
Abstract
Patients with lower extremity peripheral artery disease (PAD) have a substantially increased risk for mortality as compared to healthy individuals. We aimed to evaluate the risk for all-cause mortality in PAD patients and in healthy controls during a 10-year follow-up period. Our hypothesis was that the mortality rates at 10 years would differ in diabetic and non-diabetic PAD patients. Our study group consisted of 331 consecutive patients with symptomatic PAD <75 years of age admitted to a tertiary care hospital, including 216 patients without diabetes and 115 with diabetes. Control subjects without atherosclerotic disease were matched to the patients in a 1:1 design by sex, age, and diabetes mellitus status. The outcome measure was all-cause mortality at 10 years. Mortality rates at 10 years were 29% in non-diabetic PAD patients versus 14% in age- and sex-matched non-diabetic controls (risk ratio (RR), 2.31; 95% confidence interval (CI), 1.54–3.47; p<0.001), and 58% in diabetic PAD patients versus 19% in age- and sex-matched diabetic controls (RR, 4.06; 95% CI, 2.67–6.18; p<0.001). Further, PAD patients with diabetes had a significantly increased risk for death within 10 years than did the non-diabetic PAD patients (RR, 2.51; 95% CI, 1.72–3.66; p<0.001). Diabetes was independently associated with outcome, and was the strongest predictor of death in multivariate Cox proportional hazards regression. We conclude that mortality rates at 10 years differ in PAD patients <75 years old with and without diabetes. Our findings suggest that future studies should apply distinct risk assessment strategies in the two PAD subgroups.
Introduction
Lower extremity peripheral artery disease (PAD) is a condition characterized by progressive atherosclerosis involving the arteries supplying the lower extremities.1,2 PAD is a distinct subtype of atherosclerotic vascular disease that differs from coronary artery and cerebrovascular disease in its clinical presentation. 2 The phenomenon of plaque instability in the coronary or cerebral arterial beds leads to acute events, such as myocardial infarction or ischemic stroke. 2 For reasons that are not fully understood, such acute events are relatively rare in PAD, and symptoms most often result from progressive arterial narrowing because of on-going atherosclerosis. 2
Modifiable conditions that predispose to the development and progression of PAD include smoking, diabetes mellitus, arterial hypertension and dyslipidaemia. 1 Because those same ‘classical’ risk factors contribute to the development of systemic atherosclerosis as well, identification of PAD increases the likelihood of coexistent coronary artery and cerebrovascular disease. 1 As a consequence, PAD is associated with an increased risk for ischemic manifestations involving other vascular territories. 1 The most dramatic effect of PAD is impaired survival, with a substantially increased risk for 5- to 10-year mortality as compared to healthy individuals.1,2
As there are only a few published studies on 10-year outcome data in PAD cohorts, we aimed to evaluate the risk for all-cause mortality in PAD patients and healthy controls during a 10-year follow-up period. From our experience with 5-year outcome data in patients with lower extremity PAD, 3 we hypothesized that the mortality rates at 10 years would differ in diabetic and non-diabetic PAD patients. To test this hypothesis we evaluated a cohort of PAD patients aged <75 years from the Linz Peripheral Arterial Disease (LIPAD) study.
Materials and methods
Study design
The LIPAD study was prospectively designed and conducted to evaluate biomarkers for PAD by using a case–control design and to determine the long-term outcome of patients with established PAD.4,5 The study protocol was approved by the local ethics committee in accordance with the Declaration of Helsinki, and all study participants gave informed consent. 5 In PAD patients and controls, the following data were obtained as recommended and as previously described:5,6 history, including evaluation of comorbidities and existing risk factors for atherosclerotic disease; Doppler segmental blood pressure of the lower limbs, including continuous-wave spectral analysis and resting ankle–brachial index (ABI) measurements; and colour duplex ultrasound scanning of the carotid bifurcation and the internal carotid artery. In the controls these data were obtained purely for the purpose of the study. Furthermore, we performed contrast intra-arterial aorto-femoral angiography in all PAD patients at the time of patient recruitment (which is the ‘gold standard’ for defining both normal vascular anatomy and vascular pathology)2,6–9 to confirm the presence of lower extremity PAD and to characterize the site and extent of stenoses and/or occlusions of the lower limb arteries.
Outcome ascertainment
Mortality data for the entire cohort were obtained from the Austrian Mortality Registry, resulting in date of death and cause of death, encoded either before 2002 according to the International Code of Diseases, Version 9 (ICD9), or after 2002 according to ICD10. The Austrian Mortality Registry includes all deaths within Austria and the deaths of Austrian citizens in foreign countries if reported to Austrian officials.
The outcome measure for the present work was all-cause mortality at 10 years. All PAD patients and all controls completed follow-up, and the observation period for each of them was set at 10 years (i.e. exactly 3650 days from the time of enrolment) or until death, if sooner. Cardiovascular mortality was defined as ICD9/ICD10 codes 390–459/I00–I99, and cancer mortality as ICD9/ICD10 codes 140–239/C00–D48. The remaining ICD9/ICD10 codes were summarized as mortality attributable to other causes.
Definitions
Symptomatic lower extremity PAD was defined as specific symptoms (claudication, rest pain or minor or major tissue loss) with the corresponding vascular pathology as determined by intra-arterial aorto-femoral angiography and classified as claudication or critical limb ischemia. The ABI was calculated as the quotient of the higher of the systolic blood pressures measured at the two ankle arteries of each limb (either the anterior tibial artery or the posterior tibial artery) and the higher of the two brachial systolic blood pressures; we used the lower ABI of each limb for further analysis. 7 Early-onset PAD was defined as the beginning of symptomatic PAD at patient age <55 years. Coronary artery disease was defined as a documented history of percutaneous transluminal coronary angioplasty or coronary bypass surgery, as previous acute coronary syndrome (i.e. myocardial infarction or stable or instable angina) or as occult myocardial infarction diagnosed by electrocardiography. 5 Cerebrovascular disease was defined as a history of stroke with permanent neurological deficit or a history of transient or temporary stroke. 5 Arterial hypertension was defined as a systolic blood pressure ⩾145 mmHg, or diastolic blood pressure ⩾90 mmHg, or the use of any antihypertensive medication. 5 Diabetes mellitus was defined as fasting blood glucose levels ⩾126 mg/dL or the use of any glucose-lowering medication. 5
Patients with symptomatic lower extremity PAD
From April 2000 to April 2002 we consecutively enrolled all patients with symptomatic chronic atherosclerotic PAD admitted to a single tertiary care hospital in Austria (Konventhospital Barmherzige Brueder, Linz).3–5 PAD was diagnosed by the vascular surgeon attending during index hospitalization. At that early time it was common practice in the Austrian health system to evaluate all patients with established PAD as inpatients in hospital. Because all patients were enrolled at hospital admission, baseline data were obtained prior to any PAD-specific treatment and/or modification of drug therapy during index hospitalization. As already stated, the study participants were admitted for diagnostics and treatment of significant lower extremity PAD and therefore none of them suffered acute coronary syndrome, acute stroke or acute transient or temporary stroke at the time of enrolment. Exclusion criteria were the history or presence of any malignancy, acute PAD (i.e. acute thromboembolic vascular occlusion) or PAD of non-atherosclerotic causes.3–5 All PAD patients were Caucasian.
The entire LIPAD cohort included 487 consecutive patients with symptomatic lower extremity PAD as described previously.3–5 Patient age at the time of enrolment in the study ranged from 38 to 94 years. As described in the original article on the LIPAD cohort, 5 we stratified the entire cohort into two groups according to patient age. We had 331 individuals <75 years of age (216 without and 115 with diabetes mellitus) and 156 individuals ⩾75 years of age (102 without and 54 with diabetes mellitus). The decision to stratify the entire PAD cohort according to age 75 years was already made before starting patient recruitment and was based on the cut-off point used in a former landmark study on PAD, the Edinburgh Artery Study, that evaluated only individuals <75 years. 10 For the present work we assessed all-cause mortality at 10 years in our PAD cohort and – in keeping with the nature of such a long-term outcome study – we decided to evaluate our 331 PAD patients <75 years of age but not our 156 PAD patients ⩾75 years of age, because we assumed that assessing long-term outcome as a function of having diabetes mellitus versus not having diabetes mellitus in patients aged between 75 and 94 years would not be appropriate.
Control subjects without relevant atherosclerotic disease
From January 2001 to July 2004 we recruited controls matched to the patients with lower extremity PAD in a 1:1 design by age (±2 years), sex, and diabetes mellitus status.3,5 All controls were admitted to a single tertiary care hospital in Austria (Konventhospital Barmherzige Brueder, Linz) because of minor health problems, such as vertebrogenic pain, cataract surgery, and non-arterial surgery (e.g. varicose vein extirpation, herniotomy). All controls were in good health and had the following characteristics: no history or presence of any malignant disease; no coronary artery or cerebrovascular disease according to the above definitions; no previous stenting or vascular surgery of the internal carotid arteries; no stenosis of the internal carotid arteries >50% as assessed by colour duplex ultrasound scanning; no history or current clinical evidence of PAD; no pathological patterns of pulse waves in the legs shown by continuous-wave spectral analysis; ABI ⩾1.0; and no history of venous thromboembolism.3,5 All control subjects were Caucasian.
Biochemical analyses
We collected blood at admission to hospital after overnight fasting by venipuncture. Creatinine, estimated glomerular filtration rate (eGFR), lipid profiles, glucose, and glycohaemoglobin A1c were analysed with appropriate methods, which have been described in detail previously.3,4
Statistical analysis
We displayed dichotomous variables as numbers (and percent) and continuous variables as median (with interquartile range), unless otherwise stated. We computed Kaplan-Meier estimates of the distribution of times from baseline to death and used log-rank tests to compare the survival curves of the patient subgroups or the corresponding controls. We further used univariate Cox proportional hazards regression analyses to evaluate the effect of case–control status and diabetes mellitus status on survival in our cohort. Univariate and multivariate Cox proportional hazards regression analyses were performed to assess a potentially independent effect of diabetes mellitus status on survival in the PAD cohort. For both univariate and multivariate analyses, continuous predictor variables were dichotomized according to commonly used cut-off values in order to achieve risk ratios (RR) for all predictor variables that are comparable to each other with respect to their magnitude. Our data were analysed with MedCalc 13.0.0.0 (MedCalc Software bvba, Ostend, Belgium) and SPSS 13.0 (SPSS, Inc., Chicago, IL, USA). Obtained p-values were not adjusted for multiple comparisons and are therefore descriptive only.
Results
Description of PAD patients and controls
The present cohort included 331 consecutive patients with symptomatic lower extremity PAD <75 years of age and 331 controls matched to the patients in a 1:1 design by sex, age and diabetes mellitus status. Characteristics of patients and controls are detailed in Table 1 according to diabetes mellitus status.
Baseline characteristics and mortality data of the 331 patients with symptomatic peripheral artery disease (PAD) and the 331 controls.
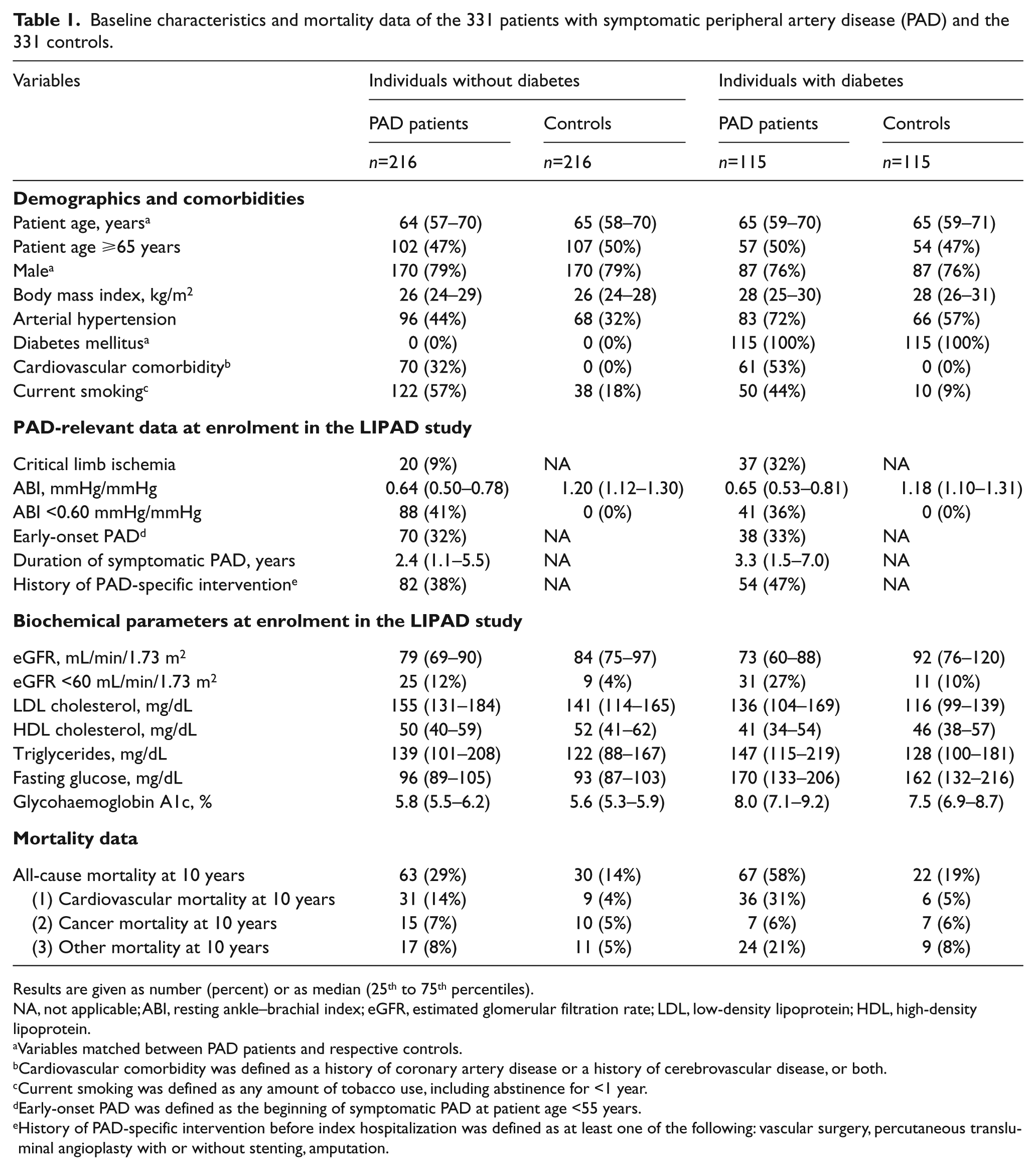
Results are given as number (percent) or as median (25th to 75th percentiles).
NA, not applicable; ABI, resting ankle–brachial index; eGFR, estimated glomerular filtration rate; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Variables matched between PAD patients and respective controls.
Cardiovascular comorbidity was defined as a history of coronary artery disease or a history of cerebrovascular disease, or both.
Current smoking was defined as any amount of tobacco use, including abstinence for <1 year.
Early-onset PAD was defined as the beginning of symptomatic PAD at patient age <55 years.
History of PAD-specific intervention before index hospitalization was defined as at least one of the following: vascular surgery, percutaneous transluminal angioplasty with or without stenting, amputation.
At enrolment, the 331 PAD patients had a median age of 64.2 years (range, 38.2–74.9). Of the PAD patients, 96 had a history of coronary artery disease and 56 a history of cerebrovascular disease, resulting in 131 patients with cardiovascular comorbidity (75 had only a history of coronary artery disease, 35 had only a history of cerebrovascular disease and 21 had both).
Of the 331 patients evaluated, 105 were treated conservatively during index hospitalization, and 226 underwent PAD-specific interventions during index hospitalization (i.e. one or more of the following: vascular surgery, percutaneous transluminal angioplasty with or without stenting, amputation). Two patients died in hospital (both undergoing vascular surgery during index hospitalization).
At discharge from hospital, 262 patients were on antiplatelet therapy (226 on aspirin and 123 on clopidogrel), 70 were taking oral anticoagulation (13 of them in combination with antiplatelet therapy) and 176 received lipid-lowering medication (167 statins, seven fibrates, and two both). Furthermore, 74 patients with diabetes were controlled by diet and oral agents, and 41 were insulin-controlled. With regard to antihypertensive treatment, 48 patients took a single medication at discharge, 56 a combination of two, and 74 a combination of three or more. In detail, 75 patients took beta-blockers at the time of discharge, 124 angiotensin-converting enzyme inhibitors, 11 angiotensin II antagonists, 47 calcium antagonists, 21 alpha-1 receptor blockers, 11 alpha-2 agonists, 20 loop diuretics, 86 thiazide diuretics, and 12 potassium-sparing diuretics.
Mortality data of the PAD patients and controls
Of the 331 individuals with symptomatic lower extremity PAD evaluated in this study, 216 patients did not have diabetes mellitus and 115 did. After a 10-year follow-up period, 63 (29%) of the 216 non-diabetic PAD patients and 67 (58%) of the 115 diabetic PAD patients had died. Thus, PAD patients with diabetes had a significantly increased risk for death within 10 years as compared with the non-diabetic PAD patients (risk ratio (RR), 2.51; 95% confidence interval (CI), 1.72–3.66; p <0.001). Figure 1 shows the survival probability in time course for the 331 PAD patients according to diabetes mellitus status. Each of the survivors had a follow-up period of exactly 10 years, whereas the 63 decedents without diabetes had a median survival time of 6.1 years (range, 0.2–9.8) and the 67 decedents with diabetes had a median survival time of 5.7 years (range, 0.1–10.0). The overall median survival time of the 216 patients without diabetes was 10.0 years, whereas the median survival time of the 115 patients with diabetes was 8.0 years.
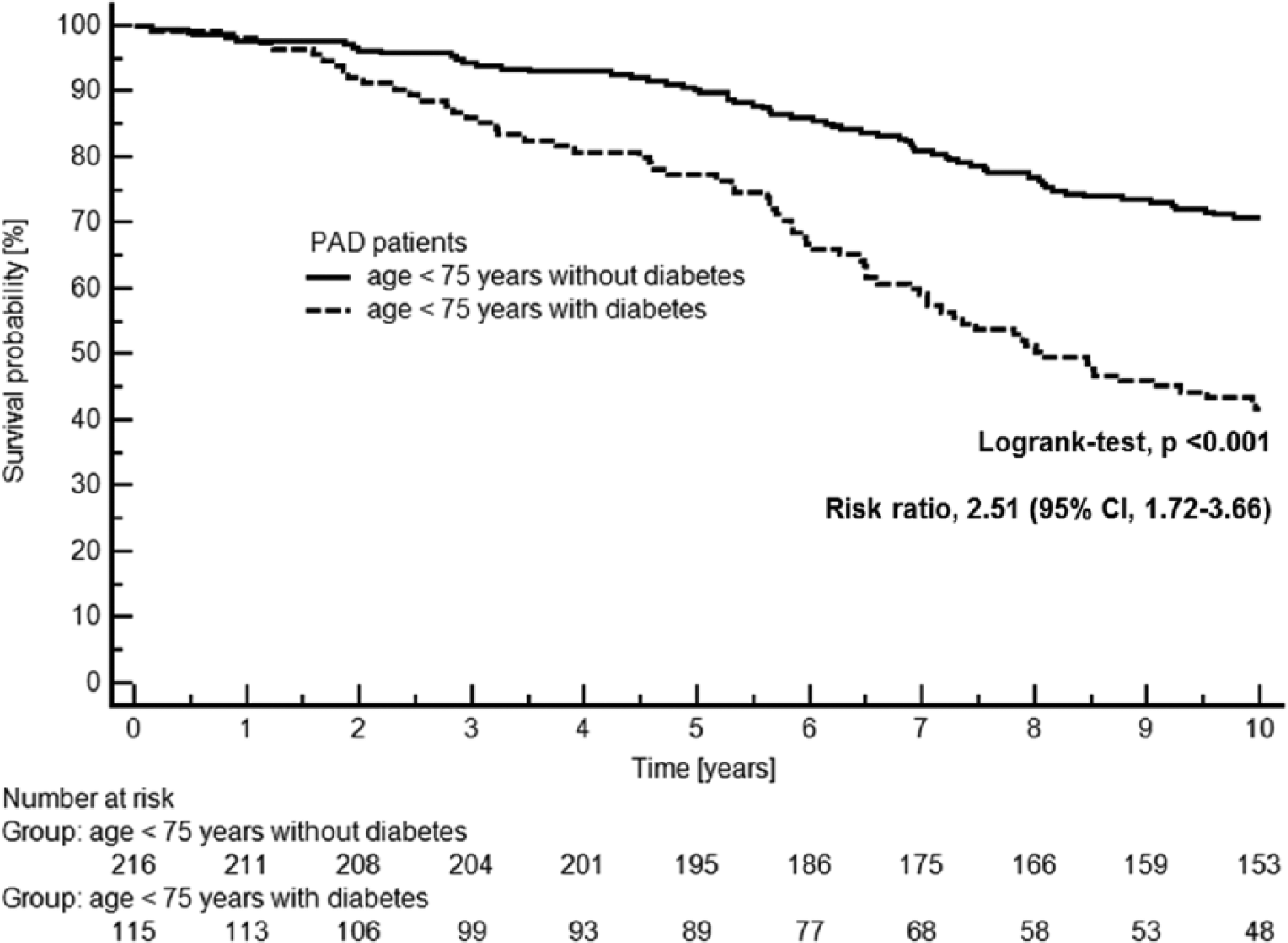
Kaplan-Meier plot showing survival in 331 patients with symptomatic peripheral artery disease (PAD) according to the two patient groups (i.e. 216 patients without diabetes mellitus vs 115 patients with diabetes mellitus).
Figure 2 shows the survival curves for PAD patients versus controls. The 10-year mortality rates were higher in the 216 PAD patients without diabetes versus the 216 age- and sex-matched non-diabetic controls (29% vs 14%; RR, 2.31; 95% CI, 1.54–3.47; p <0.001) and also in the 115 PAD patients with diabetes versus the 115 age- and sex-matched diabetic controls (58% vs 19%; RR, 4.06; 95% CI, 2.67–6.18; p <0.001).
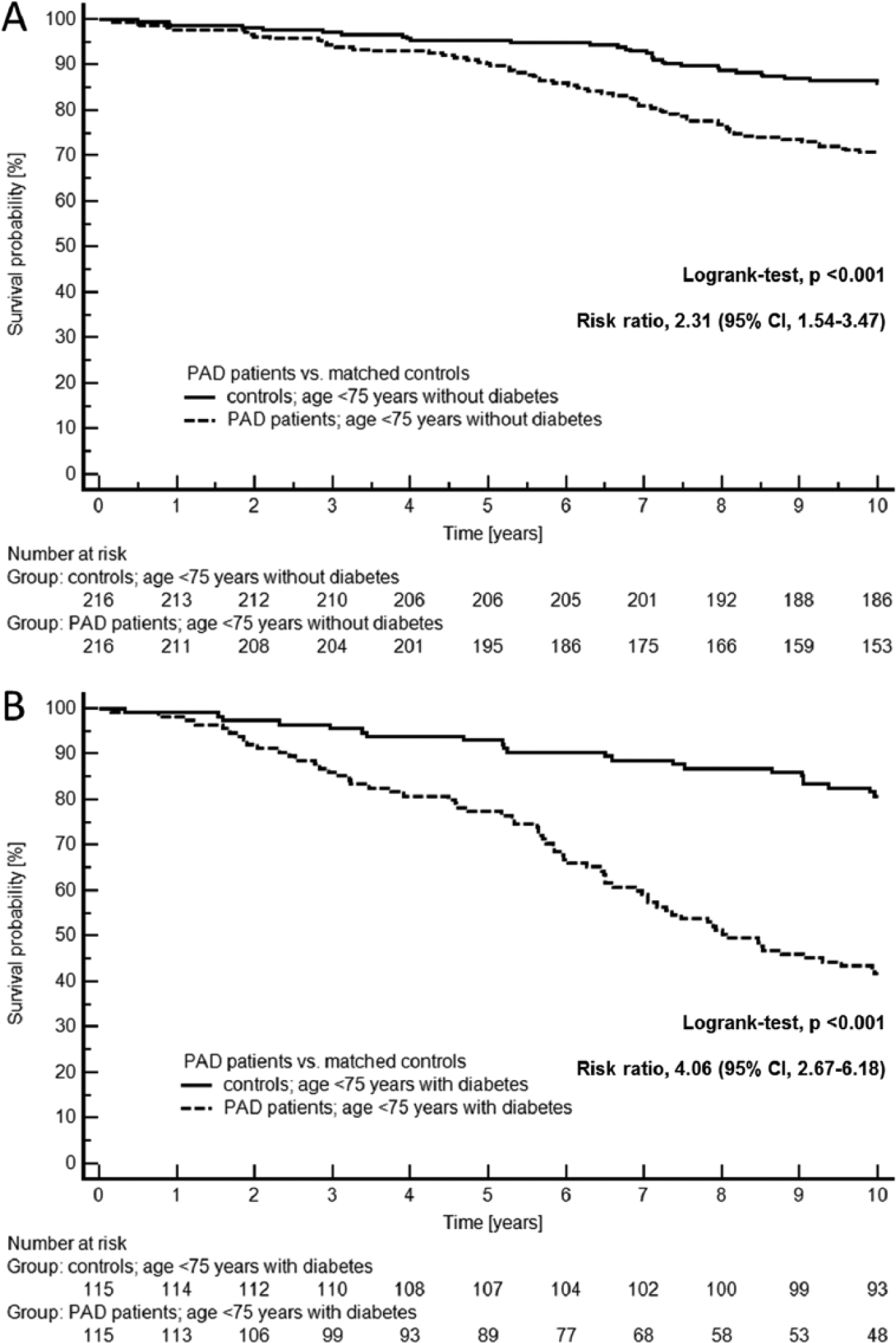
Kaplan-Meier plots showing survival in (A) 216 non-diabetic peripheral artery disease (PAD) patients and 216 age- and sex-matched non-diabetic controls and (B) 115 diabetic PAD patients and 115 age- and sex-matched diabetic controls.
Table 2 summarizes the mortality data for patients with established PAD and for healthy controls. Overall, the 331 patients <75 years of age with symptomatic lower extremity PAD had an approximately threefold higher risk for death within 10 years than did the 331 age-, sex- and diabetes-matched controls (RR, 2.93; 95% CI, 2.13–4.05; p <0.001).
Results of 10-year all-cause mortality in peripheral artery disease (PAD) patients and controls according to diabetes mellitus status.
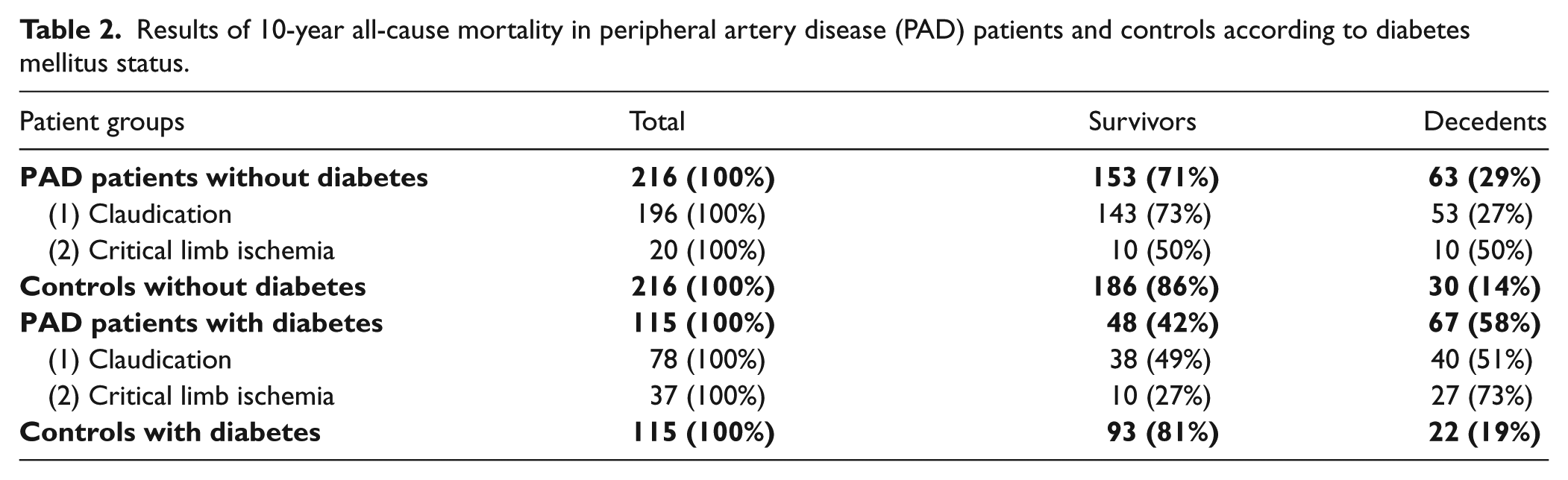
Table 3 gives the results of Cox proportional hazards regression analysing the ability of diabetes to predict 10-year all-cause mortality in our PAD cohort. The table shows that diabetes was independently associated with outcome and was the strongest independent predictor of death among all variables included in the statistical model.
Results of Cox proportional hazards regression analysing the ability of main study variables to predict 10-year all-cause mortality in the entire peripheral artery disease (PAD) cohort (n=331; 201 survivors vs 130 decedents).
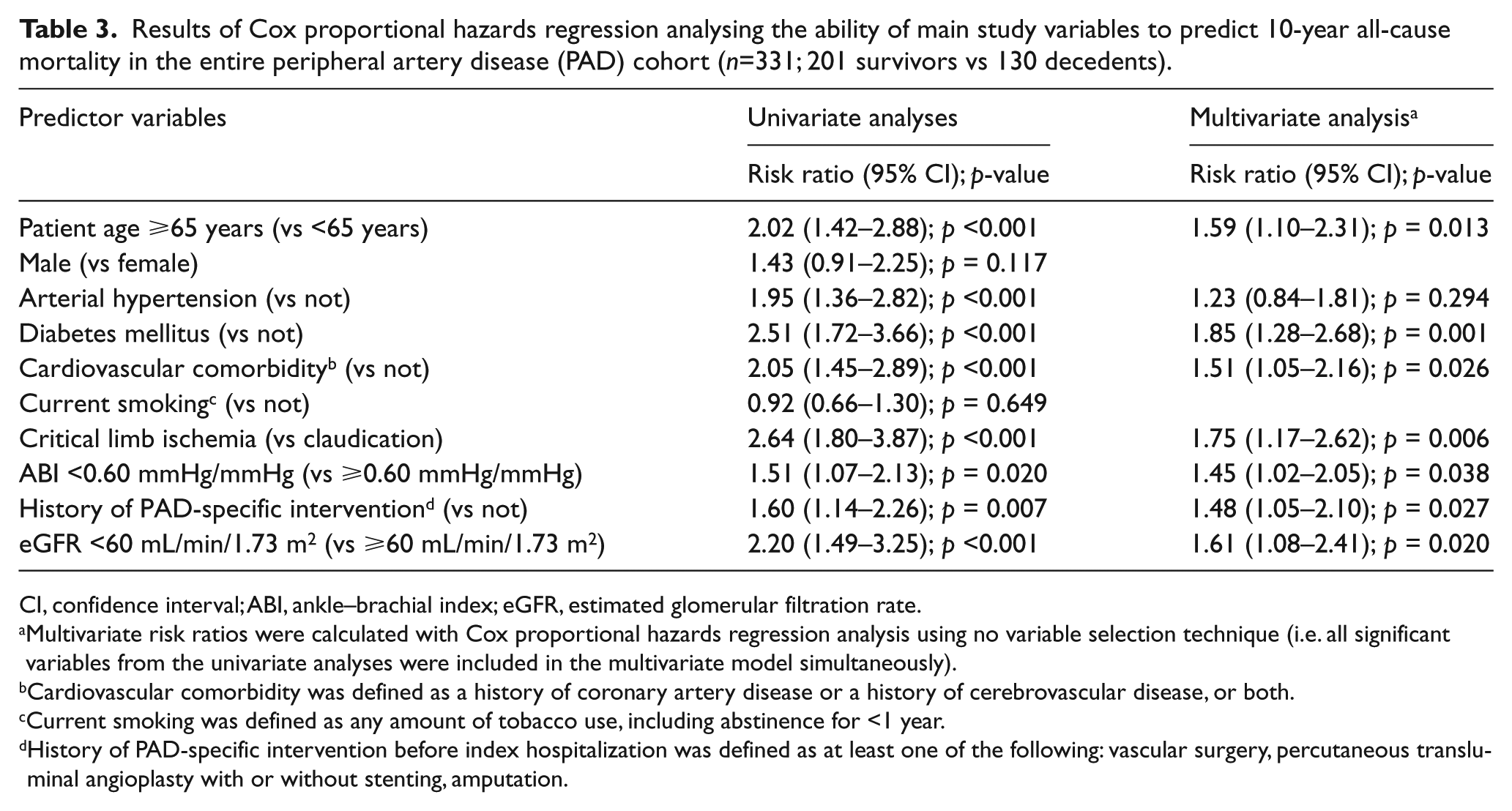
CI, confidence interval; ABI, ankle–brachial index; eGFR, estimated glomerular filtration rate.
Multivariate risk ratios were calculated with Cox proportional hazards regression analysis using no variable selection technique (i.e. all significant variables from the univariate analyses were included in the multivariate model simultaneously).
Cardiovascular comorbidity was defined as a history of coronary artery disease or a history of cerebrovascular disease, or both.
Current smoking was defined as any amount of tobacco use, including abstinence for <1 year.
History of PAD-specific intervention before index hospitalization was defined as at least one of the following: vascular surgery, percutaneous transluminal angioplasty with or without stenting, amputation.
Discussion
The results of our study demonstrate that in symptomatic PAD patients <75 years of age, 29% of the individuals without diabetes and 58% of those with diabetes died within 10 years. The literature reports that patients with PAD have an approximately threefold increased risk for death from all causes within a period of 10 years. 1 Thus, our findings are in line with this evidence because we show that even our 331 individuals <75 years of age with symptomatic lower extremity PAD had an approximately threefold higher relative risk for death within 10 years than did our 331 controls matched for age, sex and diabetes mellitus status. The aim of our study, however, is to evaluate the effect of diabetes mellitus on long-term mortality. As a result, the relative risk for death within 10 years was approximately twofold and approximately fourfold in PAD patients without and with diabetes, respectively, as compared with healthy controls. We thus conclude that the mortality probability of a certain patient at 10 years strongly depends on whether the PAD patient has diabetes mellitus or not.
Published data on 10-year mortality rates in patients with established/symptomatic PAD are rare.11–14 One article reporting on 10-year all-cause mortality in 67 patients with symptomatic PAD demonstrates that 48% had died at 10 years. 11 The second study investigated the long-term outcome in 109 PAD patients and reported that 42% of them had died at 10 years. 12 Another study on the 10-year all-cause mortality of 40 PAD patients revealed a mortality rate of 38% during follow-up. 13 A fourth study evaluating long-term all-cause mortality demonstrated that 41% of 2642 patients with PAD died within 10 years of enrolment. 14 By comparison, 39% of the 331 patients with symptomatic PAD in our study died within 10 years.
Although not explicitly described for all five cohorts, there are most probably differences in the age distribution and the proportion of patients with critical limb ischemia, both factors known to be associated with poor outcome in PAD. In addition, when described, the proportion of patients with diabetes or hypertension and coexistent coronary artery or cerebrovascular disease differs among the studies. Our study included only Caucasian patients, while the other studies did not mention the distribution of race, if any. Lastly, the studies differed in setting. Nevertheless, mortality rates in the four cited studies and ours were fairly similar.
However, none of the former studies investigating 10-year all-cause mortality evaluated the PAD patients stratified according to diabetes mellitus status. Therefore, our finding that diabetes seems to be a main trigger for increased mortality rates at 10 years in patients with lower extremity PAD are novel and might have implications for a differentiated and optimal treatment strategy in non-diabetic versus diabetic PAD patients. To elucidate these important issues we intend to evaluate in our future work whether predictors of death differ in non-diabetic and diabetic PAD patients.
Limitations
We acknowledge that the LIPAD study was a single-centre study performed in Austria. In addition, we would like to emphasize that our patients were a selected subgroup of the overall PAD population, as detailed in the Methods section (Caucasian patients <75 years of age admitted for inpatient diagnosis/treatment of atherosclerotic PAD). Therefore, we are not able to generalize our findings to non-white individuals, patients with asymptomatic PAD or non-hospitalized PAD patients. Accordingly, the results of our single-centre study are probably not generally applicable and thus remain to be confirmed by future studies in other settings.
Furthermore, we had a great male predominance in our study, which, however, reflects the epidemiological situation of PAD in Austria at the time of patient recruitment (i.e. April 2000 to April 2002). In the year 2002, for example, 13,553 patients <75 years of age with the main diagnosis of lower extremity PAD (ICD10 codes I70.2 and I73.9) were discharged from hospital in Austria according to Statistics Austria (www.statistik.at). Of these hospital discharges, 9087 (67%) were male and 4466 (33%) were female.
Next, we found that diabetes mellitus per se is a risk factor for poor outcome in PAD, but of course diabetic control most probably matters. It is therefore another limitation of our study that we are not able to differentiate between well and poorly controlled disease in time course during our 10-year follow-up period in PAD patients and controls. However, knowing the Austrian health care system, we assume that the proportion of well and poorly controlled disease was definitely not lower in PAD patients than in controls.
A last limitation also deserves clarification. Our controls cannot be considered individuals without any atheroscle-rosis. Our controls had the following characteristics: no coronary artery or cerebrovascular disease, as defined in the Methods section; no previous stenting or vascular surgery of the internal carotid arteries; no stenosis of the internal carotid arteries >50% as assessed by colour duplex ultrasound scanning; no history or current clinical evidence of PAD; no pathological patterns of pulse waves in the legs shown by continuous-wave spectral analysis; ABI ⩾1.0. Thus, although we had stringent selection criteria for our controls and excluded ‘significant’ atherosclerotic disease by history and by screening, we cannot exclude the presence of atherosclerotic disease per se in our controls. Given the age distribution of our controls with a median age of 65 years ranging up to 75 years, it is conceivable that even a great proportion of the controls had atherosclerosis. However, this actuality had rather contributed to an underestimation of the risk for death in PAD patients versus controls in the diabetic and non-diabetic subgroups.
Conclusion
In this study, mortality rates at 10 years differed in PAD patients with and without diabetes. Our findings suggest that distinct risk assessment strategies should be applied in the two PAD subgroups in future studies.
Footnotes
Acknowledgements
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.