
Abstract
Ultrasound screening for abdominal aortic aneurysm (AAA) is recommended for male smokers >65 years of age, but screening rates remain low. If computed tomography (CT) performed for other indications could be considered adequate for screening, one-third of ultrasounds would potentially be unnecessary, and overall screening rates would be substantially higher. The objective of this study was to evaluate the sensitivity of CT imaging of the abdomen for the detection of AAA when performed for other clinical indications. We performed a retrospective study of patients eligible for AAA screening who had undergone an abdominal ultrasound as well as an abdominal CT scan for other indications within 3 years prior to that study. The primary outcome was identification of an AAA, recorded in the findings narrative or impression of the CT scan report. Of 142 patients with both a CT scan and an AAA on ultrasound, 127 (89.4%) were noted to have an AAA in the report of a CT scan performed within the 3 years prior to the ultrasound. An additional 10 films demonstrated an AAA that was not mentioned in the report. The sensitivity of pre-existing CT scans for AAA screening was 97.2% (137/141) [95% CI: 93.4–99.0%]; 123 (86.6%) of these positive findings were reported in the findings narrative and 120 (84.5%) were reported in the radiologist’s final impression. The sensitivity for AAA identification in the report of a pre-existing CT scan of the abdomen performed for alternate indications appears high enough to use as a screening test. When radiologists note an AAA, they should be sure to include it in the final impression.
Keywords
Introduction
In 2005, the United States Preventative Services Task Force (USPSTF) recommended one-time abdominal aortic aneurysm (AAA) ultrasound screening for all men aged 65 to 75 years who had ever smoked. 1 In June 2014, revised guidelines were published adding to this selective screening of men aged 65 to 75 those who have never smoked. 2 Screening for AAA with abdominal ultrasound is nearly 100% sensitive and specific for detecting AAA in asymptomatic patients.3–7 This is important because a ruptured AAA confers a mortality of 90% 8 and data from randomized trials demonstrate that screening can reduce AAA-related mortality by 50%.9,10
Prior to the revision of the USPSTF recommendations, ultrasound screening rates were noted to be low, ranging from 2.5% to 12.9%, even though insurance coverage for screening has been mandated during the Welcome to Medicare Physical under the Medicare Screening Abdominal Aortic Aneurysms Very Efficiently (SAAAVE) Act of 2006.11–14 However, reported rates generally consider only screening with designated ultrasound. If other forms of imaging of the abdomen computed tomography (CT), magnetic resonance imaging (MRI), other ultrasound) ordered for other purposes are also considered, then screening rates exceed 40%. 14
CT is generally considered highly sensitive for AAA,15,16 and abdominal imaging locates an incidental AAA in 1–2% of studies.17,18 If CT and other abdominal imaging performed for other indications could be considered adequate for screening, as many as one-third of ultrasounds would be unnecessary, and overall screening rates would be substantially higher. 14 However, it is unknown if these studies adequately report incidental AAAs in a reliable manner. The purpose of this study is to determine the sensitivity of AAA reporting in the full radiologist report and the final impression.
Methods
We performed a retrospective chart review of patients who were seen in 2007 or 2012 by a primary care physician (Internal Medicine or Family Practice) at a single institution and met the 2005 USPSTF criteria for AAA screening. These patients were identified through a search of the electronic health record. The electronic health record was queried for all ultrasound and CT scan studies of the abdomen completed after the age of 50, performed for any indication. For all patients who had undergone an abdominal ultrasound in our vascular laboratory, presence of an AAA and size were available from a pre-existing database. AAA was defined as an anterior-posterior or transverse aneurysmal dilation of the aorta below the diaphragm measuring ≥3.0 cm. We included all patients who were eligible for AAA screening who had undergone a first ultrasound in the vascular laboratory and had also had a CT scan within 3 years prior to that study. Patients were excluded if they had a known history of AAA or AAA repair noted in the chart.
The primary outcome was identification of an AAA, recorded in the body or impression of the CT scan report, noted on manual review (NA).
For patients with a positive AAA ultrasound and no AAA noted on the preceding CT scan report, the CT scan was reviewed by a single radiologist (JJ) to confirm the presence or absence of an AAA. The indications for these CT scans were noted in order to determine if studies ordered for certain indications were more likely to result in a missed AAA. A radiologist review was also performed for patients with a positive CT and a negative ultrasound to evaluate for potential over-reading. To avoid biasing the radiologist’s reading, all studies were provided in a blinded fashion, with a 1:1 ratio of control studies that did not contain an AAA. The study was approved by the Cleveland Clinic Institutional Review Board.
Statistical analysis
We assessed the sensitivity and specificity of CT scanning using the vascular laboratory ultrasound finding as a gold standard. The sensitivity was defined as the percentage of AAAs on vascular laboratory ultrasound, which were also present on the CT scan (true positive rate). We also determined the sensitivity of the findings narrative of the radiology report and the sensitivity of the impression contained in the report. Specificity was defined as the percentage of patients without AAA on ultrasound who were found not to have an AAA on CT scan (true negative rate). For sensitivity and specificity, 95% confidence intervals (CIs) were generated using the Jeffreys method. 19
Results
Of the 15,120 patients eligible for screening in 2007 and 22,355 eligible for screening in 2012, our final sample included 265 patients with both CT and vascular laboratory ultrasound, including 142 patients with AAA on ultrasound and 123 without (Figure 1). The sensitivity of the CT scan report for AAA screening was 89.4% (95% CI: 82.9–93.8%); 123 (86.6%) of these positive findings were reported in the findings narrative of the report and 120 (84.5%) were reported in the radiologist’s final impression.
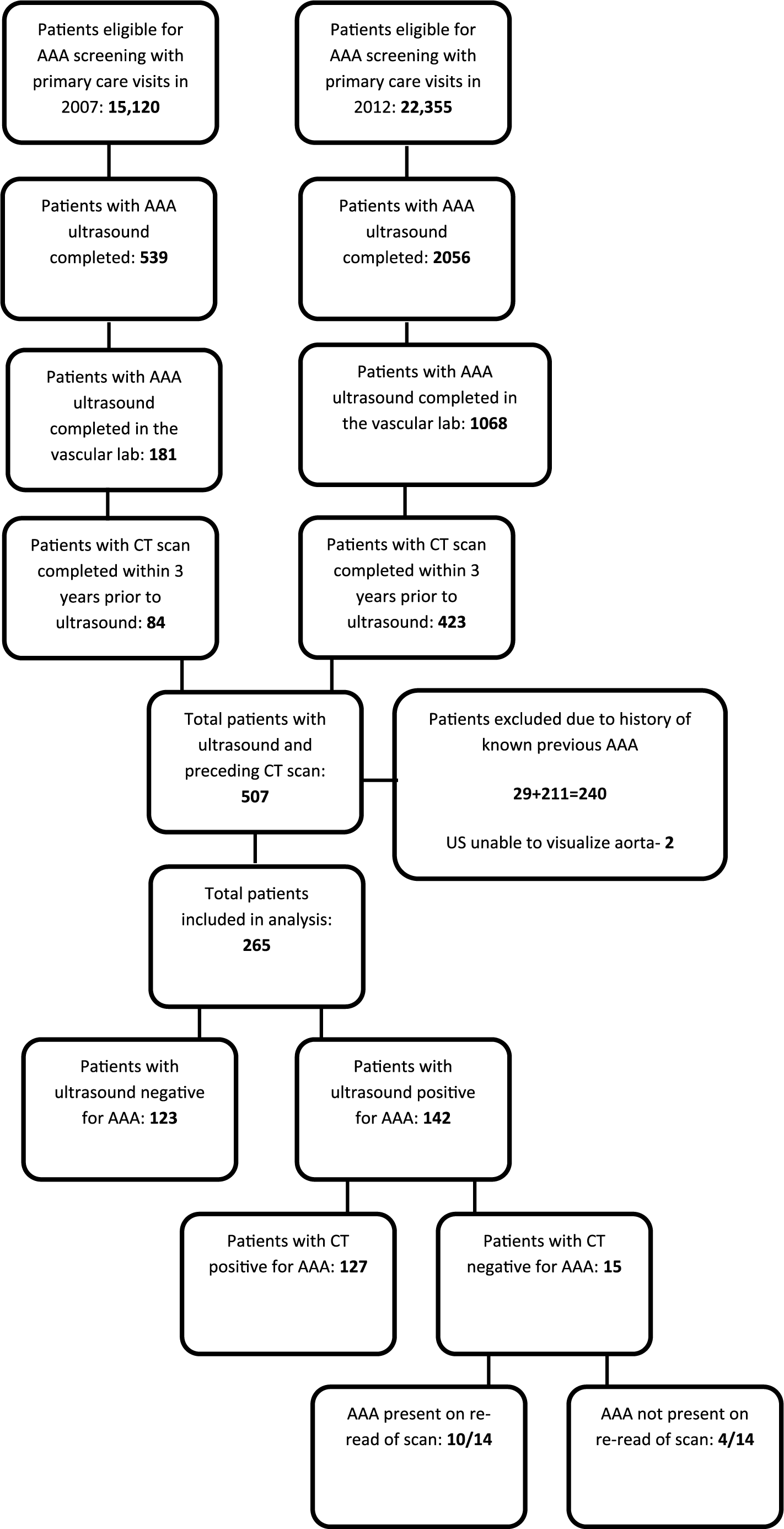
Flow diagram of patient selection. AAA, abdominal aortic aneurysm.
Of the 15 discordant studies in which the ultrasound demonstrated AAA but AAA was not mentioned in the CT report, 14 images were available for review. Ten of these were noted to have a visible AAA on the scan. Figure 2 demonstrates one such aneurysm, seen both on non-dedicated CT and ultrasound. Thus, the overall sensitivity of the CT scan to detect an AAA compared to ultrasound was 97.2% (10+127/141) [95% CI: 93.4–99%]. Indications for these studies included abdominal pain (6/15), concern for cancer (3/15), renal failure (1/15), abdominal distension (1/15), and diarrhea/hypotension (1/15). The specificity of the CT report compared to ultrasound was 97.6% (120/123) [95% CI: 93.6–99.3%]. On reviewing the discordant studies, 2/3 false positive readings were determined not to represent an AAA. Therefore the overall specificity of the CT scan itself was 99.2% (122/123).

Computed tomography (CT) and ultrasound images of an abdominal aortic aneurysm in a 78-year-old woman. A CT scan of the abdomen was initially performed for cancer staging purposes.
Of the 10 AAAs missed on the CT scan, all were <4 cm in the largest dimension. Thus, sensitivity for identifying an AAA was 88/98 (89.8%) if 3–4 cm and 100% if >4 cm. The size distribution of AAAs that were initially seen on non-dedicated CT scans are demonstrated in Figure 3.
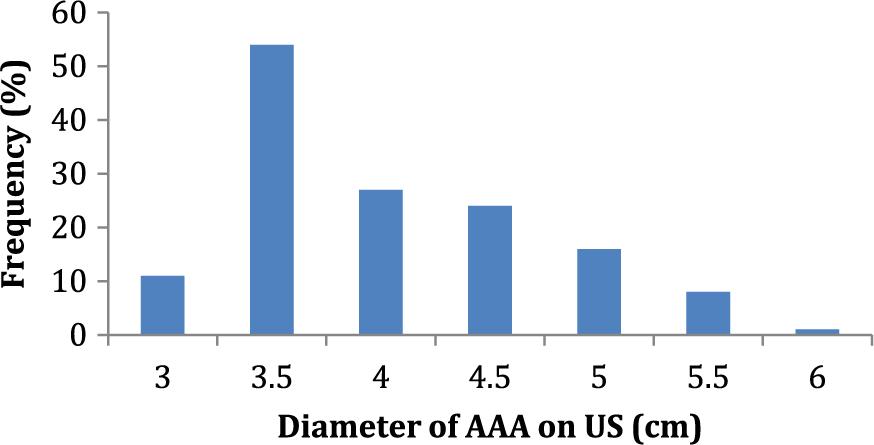
Distribution of abdominal aortic aneurysm (AAA) sizes initially noted on non-dedicated computed tomography scans.
Discussion
In this retrospective study, abdominal CT scans not ordered for detection of AAA had a sensitivity of 97.2% when compared to dedicated ultrasounds for detection of AAA. The sensitivity of the CT findings narrative was lower, and the sensitivity of the impression slightly lower than that; even so, 85% of AAAs could be detected solely by reading the impression of a previous CT report. In contrast, the sensitivity of designated screening ultrasound for AAA is reported to approach 100%, with 1–3% of studies unable to visualize the aorta due to obesity and/or bowel gas.3–7 Given the low rates of AAA screening noted in previous studies and the frequent use of abdominal imaging for other reasons, physicians could greatly increase screening rates by simply reviewing reports of any CT scans performed within the preceding 3 years. The sensitivity of the report should be sufficient for screening purposes, especially if the physician reviews the entire report, not simply the final impression. In particular, the sensitivity for large AAAs, defined as >4.0 cm, was 100%, so patients with a negative CT report would have a very low probability of a clinically significant AAA.
Most positive findings were reported in the impression, but 5.5% (7/127 results) appeared only in the findings narrative of the report. Therefore, in order to realize the full value of previously performed CT scans in AAA screening, physicians need to review the entire report, which may be challenging in a busy primary care practice. At the same time, relying on the CT to rule out AAA without reading the complete findings narrative could pose liability issues. To mitigate this threat, healthcare systems may choose to standardize CT scan readings, such as with structured reporting, to ensure that any AAA is noted in the summary or impression.
Of the patients with an AAA and a negative CT scan report, the AAA was nevertheless visible in 71% of the images, so that the scan itself had a sensitivity of 97%. Although the false negative rate of the reports could be considered acceptable for a screening examination, it could be improved if radiologists specifically evaluated for AAA while reading all abdominal studies. This practice would take additional time and may not be cost-effective, especially given the low prevalence of AAA in the general population. Limiting such readings to men over the age of 65 might be more reasonable, but may fall outside of the scope of standard practice for most radiologists and institutions.
Three patients in our dataset had a CT report describing a small AAA followed by a negative screening ultrasound sometime later. On radiologist review, no AAA was seen on two of these scans. According to the 2009 Society for Vascular Surgery guidelines and the 2005 American College of Cardiology/American Heart Association guidelines, aneurysms between 2.6 and 2.9 cm only require surveillance every 5 years. Therefore, this small percentage of ‘over-reads’ would not result in a burdensome amount of surveillance.20,21
Limitations
This study has a number of limitations. First, the sample size is small and was limited by the quantity and nature of ultrasound studies done in the vascular laboratory. Given the nature of the Cleveland Clinic as a referral center for cardiovascular care, we may have a higher rate of diagnosed vascular disease than many primary care practices. Additionally, abdominal aortic ultrasounds at the Cleveland Clinic can be performed either by radiology or in the vascular laboratory. Clinicians are more likely to refer to the vascular laboratory when they have a higher clinical index of suspicion for AAA, making these patients higher risk for AAA than a more generalized screening population. It is also possible that some ultrasound studies performed in the vascular laboratory may have been ordered in response to the CT findings. Finally, the vascular laboratory serves specialized vascular medicine and vascular surgery practices which care for patients with vascular disease, including AAA, thus the population is not reflective of a community-based population without known vascular disease undergoing duplex ultrasound screening for AAA. This is seen in the large percentage of ultrasounds positive for AAA, which is far higher than the national prevalence of 1% in men, increasing by 2–4% per decade after age 64,22 –24 and may limit generalizability in a true screening population. However, the focus of this study was to assess the relationship between the CT scans (none of which were carried out for AAA screening purposes) and the subsequent ultrasound, which served as the gold standard. This relationship is likely to hold regardless of the study population assessed. Additionally, this study only evaluated CT scans and did not include other cross-sectional imaging, including MRI. A future study evaluating the sensitivity and specificity of other non-dedicated axial imaging would also contribute to increasing screening rates. Finally, different policies governing radiology reads in varying practices and health systems may affect the formatting and trends in radiology reports at those institutions.
Conclusion
Currently, reported screening rates nationwide for AAA are low and utilizing pre-existing CT scans for screening may be a cost-effective mechanism for increasing screening rates. The sensitivity for AAA identification on pre-existing CT scans suggests that this would be a suitable screening strategy. Incorporating these studies would greatly increase screening rates and could obviate many ultrasounds. If this strategy is adopted, it will be important to ensure practitioners evaluate the entire CT report, not simply the final impression, and that national radiology societies are aware of this development in order to address liability issues for over- and under-reads.
Footnotes
Acknowledgements
The authors would like to acknowledge Nurahn Abouzahra for her work in reviewing the CT scan reports.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.