
Abstract
We sought to determine if symptomatic cardiogenic limb emboli have a random distribution or if there are demographic or echocardiographic factors that predict site of embolization, limb salvage and mortality. Upper (UE) and lower extremity (LE) emboli were evaluated over a 16-year period (1996–2012). Demographic (age, gender, smoking, medical comorbidities) and echocardiographic data were analyzed to determine predictors of embolic site. All symptomatic patients underwent surgical revascularization. Limb salvage and mortality were compared with Kaplan–Meier analysis. A total of 161 patients with symptomatic cardiogenic emboli were identified: 56 UE and 105 LE. The female-to-male ratio for UE emboli (70%:30%) was significantly higher than for LE emboli (47%:53%, p=0.008). No other demographic factors were statistically different. Upper extremity patients were more likely to have atrial fibrillation (50% vs 29.8%, p=0.028), while LE patients had a higher percentage of aortic or mitral valvular disease or intracardiac thrombus (71.4% vs 52.5%, p=0.038). The 30-day limb salvage was higher for UE compared to LE (100% vs 88%, p=0.008). There was a trend toward higher 30-day mortality in the LE group (14% vs 5%, p=0.11). Survival at 1, 3, and 5 years were similar (UE: 62.2%, 44.2%, 35.3%; LE: 69.1%, 47.5%, 30.3%; p=ns). Upper extremity emboli are more frequent in women and patients with atrial fibrillation. Lower extremity emboli are more frequent in the presence of valvular disease or intracardiac thrombus, and are associated with increased 30-day limb loss and mortality. These findings suggest gender- and cardiac-specific differences in patterns of blood flow leading to preferential sites of peripheral embolization.
Introduction
Acute cardiogenic limb emboli are a rare yet well-recognized source of both upper extremity (UE) and lower (LE) extremity ischemia. Atrial fibrillation has been shown in multiple case series to be a significant risk factor for peripheral emboli.1–4 Intuitively, one might expect the anatomic destination of cardiogenic thrombus to follow a random pattern. McBane and associates identified advanced age and atrial enlargement in patients with atrial fibrillation as risk factors for peripheral rather than cerebral emboli. 5 In this study, we sought to determine risk factors for UE versus LE emboli, and evaluated complications, limb salvage, and mortality based on embolus destination.
Methods
The study was approved by the Oregon Health & Science University Institutional Review Board. Patients who underwent surgical treatment of symptomatic UE and LE peripheral emboli were identified from a prospectively maintained operative database (Microsoft Excel; Richmond, WA, USA). A retrospective review of the identified patients was performed. This was cross-referenced with ICD-9 code 444.21 for UE thromboemboli and 444.22 for LE emboli. Patients were excluded if a suspected or proven non-cardiogenic source of peripheral emboli was identified, such as a proximal atherosclerotic lesion, such that all included patients had either a confirmed or presumed cardiogenic embolic source. As this is an operative database of symptomatic patients, it does not contain asymptomatic patients not referred to our practice who may have been managed conservatively. All symptomatic patients in our institution are referred to the vascular surgery service, so all symptomatic patients during this time period are captured.
For each patient, demographic information (age, sex, smoking, medical comorbidities, medications on admission) were recorded. Of the medical comorbidities, renal insufficiency was defined as a serum creatinine >1.5 mg/dL. Hyperlipidemia and hypertension were defined based on medical record listing or if patients were on medications for these disorders. The remaining patients were defined by listing in the medical record or calculated body mass index. Echocardiographic results were recorded in those in whom this test was performed during their hospitalization. All patients underwent surgical thrombectomy, thrombectomy plus thrombolysis, or bypass procedure, the nature and results of which were recorded. During the study period, primary thrombolysis and anticoagulation without revascularization were not performed by the authors. Follow-up data regarding limb salvage and mortality were obtained from the patients’ electronic medical record (Epic; Madison, WI, USA). Mortality was further confirmed using the Social Security Death Index.
Continuous data are presented as means ± standard deviation for normally distributed data, and median and range if not normally distributed. Categorical data are presented as percentages. Statistical analysis was performed using SPSS statistical software (IBM; Armonk, NY, USA). Continuous data were evaluated statistically with Student’s t-test or Mann–Whitney U-test as appropriate. Categorical data were evaluated with the chi-squared test with the Yates’ correction, or Fisher’s exact test as appropriate. Logistic regression analysis was performed to determine factors predicting upper versus lower extremity embolus location. Limb salvage and survival were evaluated with Kaplan–Meier analysis and log rank testing. Significance was determined at a p-value <0.05.
Results
From January 1996 to December 2012, 161 patients with UE or LE emboli of presumed cardiac origin were identified. Fifty-six patients experienced UE emboli (35 right, 21 left) and 105 experienced LE emboli (42 right, 44 left, 19 bilateral). During the time period, 18 patients undergoing UE embolectomy had a non-cardiac source identified (subclavian or axillary artery aneurysm or atherosclerotic lesion) and were excluded. Sixty patients undergoing LE embolectomy had a non-cardiac embolic source identified (aortoiliac or femoropopliteal aneurysm or atherosclerotic lesion) and were excluded. Forty-eight patients with acute LE ischemia due to bypass graft occlusion treated with either catheter directed thrombolysis or surgical thrombectomy were also excluded. There was one patient who presented with concomitant UE and LE emboli who is included in both groups. There were two patients who had UE and LE emboli at different time points (1 week and 8 years) who are also included in both groups. None of the included patients had emboli in other arterial trees.
Locations of emboli within the involved extremities are shown in Figure 1. The most frequent sites of emboli were the brachial artery in the UE (78.6%) and the superficial femoral artery in the LE (56.2%), although LE emboli were frequent throughout the femoral, popliteal, and tibial distribution. These categories are not mutually exclusive, and many patients presented with emboli in multiple arterial beds. In particular, patients with radial or ulnar thrombus all had brachial artery emboli, and patients with tibial or pedal thrombus also had popliteal emboli. It could not be determined if the more distal thrombus was due to the initial embolus or if it was due to distal clot propagation after the initial embolic event.
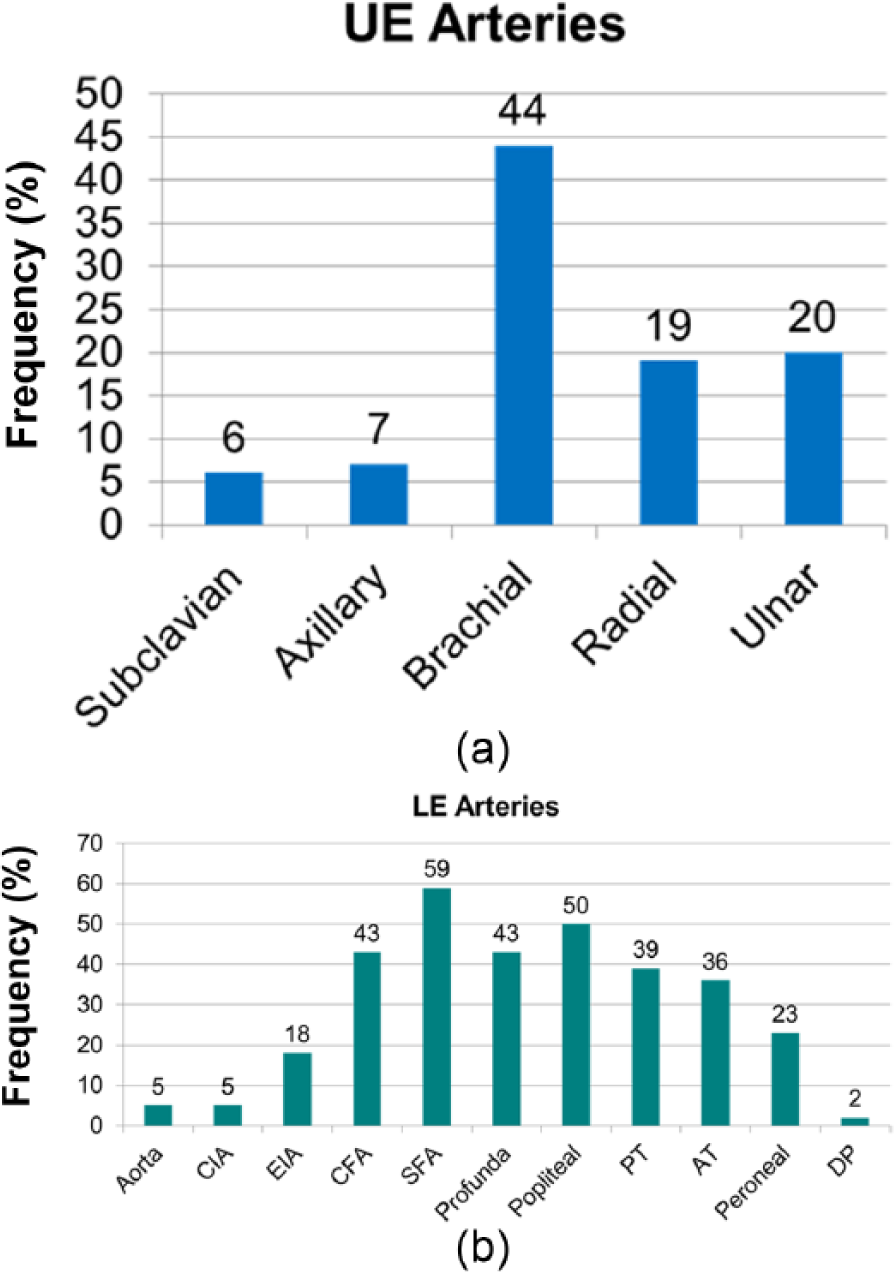
Sites of peripheral embolization in the upper extremity (UE) (1a) and lower extremity (LE) (1b).
Demographic characteristics, pre-admission cardiovascular diagnoses, and medications of the patients are represented in Tables 1–3. Of note, the female-to-male ratio for UE emboli (70%:30%) was significantly higher than for LE emboli (47%:53%, p=0.008) (Table 1). Patients discharged following treatment of UE emboli were more likely to be discharged on warfarin anticoagulation than those with LE emboli (46 (88%) UE vs 67 (72%) LE, p=0.02) (Table 3). No other significant demographic, comorbidity, or medication differences existed between groups.
Demographic characteristics of patient cohort.
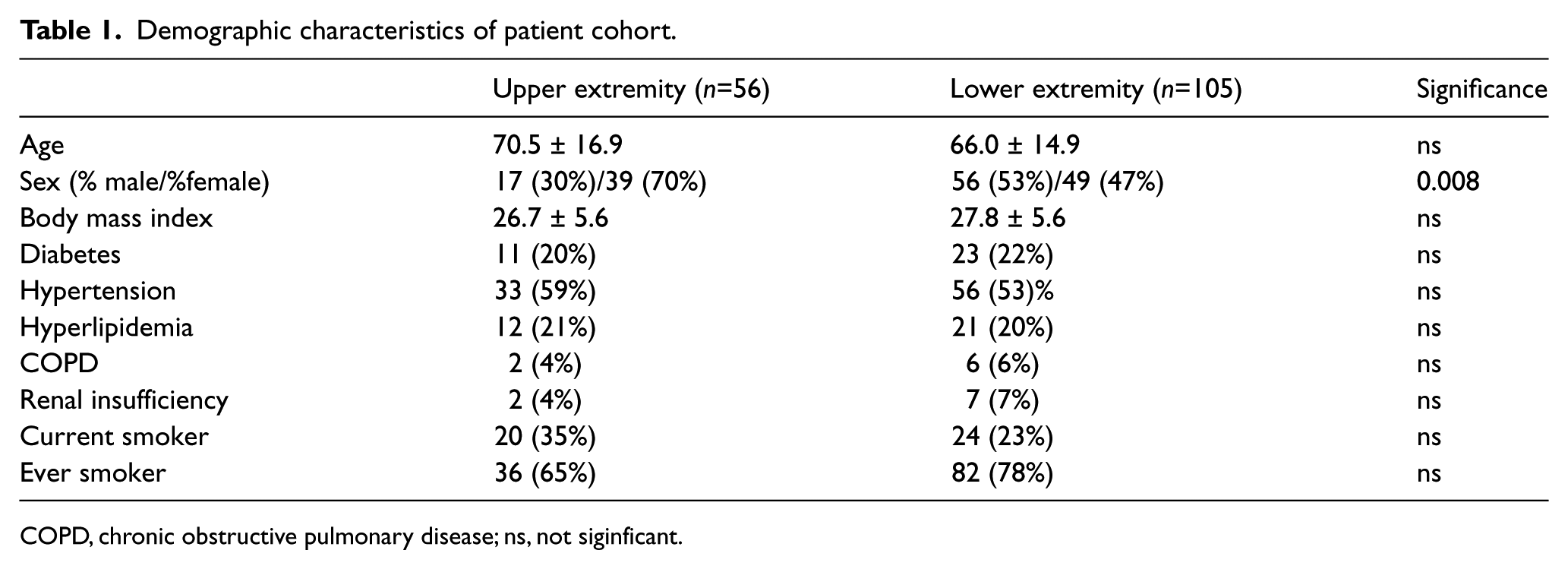
COPD, chronic obstructive pulmonary disease; ns, not siginficant.
Cardiovascular history of patient cohort.
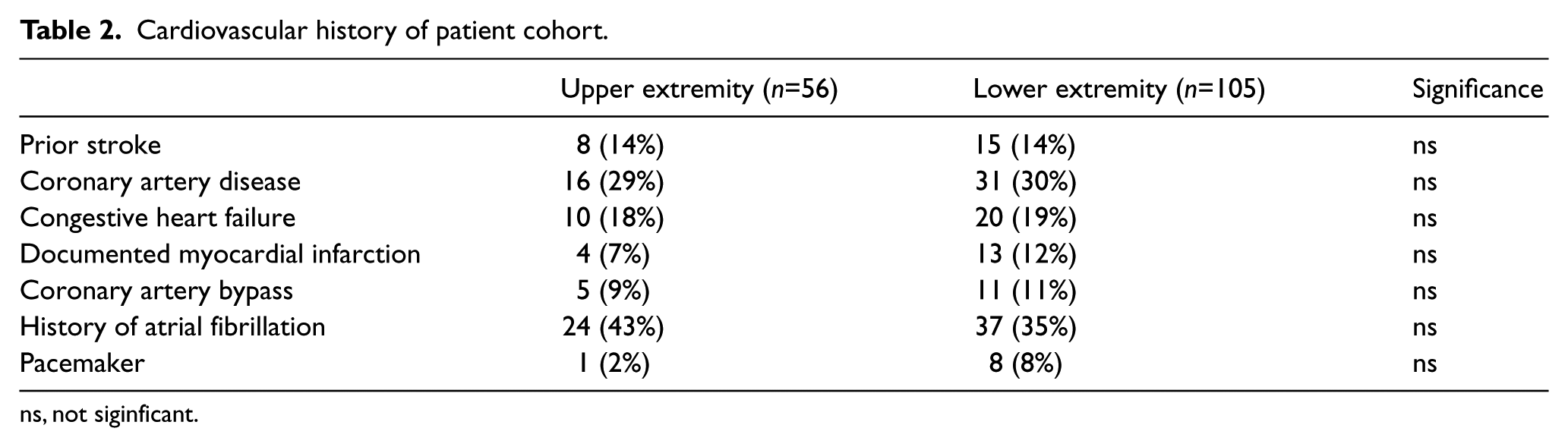
ns, not siginficant.
Admission and discharge medications.
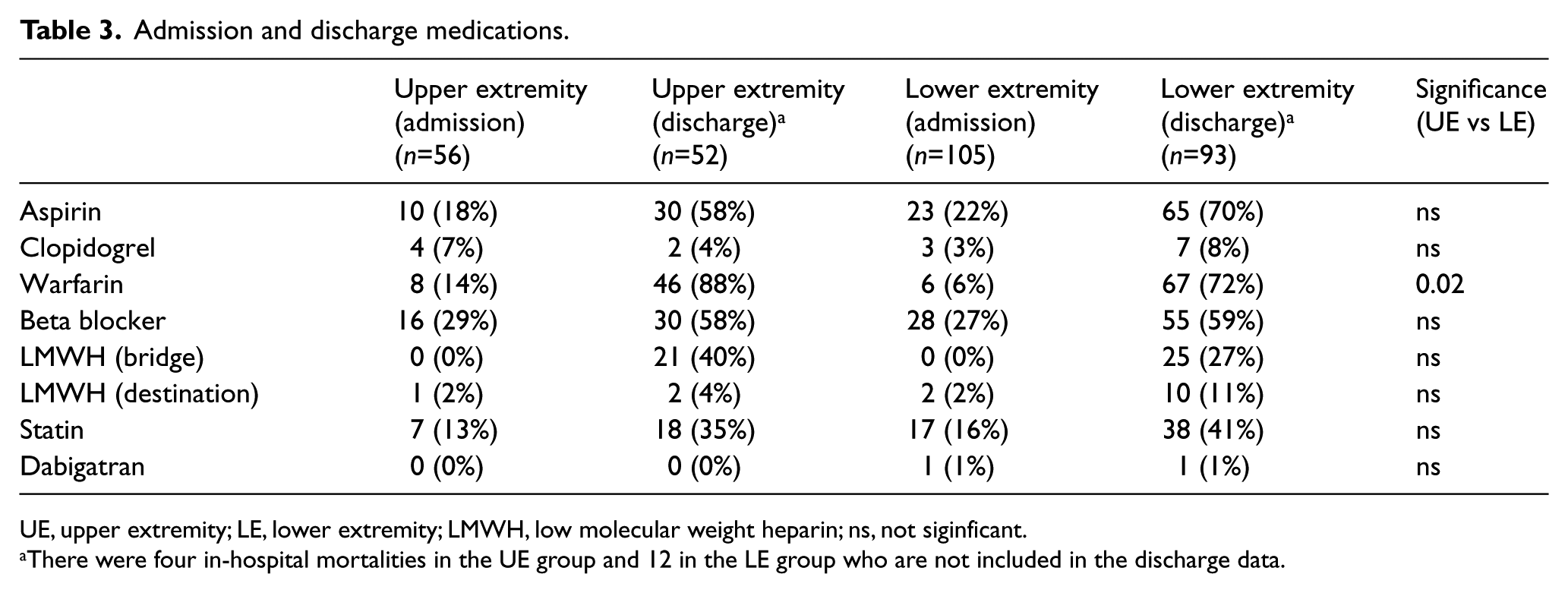
UE, upper extremity; LE, lower extremity; LMWH, low molecular weight heparin; ns, not siginficant.
There were four in-hospital mortalities in the UE group and 12 in the LE group who are not included in the discharge data.
Echocardiographic data were available for 71.4% of the patients with UE emboli and 80.0% of patients with LE emboli, the results of which are reported in Table 4. Transthoracic echocardiography was performed in 112 patients, with transesophageal echocardiography in 13. While the percentage of patients with a prior history of atrial fibrillation was similar between the two groups (Table 2), at the time of embolus diagnosis, a greater percentage of patients with UE emboli were in active atrial fibrillation compared to LE cases (50% vs 29.8%, p=0.028). Numerically, there was a greater percentage of patients with either valvular disease or intracardiac thrombus who presented with LE emboli; however, neither reached statistical significance individually. As a composite endpoint, however, a significantly greater percentage of patients with LE emboli had either valvular disease or evidence of intracardiac thrombus compared to UE cases (71.4% vs 52.5%, p=0.038). By logistic regression analysis, only female sex was a significant predictor of UE versus LE embolus location (odds ratio (OR) 2.62, 95% confidence interval (CI) 1.28–5.35, p=0.008).
Echocardiography results.
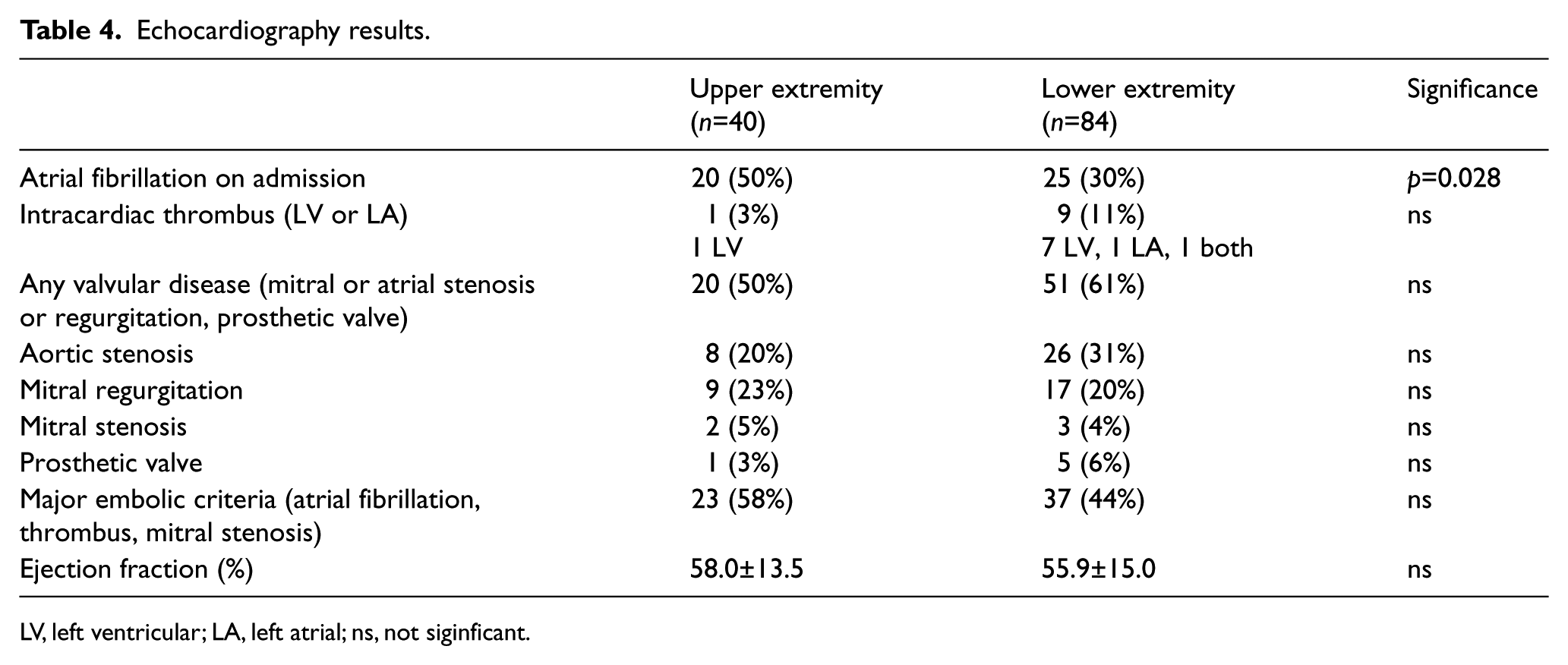
LV, left ventricular; LA, left atrial; ns, not siginficant.
The initial attempt at revascularization was by embolectomy in 100% of UE cases and in 96.2% of LE cases. Supplemental bypass was performed in 7.1% of UE cases and 10.5% of LE cases. Bypasses were only performed when thromboembolectomy was incomplete, typically due to the presence of more chronic thrombus that could not be adequately removed, and limbs were still felt to be ischemic. Intraoperative thrombolysis was employed in 3.6% of UE and 7.6% of LE cases, typically with the goal of improving outflow in patients with distal thrombus propagation. Fasciotomies were performed in only one UE case (1.8%), but were frequently performed in LE cases (31/105 (29.5%), p<0.0001 compared to UE). In the one UE case, the fasciotomy was therapeutic for compartment syndrome that developed after embolectomy. In the LE cases, 29 (94%) were performed at the time of initial surgery, either due to frank compartment syndrome or muscle necrosis, or due to the length of ischemic time. Two patients (6%) were taken back to surgery for delayed fasciotomy due to development of compartment syndrome.
Perioperative morbidity and mortality are presented in Table 5. Wound hematomas were more frequent following UE procedures (19.6% vs 7.6%, p=0.04), possibly due to the increased number of fasciotomies in the LE group, with the subsequent open wound being less susceptible to hematoma formation. Minor amputations (partial or complete phalangectomy) were equally prevalent in both groups (5.4% UE, 4.8% LE). Major amputations (proximal to wrist or ankle) were more frequent following LE embolectomy (11.4% vs 0%, p=0.009). Of the 12 amputations in the LE group, five were performed immediately at the time of initial operation due to extensive myonecrosis, six were performed in patients who underwent fasciotomies at the time of initial operation but were noted to have myonecrosis that progressed postoperatively, and one patient developed foot gangrene and infection despite having viable calf muscles not requiring fasciotomy. There was a non-significant trend for increased perioperative mortality following LE embolectomy (14.3% vs 5.4%, p=0.11).
Perioperative (<30 day) morbidity and mortality.
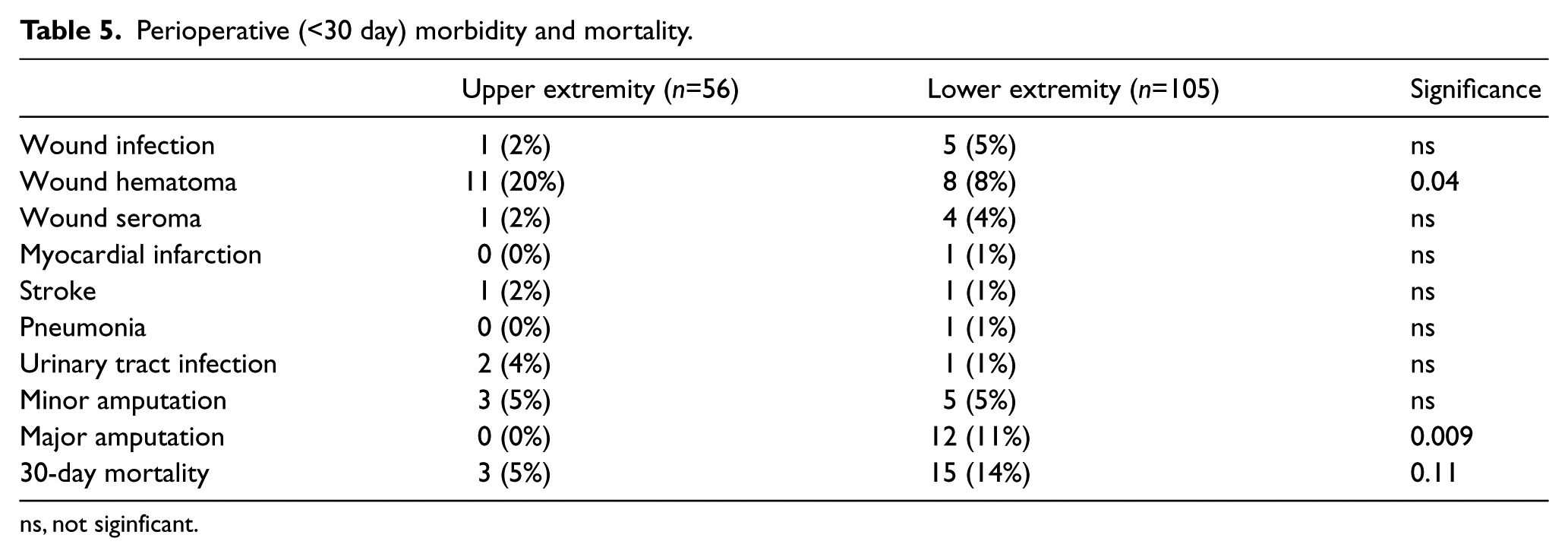
ns, not siginficant.
Overall median follow up was 5.0 months (range 0–195 months), and was the same for UE (5.5 months, range 0–188 months) and LE (4.0 months, range 0–195 months). No further amputations were performed outside of the perioperative period. Survival at 1, 3, and 5 years was not statistically different between UE (62.2%, 44.2%, 35.3%, respectively) and LE (69.1%, 47.5%, 30.3%, respectively) patients (Figure 2).
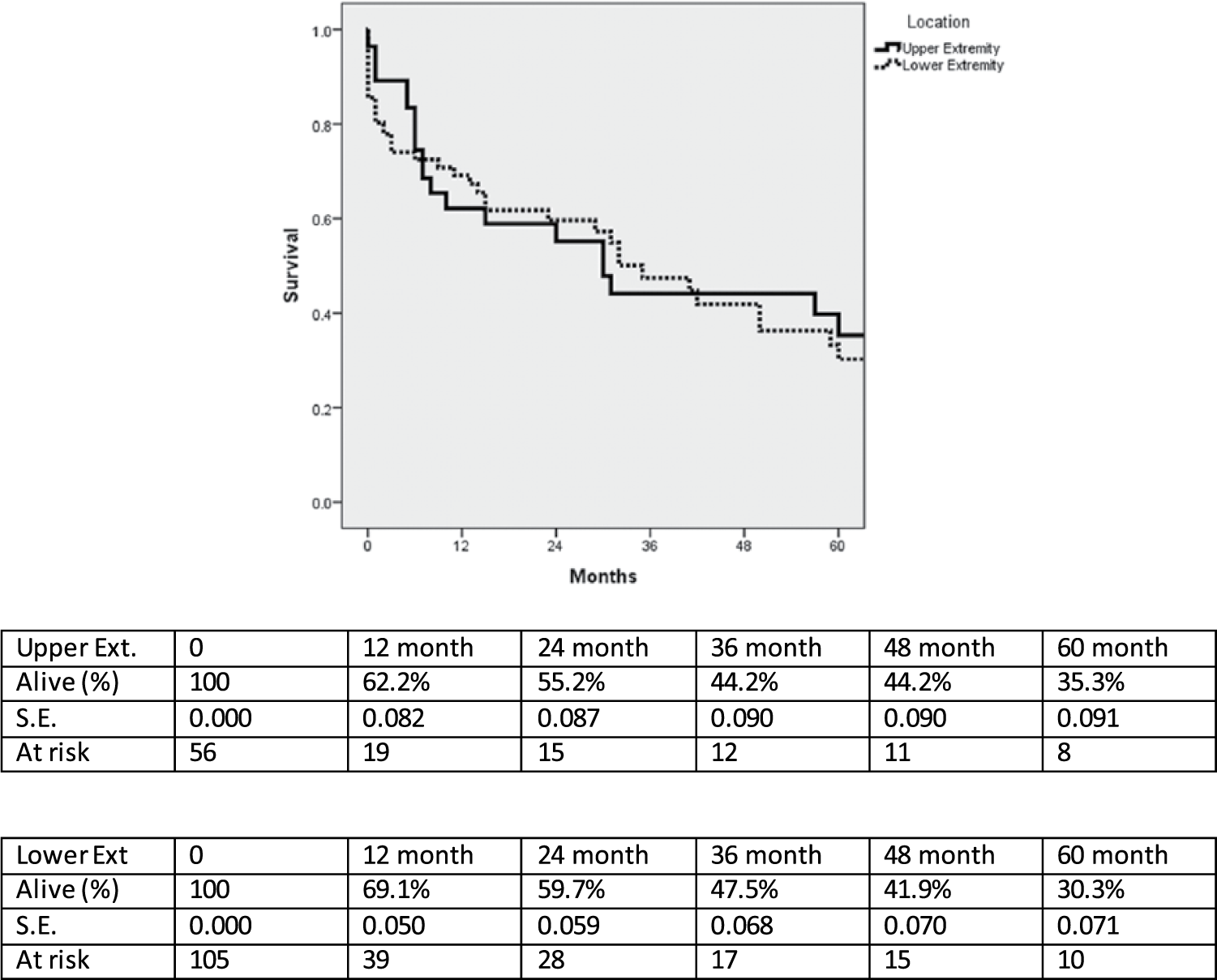
Kaplan-Meier survival curves for patients with upper and lower extremity emboli. SE, standard error..
Discussion
In this study, results of the work-up and treatment of patients with peripheral emboli at a single institution over a 16-year period were reviewed. We sought to determine what factors might predict the anatomic location of emboli. While there were no specific factors that seemed to predict LE emboli, female sex and active atrial fibrillation were more likely to be associated with upper extremity emboli.
Echocardiography has been extensively evaluated as a diagnostic method in patients with cardiogenic emboli, most often in the setting of embolic stroke.6–8 High-risk findings on echocardiography include atrial fibrillation, left ventricular aneurysm, cardiomyopathies, cardiac masses, mechanical valves, and mitral valve stenosis. Minor findings or findings of unclear significance include mitral valve prolapse, aortic stenosis, patent foramen ovale, and atrial septal defect. Using these criteria, major embolic findings were present in 57.5% of patients with UE emboli and 44.1% with LE emboli (p=ns) in our patient population, with 42.5% of UE and 55.9% of LE patients having either low-risk or normal echocardiograms.
Our data on embolectomy outcomes are similar to those in the literature, including studies dealing primarily with UE,1,3,9,10 LE 11 and UE and LE12–14 emboli. As noted, atrial fibrillation is a universally recognized risk factor. The frequent need for fasciotomies and the approximately 5–15% amputation rate have been reported by others.12–14 In contrast, the need for fasciotomies and amputations is rare in UE emboli. None was required in our series. In the National Cohort Study in Denmark, 30-day upper limb amputation rates following upper extremity emboli were 2.0% in males and 2.2% in females. 9 This likely reflects the increased collateralization as well as more straightforward embolic burden of the UE in which the majority of thrombi are localized to the brachial artery, as opposed to the LE in which widespread femoral, popliteal, and tibial involvement is often seen. Furthermore, while we typically treat symptomatic patients surgically, many patients with UE emboli can be managed non-surgically. 15
This study points out the poor survival of this patient population, with 1-year survival of approximately 2/3 and 5-year survival of approximately 1/3. The high mortality of this group is in line with other studies, likely reflecting the advanced age and comorbidities of this patient population.9,10,16 Mortality may be related to another significant finding of this study, namely, the inadequate medical therapy of patients upon their initial presentation despite a high cardiovascular risk profile. Very few patients were taking antiplatelet therapy, anticoagulation, statins or beta blockers at the time of their presentation. This finding is consistent with numerous other studies that have demonstrated suboptimal medical management of patients with cardiovascular and peripheral vascular disease.17–20 This points to a potential area of improvement in the health care system in general – in the optimization of preventive care in this patient group. This will potentially change the natural history of this disease, both with respect to incidence and survival.
Postoperatively, we attempt to anticoagulate all patients, particularly those with echocardiographic findings warranting this. Warfarin use at discharge was more frequent in the UE group. While this is largely due to physician preference and judgement, reasons for not using warfarin therapy included use of low molecular weight heparin therapeutically (2 UE, 10 LE), use of dual antiplatelet therapy (aspirin and clopidogrel: 1 UE, 7 LE), no anticoagulation due to high bleeding risk relative to anticoagulation benefit (3 UE, 13 LE), and patient refusal to be anticoagulated (2 UE). The high hematoma rate in the UE group has led to changes in our approach. We previously continued anticoagulation immediately postoperatively to prevent further embolic episodes. We now delay anticoagulation at least 6 hours postoperatively to allow good wound hemostasis, and have not noticed any adverse re-embolic episodes with this strategy.
The reason for the increased incidence of UE emboli in women is not clear. There are known anatomic differences in aortic arch anatomy between men and women that are accentuated with aging. For example, the diameter of the ascending aorta increases with age and with male gender. 21 Aortic length also increases with age, although this does not appear to be sex-related. 22 However, aortic wall stiffness is greater in women than in men, which dramatically increases after menopause. 23 This may play a role in the increase in cardiovascular disease in general in postmenopausal women, in which a curvilinear increase is noted in comparison with a linear increase noted in men. 24 Sex differences are also present in atrial fibrillation, with females tending to be older, more symptomatic, and more likely to have paroxysmal atrial fibrillation than males. 25 In a recent meta-analysis, female sex was noted to be a significant risk factor for stroke in patients with atrial fibrillation (OR 1.3, 95% CI 1.15–1.49). 26 If and how these sex-related differences affect sites of peripheral embolization is not clear, but it can be hypothesized that the structural or rhythmic differences between men and women may create different flow dynamics or clot size which lead to preferential sites of embolization. It is also, however, possible that sex differences do not really exist but that women more often undergo surgery for UE emboli, due perhaps to increased arterial size and collateralization in men leading to a less symptomatic state.
Limitations
This paper has several weaknesses. The sample size is small, so testing for comparisons may be underpowered. Furthermore, both the UE and LE groups had significant loss to follow-up within the first year, making conclusions beyond 1 year difficult. As a retrospective study, the decision for performing transthoracic echocardiography and in proceeding to transesophageal echocardiography was not regimented. In general, if transthoracic echocardiography was deemed definitive no further imaging was obtained. Transesophageal echocardiography was performed when transthoracic echocardiography was felt to be unclear or with subtle findings (e.g. ventricular enlargement, wall motion abnormalities) without associated thrombus that were felt to be better elucidated with transesophageal echocardiography. Furthermore, data from the earlier patients in the study predate the use of an electronic medical record, and some of the echocardiographic data in these patients may have been lost with the transition to an electronic medical record. As with many studies that have examined cardiogenic emboli, a specific echocardiographic source is not always found. It is possible that, in some cases, emboli were due to another idiopathic cause; however, computed tomography (CT) imaging was performed in all patients to rule out an obvious proximal arterial source. Owing to the paroxysmal nature of atrial fibrillation, it is possible that some patients may have had atrial fibrillation at the time of embolization that had resolved at the time of echocardiography, and were therefore miscategorized. The relationship between emboli and thrombophilia was not specifically evaluated in this study, and in the early portion of the study, was infrequently tested. This is a topic of ongoing investigation in our Division that we are currently attempting to evaluate prospectively. We chose to focus on emboli to the upper and lower extremities; cardiogenic stroke was not evaluated as this is generally not managed by our Division at our institution. Other peripheral embolic locations, such as the renal and visceral vessels, were also not specifically evaluated as they were infrequent occurrences during the study period.
A further limitation of this study is the potential to have missed asymptomatic or minimally symptomatic patients not referred to our practice, as well as patients who may have undergone non-operative therapy (e.g. thrombolysis). As noted, all symptomatic patients presenting to our hospital are referred to our service. While there is evidence to suggest that some UE emboli can be managed conservatively, we routinely revascularize all such patients. Upper extremity embolectomy is a relatively straightforward procedure that can be performed under local anesthetic. Additionally, our policy in treating symptomatic LE emboli is to treat surgically to minimize overall ischemic times. Thrombolysis, either chemical, mechanical, or in combination, can result in delays in revascularization, although we concede that this has been shown to be an effective method of management in selected patients.
Conclusions
In summary, UE emboli occurred more frequently in women with atrial fibrillation. While there are recognized sex-related anatomic differences in the aortic arch, the reason for this sex predilection is not clear. Lower extremity emboli did not occur with a sex predilection; however, it did occur more frequently in the setting of intracardiac thrombus or aortic or mitral valve abnormalities. As most of these abnormalities are considered low risk (e.g. aortic stenosis, mitral regurgitation), there may be as yet undefined comorbidities that lead to a predilection for LE involvement.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.