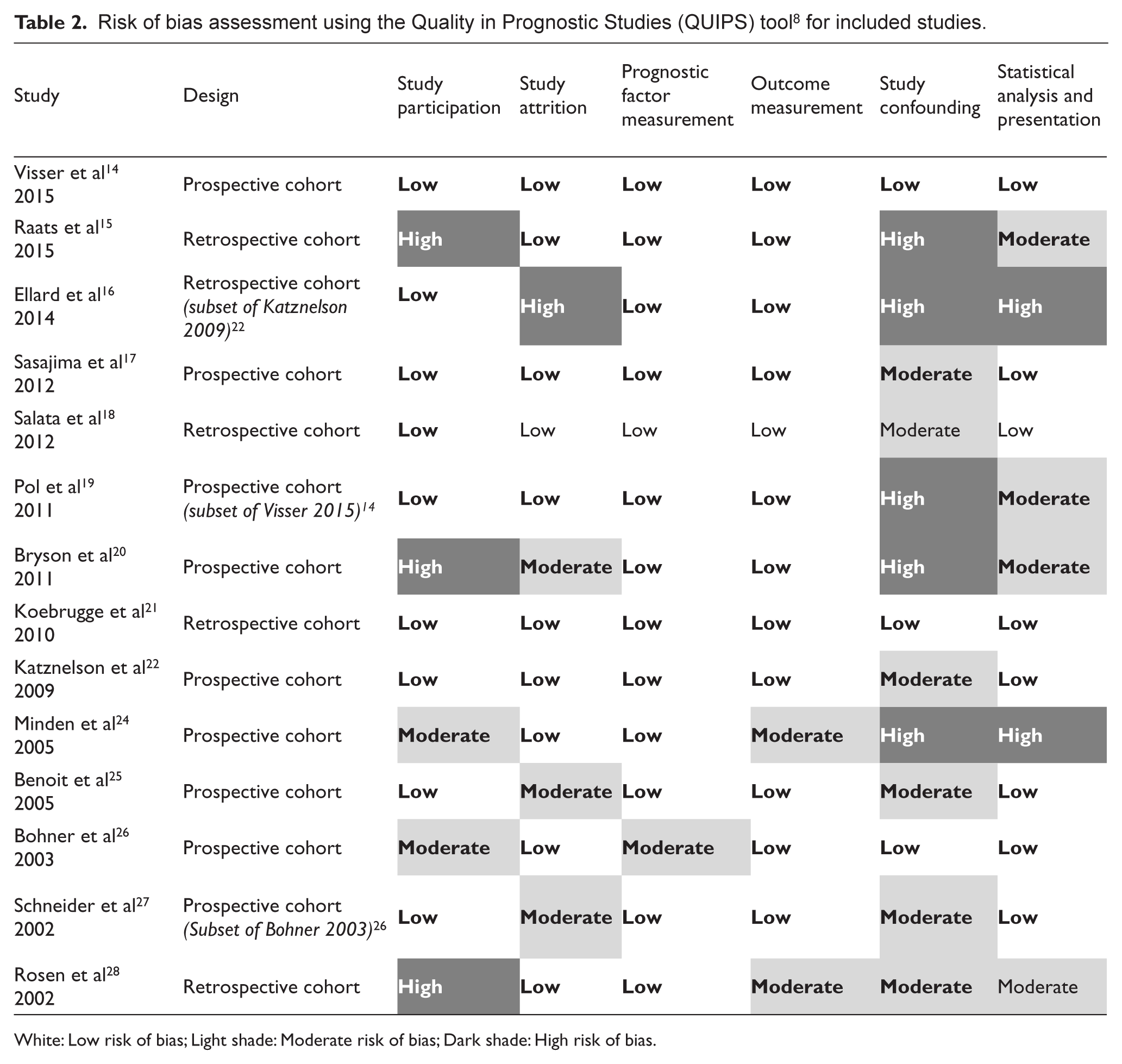
White: Low risk of bias; Light shade: Moderate risk of bias; Dark shade: High risk of bias.
Incidence of delirium
The incidence of postoperative delirium ranged between 5% and 39%. The majority of studies found the incidence of postoperative delirium to be greater than 20% (n=10). The mean duration of delirium ranged between 1 and 30 days. Based on the meta-analysis of eight studies,14,15,17,21,22,25–27 patients with delirium were more likely to be older than patients without delirium (OR 3.6, 95% CI 1.6–5.5, p<0.001) (Figure 2).
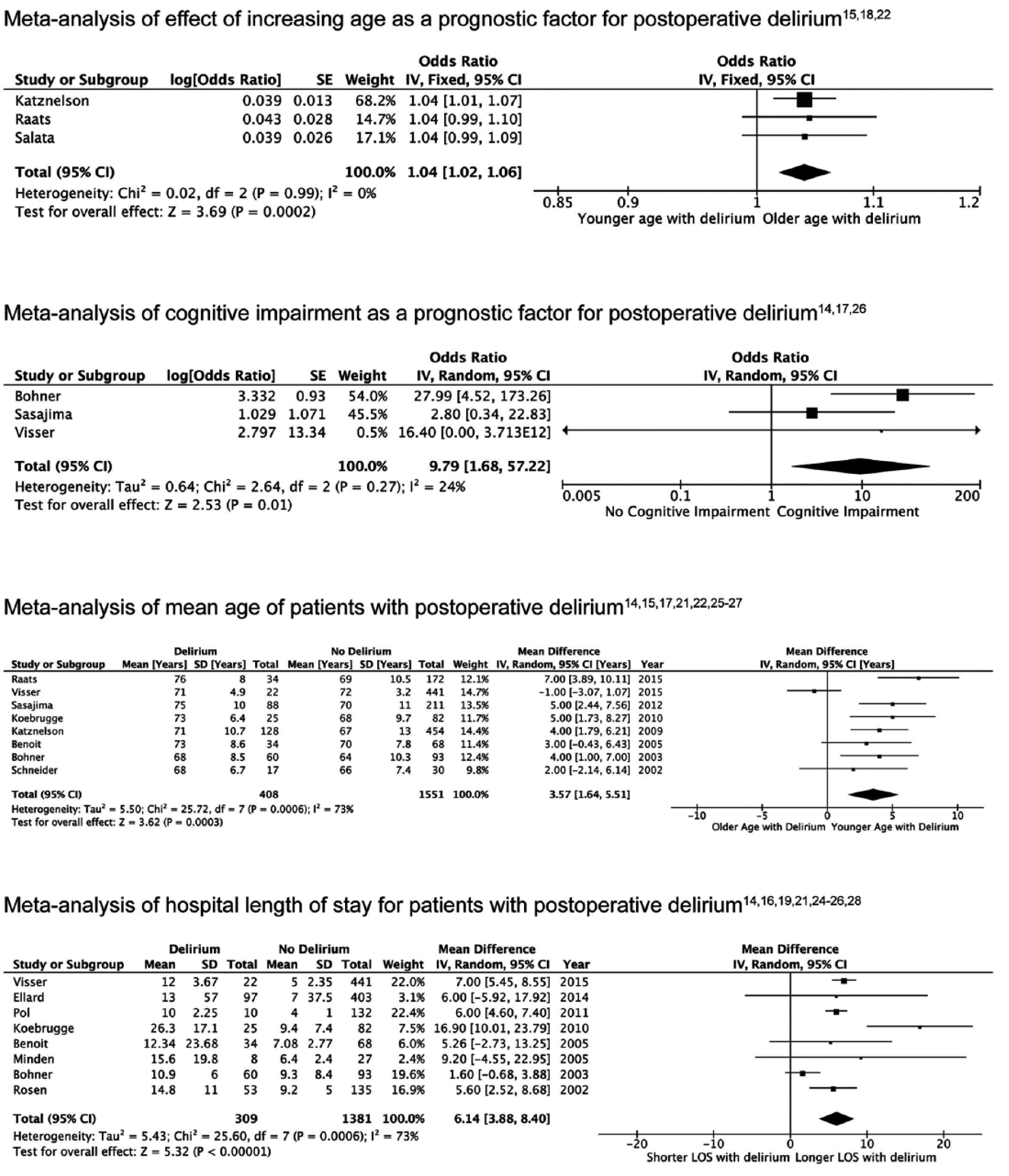
Results of meta-analysis on prognostic factors and outcomes for postoperative delirium.
Prognostic factors for risk of developing delirium
Ten14,15,17,18,19,21,22,26–28 of the 15 studies conducted multivariable analysis to investigate prognostic factors associated with the incidence of postoperative delirium. Table 3 summarizes these results, with further information included in the Online Supplemental Table 3.
Summary of prognostic factors related to post-operative delirium on multivariable analysis.
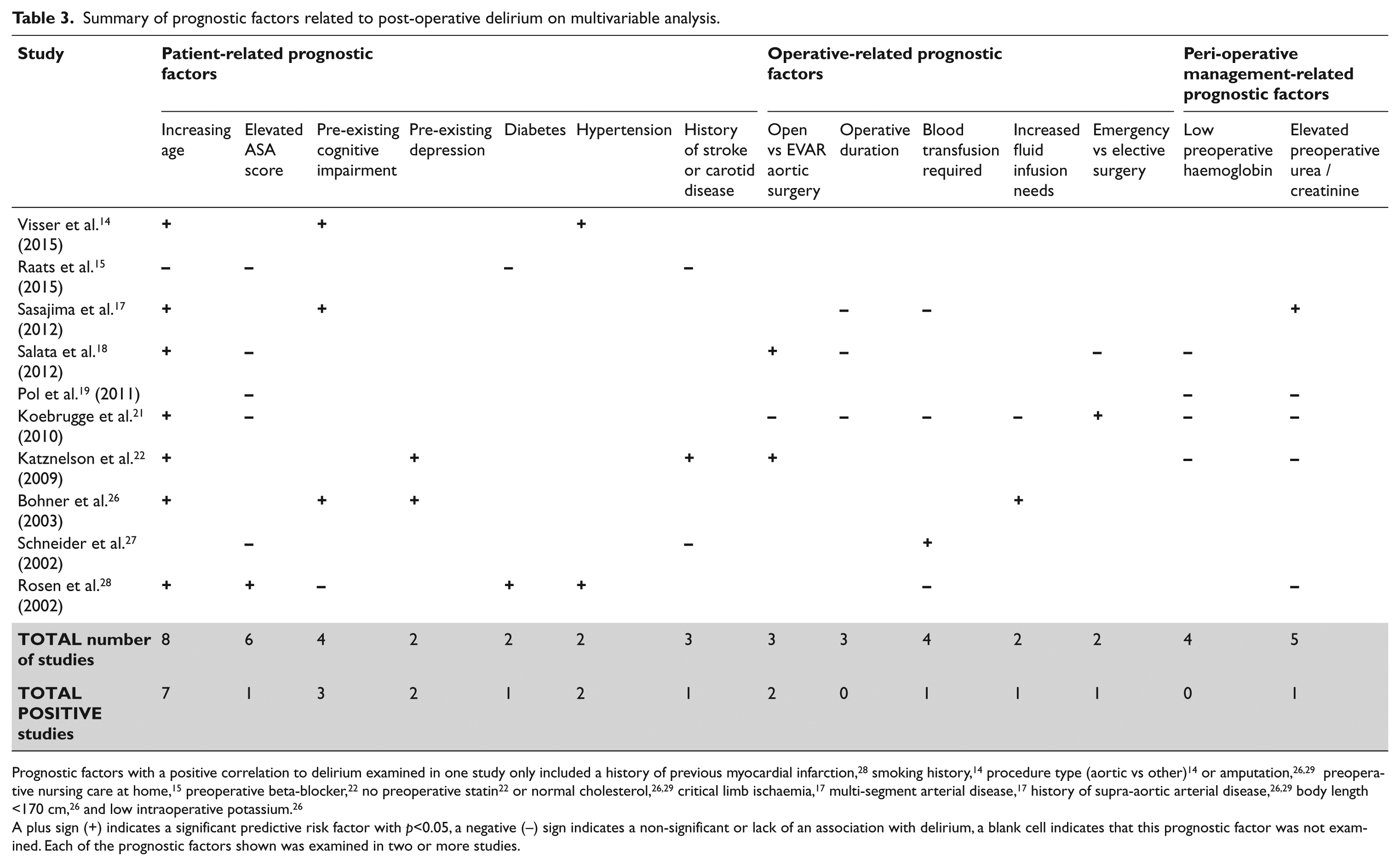
Prognostic factors with a positive correlation to delirium examined in one study only included a history of previous myocardial infarction, 28 smoking history, 14 procedure type (aortic vs other) 14 or amputation,26,29 preoperative nursing care at home, 15 preoperative beta-blocker, 22 no preoperative statin 22 or normal cholesterol,26,29 critical limb ischaemia, 17 multi-segment arterial disease, 17 history of supra-aortic arterial disease, 26,29 body length <170 cm, 26 and low intraoperative potassium. 26
A plus sign (+) indicates a significant predictive risk factor with p<0.05, a negative (−) sign indicates a non-significant or lack of an association with delirium, a blank cell indicates that this prognostic factor was not examined. Each of the prognostic factors shown was examined in two or more studies.
Increased age was the most frequently identified prognostic factor for predicting delirium (seven of eight studies).14,15,17,18,21,22,26,28 Three studies measured age as a continuous variable15,18,22 and were suitable for meta-analysis. On meta-analysis, increasing age was associated with the development of delirium (OR 1.04, 95% CI 1.02–1.06; I2=0%, p<0.001) (Figure 2). A further five studies14,17,21,26,28 reported age as a dichotomous variable, with cut-points varying between >64 and >80 years old. While these studies found an association with the older age groups and delirium, they were unable to be included in the meta-analysis.
Pre-existing cognitive impairment14,17,26,28 had a positive association with delirium in three of four studies. On meta-analysis of these three studies,14,17,26 pre-existing cognitive impairment predicted the development of delirium (OR 9.79, 95% CI 1.7–57.2, p=0.01) (Figure 2). Six studies15,18,19,21,27,28 included the American Society of Anesthesiologists (ASA) classification in multivariable analysis but were unable to be combined in meta-analysis due to variation in ASA cut-points. Only one of these studies showed ASA to be a prognostic factor for delirium. 29
Aortic surgery and delirium risk
Aortic surgery had an increased risk of delirium in a single study 15 (OR 1.77, 95% CI 1.04–3.02, p=0.004), while patients having either aortic surgery or amputation were at greater risk of delirium compared to other vascular surgical procedures (OR 14.0, 95% CI 3.9–49.8, p<0.001) in another study. 14 None of the other 12 studies reported a comparison of aortic surgery versus other non-aortic surgical procedures. Open aortic surgery had a greater risk of postoperative delirium compared to endovascular aortic surgery (EVAR) in two of the three studies that compared these procedures.18,21,22
Impact of anaesthetic type on incidence of delirium
There were no studies that assessed anaesthetic type as a prognostic factor in multivariable analysis. Three studies examined the impact of anaesthetic type on rates of delirium using crude ratios or univariate analysis.16,21,22 None of these three studies found that general anaesthetic was prognostic of delirium development; however, they did not account for use of sedation, patient comorbidities or type of anaesthesia such as general versus loco-regional anaesthesia. The QUIPS risk of bias score demonstrated a moderate–high risk of bias for confounding and analysis in two of these three studies.16,22
Impact of postoperative delirium on peri-operative outcomes
Postoperative delirium significantly increased the length of hospital stay for vascular patients. Eight studies reported on differences in length of stay between patients with and without delirium (Figure 2). On meta-analysis, patients with delirium remained over 6 days longer than those patients without delirium (6.1 days, 95% CI 3.9–8.4, p<0.001). Eight studies reported duration of intensive care requirements for patients with delirium. Patients with delirium did not have significantly longer intensive care unit stays than those without delirium (1.3 days, 95% CI 0.7–2.0, p<0.001).
Delirium increased the risk of discharge to nursing home or institutional care facilities14,28 but was only examined in two studies. In one study of patients with delirium after aortic surgery, 38% were discharged to a nursing home after previously living at home, compared to 11% of patients who did not have delirium (p<0.001). 28 Two studies investigated longer-term patient outcomes. In one study, patients who had postoperative delirium after endovascular aortic aneurysm surgery had poorer physical function, social function and energy at 1 and 6 months after surgery compared to those without delirium. 24 In the other study, residual postoperative cognitive impairment in patients who experienced delirium in hospital was not significantly increased compared to those without delirium at discharge or 3 months post discharge. 20
Complications of delirium
Overall rates of complications, including life-threatening ones such as respiratory dysfunction, cardiac arrest, acute renal failure and surgical revision, were higher in patients with delirium than in those without.14,21,27,28 One study found that patients with delirium were more likely to remove venous or urinary catheters and have catheter site infections than those without delirium. 26
Mortality was not significantly increased in patients with delirium in three of the four studies14,17,21,24 that reported mortality data. Each of these studies measured mortality at different time-points, from peri-operative, at discharge, or at 30 days, thus meta-analysis was not possible.
Discussion
This systematic review demonstrates the high incidence of delirium after major vascular surgery; over a third of patients in some studies experienced postoperative delirium. With one exception, 14 the incidence of postoperative delirium was between 13% and 39%. A number of key prognostic factors were identified for development of delirium after major vascular surgery. Increasing age was the most commonly identified prognostic factor in the studies included and demonstrated a significant association with delirium on meta-analysis. Cognitive impairment, pre-existing depression, hypertension and having open aortic surgery were all prognostic factors for the development of delirium. Patients who experienced delirium were more likely to have an increased length of stay, increased risk of surgical complications, and were more likely to have institutional care needs when discharged from hospital. Risk of bias analysis showed moderate risk of bias in study populations and attrition rates, as well as a lack of adjustment for confounders.
Increasing age was associated with delirium in our study. The association between increasing age and the presence of delirium was seen on meta-analysis of mean differences in age between patients with and without delirium, and also on meta-analysis of age as a prognostic factor for the development of delirium. Increasing age has also been associated with delirium in other types of surgery. 1 Factors such as frailty may have a role in the development of delirium independent of chronological age and warrant further exploration; however, our review did not find frailty was a prognostic factor for delirium in the one study that examined this. 19 Our systematic review found cognitive impairment to be a risk factor for developing delirium, in concordance with other studies of postoperative delirium.1,3,33 As many studies excluded patients with underlying cognitive impairment, a potentially vulnerable group may not have been assessed for the risk and impact of delirium. An elevated ASA score was not associated with delirium but this is most likely due to differences in definitions of significant cut-points for grading severe comorbidities with the ASA score.
This review extends upon an earlier systematic review conducted by Balasundaram and Holmes. 34 Our review includes 15 studies of postoperative delirium following vascular surgery, and also includes meta-analysis and bias assessment. By extending the scope of this review to identify prognostic factors as well as incidence, this study is able to report on factors of clinical relevance to vascular surgical patients at risk of delirium. The emergence of validated tools to assess prognostic study quality has led to advances in the methodology of systematic reviews of prognostic factor studies. Risk of bias was assessed using the QUIPS tool, 8 which to our knowledge has not previously been used in vascular surgery prognostic studies. By using the QUIPS criteria 8 to assess risk of bias and by adhering the MOOSE guidelines, 10 the reliability of our systematic review is enhanced and informed by recent developments in the field of prognosis research methods.
Limitations
There are also limitations. Selective publication is an ongoing issue for meta-analysis of prognostic studies. Kyzas et al.35,36 highlight that the published prognostic literature contains a significant bias towards factors with positive associations, with endpoints associated with the highest association preferentially reported. Furthermore, within individual publications, reporting bias exists with a tendency to report only those factors with positive associations, making meta-analysis difficult due to the lack of non-predictive data. In this study, we have attempted to ensure that all non-significant associations with delirium are reported. We are conscious that by only including studies published in English, it is possible that important studies that were published in languages other than English were omitted; however, it was decided that the risk of selection bias secondary to language was limited after a preliminary review of the literature without language restrictions. Variation in study quality and increased risk of bias from confounders was evident and underscores the need for standardization of methods and data reporting to enable accurate characterization of the impact of postoperative delirium. Dissimilarity in the presentation of results, with different cut-points and measurement methods, reduced the capacity for comparison with meta-analysis. Where meta-analysis of unadjusted mean difference was performed, heterogeneity was high, as is common for meta-analysis of observational studies, 13 reflecting the lack of standardization occurring when study groups are not randomized. On sensitivity analysis, heterogeneity did not affect the association between increased age and the presence of delirium, nor for the association between delirium and increased length of hospital stay. I2 poorly reflects measures of heterogeneity when there are small numbers of studies included, which limits the assessment of heterogeneity in this review. For future studies, meta-analysis will be aided by adherence to standardized reporting processes, including measures such as registration of protocols, transparent study methods 37 and publication of results according to guidelines such as the REMARK guidelines 38 that recommend utilizing continuous variables where possible and including confidence intervals along with p-values. Another potential drawback to our review is the assumption that all methods for diagnosing delirium are equally robust; it is beyond the scope of this review to assess the validity of diagnostic tools for delirium. Future studies need to be stringent in assessing and adjusting for potential confounders to the development of delirium, with specific attention paid to the reporting of measures affecting the onset and outcomes of this condition.
Potential prognostic factors such as postoperative analgesia requirements, 39 anaesthetic choice, 40 psychotropic medication use 41 and environmental factors2,5 affect postoperative delirium risk after general and orthopaedic surgery, but our systematic review found that these potential prognostic factors were not included in the studies of delirium after vascular surgery. Early diagnosis and management of delirium has been shown to decrease duration and severity of delirium episodes, decrease mortality and reduce length of stay in surgery other than vascular surgery.2,42 Treatment protocols and diagnostic criteria for delirium already exist but exploration into the impact of these criteria on clinical decision-making is needed. Improvements in models of care, with greater involvement of geriatricians and multidisciplinary health teams into the postoperative management of delirium patients, may lead to better outcomes.
Conclusion
This review has implications for clinical care of vascular surgical patients. Our review suggests delirium is common and has an impact on length of stay, post discharge care requirements and peri-operative complications. Factors predicting an increased risk of delirium include increased patient age, pre-existing cognitive impairment, diabetes, hypertension and open aortic surgery. While the prognostic factors identified in this systematic review, such as age and comorbidities, are not modifiable, other factors, such surgical or anaesthetic choice, models of care, or pre-optimization of physiological parameters, are potentially modifiable but have not been assessed in vascular surgery. Arguably, these are the most valuable factors to study because of their potential for interventions. Further study into the risks and impact of postoperative delirium should focus upon potentially modifiable factors. Well-designed clinical trials are needed to evaluate the impact that modifying prognostic factors and using therapeutic interventions has on the development and outcomes of delirium.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the primary author, SJ Aitken, is the recipient of the following grants that have supported this research: Royal Australian College of Surgeons Senior Lecturer Fellowship; Sydney Medical Foundation Chapman Bequest for research in cardiovascular disease; Ageing and Alzheimer’s Research Foundation, University of Sydney.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.