
Abstract
Stanford type B aortic dissection (TBAD) is a life-threatening aortic disease. The initial management goal is to prevent aortic rupture, propagation of the dissection, and symptoms by reducing the heart rate and blood pressure. Uncomplicated TBAD patients require prompt medical management to prevent aortic dilatation or rupture during subsequent follow-up. Complicated TBAD patients require immediate invasive management to prevent death or injury caused by rupture or malperfusion. Recent developments in diagnosis and management have reduced mortality related to TBAD considerably. In particular, the introduction of thoracic stent-grafts has shifted the management from surgical to endovascular repair, contributing to a fourfold increase in early survival in complicated TBAD. Furthermore, endovascular repair is now considered in some uncomplicated TBAD patients in addition to optimal medical therapy. For more challenging aortic dissection patients with involvement of the aortic arch, hybrid approaches, combining open and endovascular repair, have had promising results. Regardless of the chosen management strategy, strict antihypertensive control should be administered to all TBAD patients in addition to close imaging surveillance. Future developments in stent-graft design, medical therapy, surgical and hybrid techniques, imaging, and genetic screening may improve the outcomes of TBAD patients even further. We present a comprehensive review of the recommended management strategy based on current evidence in the literature.
Introduction
Stanford type B aortic dissection (TBAD) is a life-threatening vascular disease, with a 5-year mortality of about 30–40%.1–3 It is caused by a tear in the intimal layer of the descending thoracic aorta, which allows blood flow between the intima and media, resulting in a separation of these layers. As a result, a true and a false lumen develop, which disrupts normal blood flow and may cause malperfusion to vital organs or even aortic rupture.4–11
The incidence of TBAD is approximately 3 per 100,000 persons per year. Although its pathogenesis remains complex, it appears to be caused by conditions that evoke decreased vascular wall strength and increased hemodynamic forces on the aortic wall. 12 Large clinical studies have reported that systemic hypertension is present in about 80% of patients with acute TBAD, 13 making it one of the most important risk factors, together with increasing age and atherosclerosis.11,14 In addition, factors such as congenital bicuspid or unicommissural aortic valves, 15 history of cocaine abuse, 16 pregnancy, 4 strenuous activities and severe emotional stress 17 are also associated with development of aortic dissection. Connective tissue disorders are likewise associated with TBAD.8,13,18
The Stanford classification is the most widely adopted for aortic dissection, and defines TBAD as involvement of the descending thoracic aorta with absence of ascending aortic involvement. 19 Patients suffering from TBAD usually present with a sudden onset of tearing or ripping chest pain.8,13,18 Clinically, subdivision is made into complicated and uncomplicated TBAD, as the prognosis differs significantly. Complicated TBAD is defined by the presence of at least one of the following symptoms or signs: aortic rupture, hypotension/shock, malperfusion, neurological signs, acute renal failure, recurrent or refractory pain, refractory hypertension, and/or early aortic dilatation or propagation of dissection.8,13,20,21 Uncomplicated TBAD refers to stable patients lacking these symptoms and signs at presentation and during the hospital course.13,18,22 The in-hospital survival for complicated TBAD patients is approximately 50%, while about 90% of uncomplicated TBAD patients survive until discharge.4,5,13,18,23–25 Based on time frame, the International Registry of Aortic Dissection (IRAD) investigators subclassify aortic dissection patients as hyperacute (symptom onset up to 24 hours), acute (2–7 days), subacute (8–30 days), and chronic (>30 days; Figure 1). 26 Acute TBAD is much more aggressive than chronic expanding TBAD, and after endovascular repair has a reported 30-day mortality of 19% compared to 0%, respectively, with significantly higher complication rates. 27
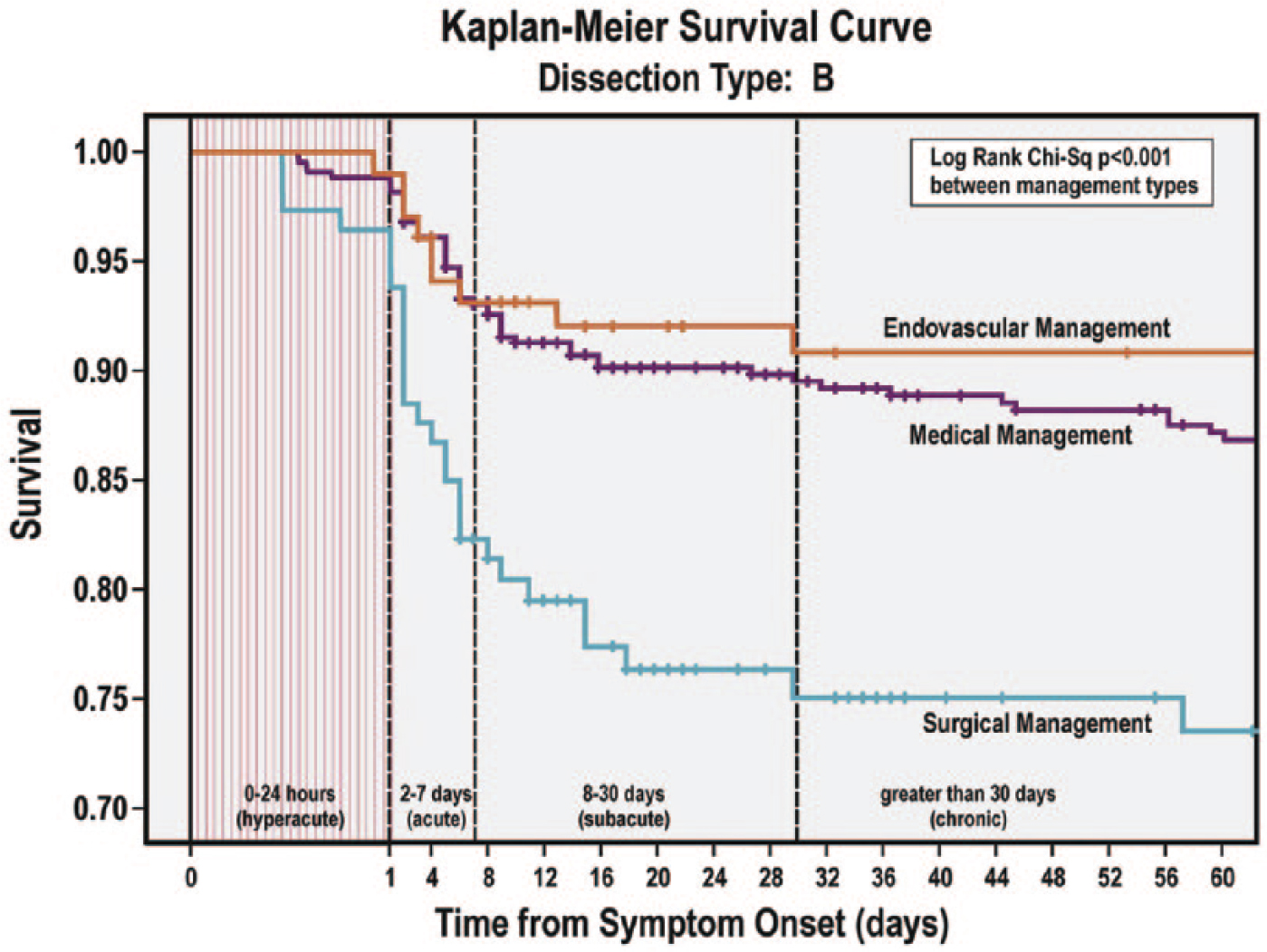
Kaplan-Meier survival curve for type B dissection stratified by treatment type. Note the continued decreasing survival up to 30 days after presentation in what has been traditionally considered the ‘chronic’ phase of aortic dissection. 26
Although TBAD can be suspected clinically, it is confirmed with imaging. Some patients present with few or no obvious symptoms or signs, which may cause an important delay in diagnosis. 26 Therefore, physicians should be familiar with atypical presentation of TBAD and should have a low threshold for performing diagnostic imaging. The most widely adopted and applied imaging modality for TBAD is computed tomography (CT). The diagnosis is confirmed if a false aortic lumen is observed. In this review, we present a comprehensive approach to the recommended management strategy based on current evidence.
Management of TBAD
Goals of TBAD management consist of restoring perfusion to the vital organs and preventing dissection progression or aortic rupture. To prevent complications, it is vital to make a risk assessment at an early stage to determine the merits of medical, endovascular or surgical intervention. Currently, imaging plays an important role in making such an assessment for TBAD patients.
Imaging
Imaging of the total aorta is recommended when TBAD is suspected. CT angiography (CTA), magnetic resonance imaging (MRI), and trans-esophageal echocardiography are all reliable imaging modalities to confirm or exclude the diagnosis of TBAD. 28 Transthoracic echocardiography may also be useful in hemodynamically unstable patients because it is portable and widely available. However, it is associated with low sensitivity (31–55%) in confirming TBAD and is limited in visualizing the descending thoracic aorta. 29 It may still be used effectively for rapid assessment of any retrograde involvement of the ascending aorta or arch, as well as for the presence of pericardial tamponade. 30 Trans-esophageal echocardiography offers a much more accurate examination for TBAD (sensitivity of about 80%) with better assessment of entry tears, true lumen compression, and potential retrograde involvement of the ascending aorta or the arch. 31 In addition, color Doppler can help to detect small communications and dissection flap movement. Therefore, this modality may be useful to identify variants of acute aortic syndromes, such as intramural hematoma and penetrating aortic ulcers. Although echocardiography remains useful to rapidly evaluate the proximal thoracic aorta, CTA and MRI are considered superior to evaluate the extent of the dissection and potential branch involvement.32,33
CTA is the most commonly used modality to assess aortic dissection since it is widely available, accurate, and fast. With CTA, important prognostic factors for patients with TBAD can be characterized. Specifically, partial false lumen thrombosis independently predicts aortic growth and follow-up mortality in acute TBAD.34,35 Other independent predictors of mortality include periaortic hematoma and descending aortic diameter ⩾5.5 cm. 36 Moreover, size of the primary tear (>10 mm), one entry tear, entry tear in the inner curvature, false lumen diameter >22 mm, and elliptic true lumen combined with saccular false lumen are related to increased risk of aortic growth and complicated TBAD.37–40 Finally, branch vessel involvement and a totally patent false lumen are associated with decreased complete thrombosis of the false lumen. 36 These morphologic signs can predict complications and may therefore guide the choice of management strategy (Figure 2).
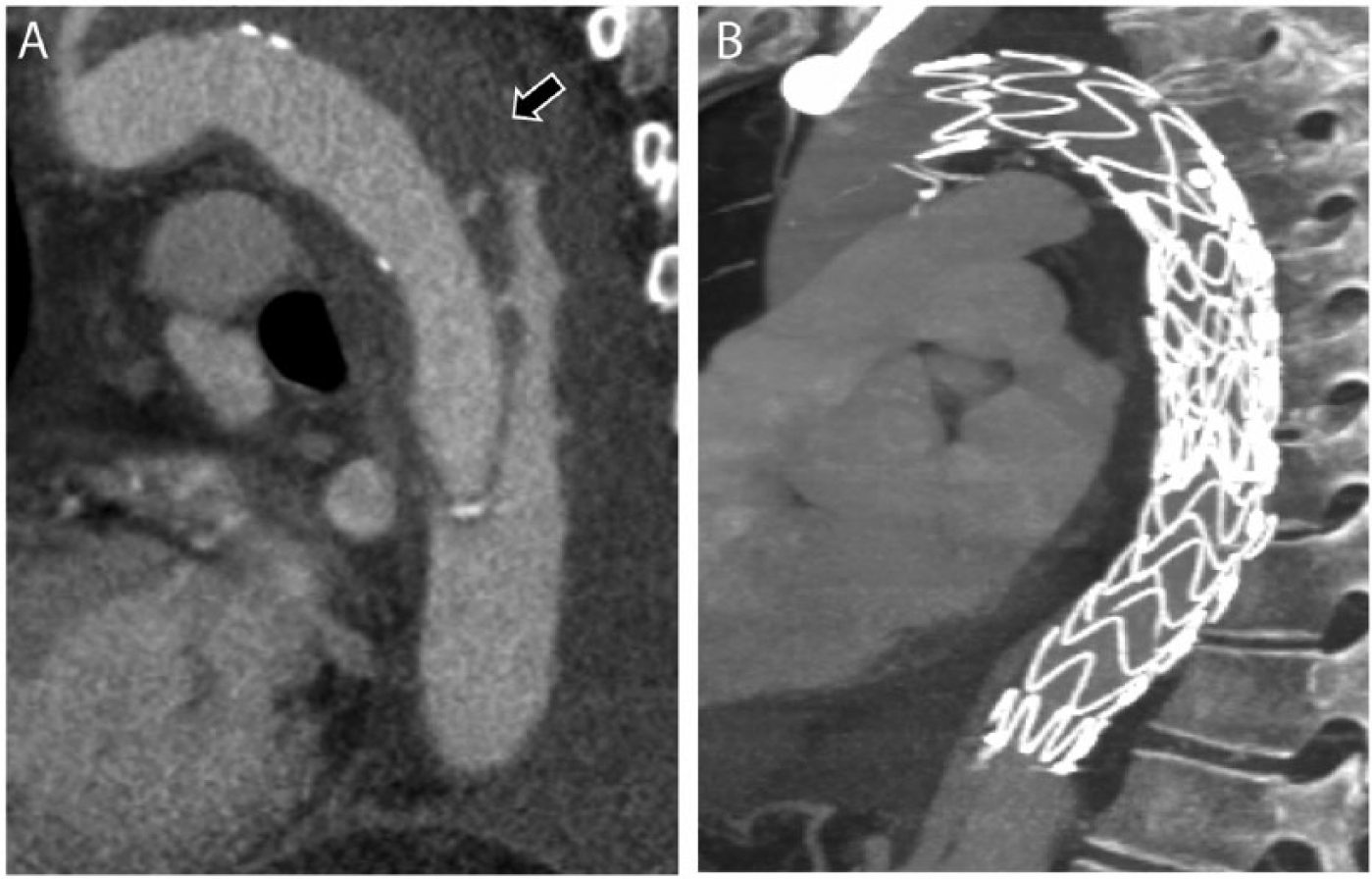
Sagittal view on CTA imaging of a complicated type B aortic dissection (TBAD). (A) Periaortic hematoma (arrow) suggesting aortic rupture. (B) The result of successful management with thoracic endovascular aortic repair (TEVAR).
The use of ECG-gated CTA imaging is currently recommended to overcome pulsation artifacts. 21 However, recent non-ECG gated CTA developments, such as fast gantry rotation, may also overcome motion artifacts with reduced exposure to radiation and contrast agent. 41 Future studies will have to confirm the accuracy and feasibility of such new CTA imaging techniques.
MRI offers a comprehensive examination of aortic dissections including both anatomical and functional information. Contrast-enhanced MRI (typically using intravenous gadolinium) can visualize the thoracic aorta and arch vessels as a three-dimensional MR angiogram. Delayed phase acquisitions with use of blood pool agents may improve visualization of the false lumen status, which may be overestimated with first pass CTA imaging. 42 Moreover, time-resolved MR angiography provides an assessment of flow dynamics. This can reveal new potential dynamic predictors of complications in TBAD patients, such as vessel malperfusion, helical blood flow in the false lumen, velocity, and false lumen stroke volume. 43
Optimal medical treatment (OMT)
All TBAD patients should be initially managed with medical therapy to reduce hemodynamic forces and mitigate the risk for immediate rupture or dissection extension. Thereafter, medical treatment strategies may be subdivided into acute or chronic treatment. An overview of medical therapy recommendations for TBAD patients is given in Table 1.
Medical therapy for type B aortic dissection (TBAD).
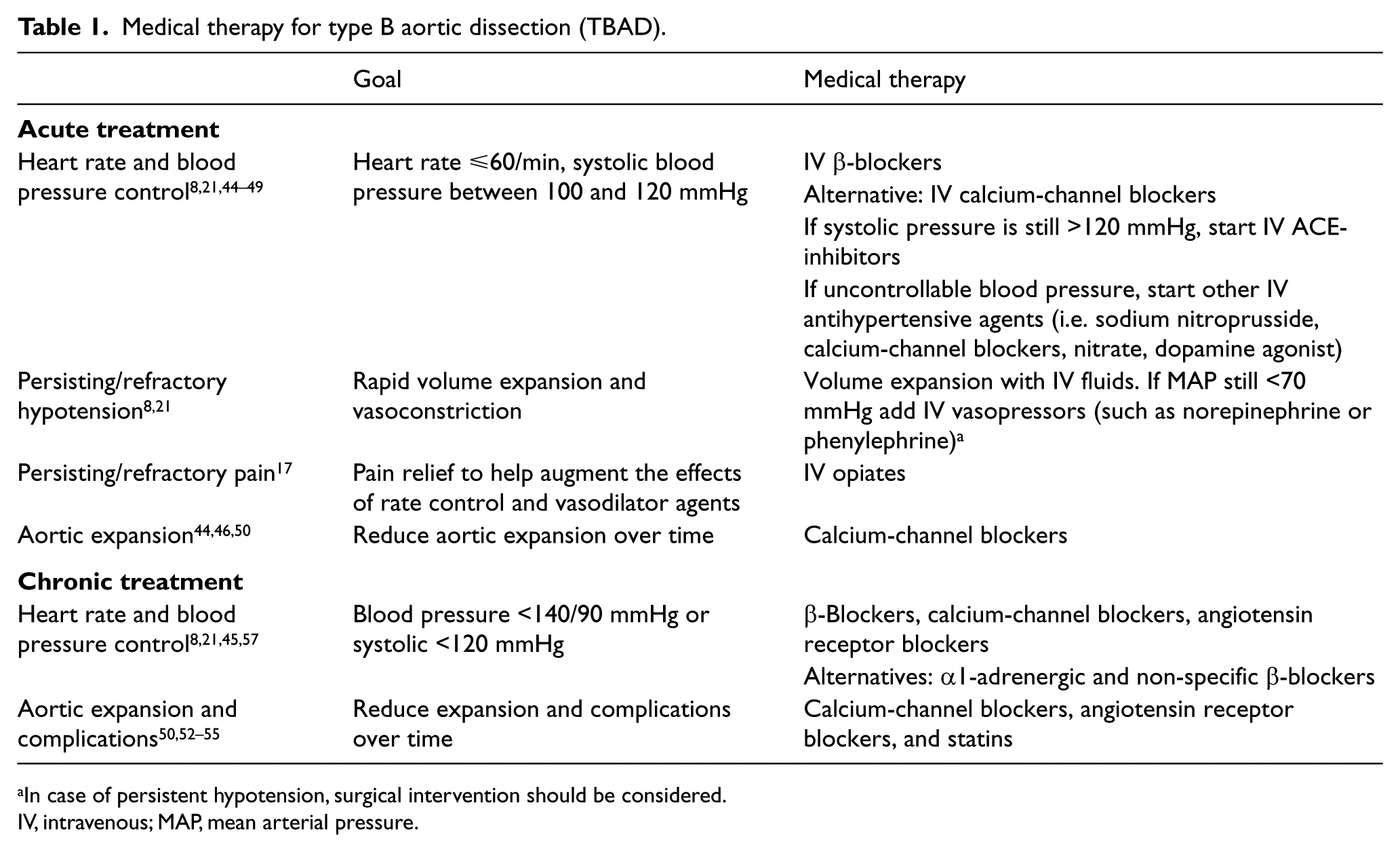
In case of persistent hypotension, surgical intervention should be considered.
IV, intravenous; MAP, mean arterial pressure.
Acute medical treatment
In acute TBAD, the main goal of medical therapy is to limit the risk of rupture or dissection propagation by control of blood pressure and heart rate. Medical therapy should include intravenous β-blockers,8,21,44,45 and in patients not responding to β-blockers or with poor tolerance of the drug, calcium-channel blockers and/or renin-angiotensin inhibitors can be used as alternatives. If the blood pressure remains uncontrollable, other intravenous hypertensive agents should be administered (i.e. sodium nitroprusside, calcium-channel blockers, nitrate, dopamine agonist).8,21,44–49 Large trials have revealed that β-blockers and calcium-channel blockers are associated with improved long-term survival in acute TBAD patients. 46 In addition, it has been reported that calcium-channel blockers are associated with reduced aortic expansion and improved survival in acute TBAD patients.44,50 Patients that present with refractory hypotension should be managed immediately with rapid volume expansion in combination with vasopressors such as norepinephrine or phenylephrine to preserve organ perfusion as a bridge to aortic repair.8,21 Pain should be relieved with intravenous opiates since emotional stress may increase blood pressure considerably, potentially further propagating the dissection. 17 Persistent or refractory pain may indicate dissection progression or impending rupture and is associated with increased mortality, and should therefore be considered a complication, possibly requiring intervention. 7 Other clinical signs associated with increased mortality in acute TBAD patients are acute renal failure, hypotension/shock, mesenteric ischemia, and limb ischemia, and therefore acute aortic repair should be considered to restore adequate blood perfusion. 36
Chronic medical treatment
For patients with uncomplicated TBAD, optimal medical treatment (OMT) is widely accepted as the standard initial management,8,21,25,51 together with consideration of endovascular repair. The goal of OMT for chronic TBAD is to delay the rate of aortic expansion. Tight heart rate and blood pressure control, calcium-channel blockers, angiotensin receptor blockers, and statins have been associated with reduced aortic growth and complications.44,50,52–55 However, large clinical trials are still warranted to evaluate the long-term efficacy of these medical treatments for TBAD. For TBAD patients with Marfan syndrome, β-blockers remain the first line therapy, but angiotensin receptor blockers specifically appear to reduce aortic growth in this cohort.47–49,56 Alternative medical therapies include α1-adrenergic and non-specific β-blockers. 57 Prior to hospital discharge, all intravenous medication should be converted to oral agents and long-term blood pressure regulation with adequate surveillance being of vital importance.
Endovascular procedures
TEVAR (Thoracic EndoVascular Aortic Repair) development and techniques
Open surgical repair of aortic dissection started in the 1950s and was associated with high morbidity (paraplegia rate of 30–36%) and mortality (29–50%).58–60 These unsatisfactory complication rates motivated the need for a minimally invasive approach, which lead to the development of TEVAR in the 1990s. 61 Soon after the introduction of TEVAR, TBAD-related morbidity and mortality decreased dramatically.61–70 The aim of TEVAR for aortic dissection is to discontinue blood flow into the false lumen by covering the primary entry tear, and to restore blood flow into the true lumen. The false lumen subsequently depressurizes, preventing extension of dissection and ideally leading to false lumen thrombosis with subsequent aortic remodeling.71,72 Potential clinical benefits of TEVAR for TBAD include hemodynamic stabilization, reversal of end-organ ischemia, reduced morbidity and mortality, minimal procedural morbidity, interventional treatment of surgically unfit patients, short procedure time with minimal blood loss, decreased recovery time and potential cost savings. Adequate preoperative sizing of the stent-graft is a key aspect to achieve adequate fixation, without damaging the aortic wall. Device ‘oversizing’ in TBAD patients remains a topic of debate as it is associated with severe complications such as stent-graft-induced new entry tears, retrograde type A dissection, and proximal neck dilatation with subsequent stent-graft migration.73–76 In general, oversizing by no more than 0–10% is recommended for patients with TBAD.74,77
Mis-sizing of the stent-graft can be avoided by keeping in mind the dynamic behavior of the aorta.78–80 Adequate device size should be based on the diameter of the aorta proximal to the dissected segment. Furthermore, a proximal aortic neck length of at least 2 cm is needed to achieve adequate fixation of the stent-graft.81,82 The first technical challenge for TEVAR procedures is cannulating the stent-graft into the usually narrowed true lumen. Trans-oesophageal echography may offer valuable assistance for this task.83,84 In addition, intravascular ultrasound and phased array intra-cardiac ultrasound have been reported as useful imaging tools for this procedure.85–87 Accurate deployment of the stent-graft requires endovascular experience 88 and may be assisted by blood pressure and pulse regulation.88,89 When introduction challenges are encountered, an antegrade approach via the brachial artery might offer a solution to snare a guidewire in the aorta. 90 Iliac artery endoconduits have also emerged as safe alternative access routes. 91 For deployment of the stent-graft, a tip-capture system allows selective release of the proximal spring which permits repositioning before fully releasing the endograft. Such a system is particularly useful for deploying a stent-graft in a curved vessel like the thoracic aorta.92–94 After deployment, ballooning is not recommended due to the risk of devastating complications such as retrograde type A aortic dissection and aortic rupture.95–97 Based on the self-expanding character of the stent and the time required for aortic remodeling, a conservative approach is advised after deployment, even if the stent-graft has not fully expanded. Technical success rates of TEVAR are high for both acute TBAD (ranging from 93.3% to 100%)98–100 as well as for chronic TBAD (ranging from 77.6% to 100%).94,101,102 Chronic TBAD is associated with a thickened and stiffened dissection flap, which might explain the lower success rate of TEVAR in this cohort. Proximal fixation of the stent-graft in the aortic arch is important, as mechanical forces, blood flow and aortic pulsatility might jeopardize durable fixation of the stent-graft. Intentional over-stenting of the left subclavian artery can increase applicability of endovascular repair; however, this should be performed with caution to avoid ischemic events due to complete occlusion of the left subclavian artery. Therefore, arterial revascularization is advised, for which several techniques have been described. Preoperatively, left subclavian artery revascularization for TEVAR in TBAD is typically accomplished by a surgical bypass from the left common carotid to the left subclavian artery. 103 However, depending on the occlusion of cervical branches, more complex revascularization surgery may be necessary, such as a bypass from the brachiocephalic artery or the ascending aorta. 104 Perioperatively, in situ laser fenestration of the stent-graft has also been associated with good outcomes. 105 An overview of the evidence for the use of TEVAR in complicated and uncomplicated TBAD is given in Table 2.
TEVAR for type B aortic dissection (TBAD).
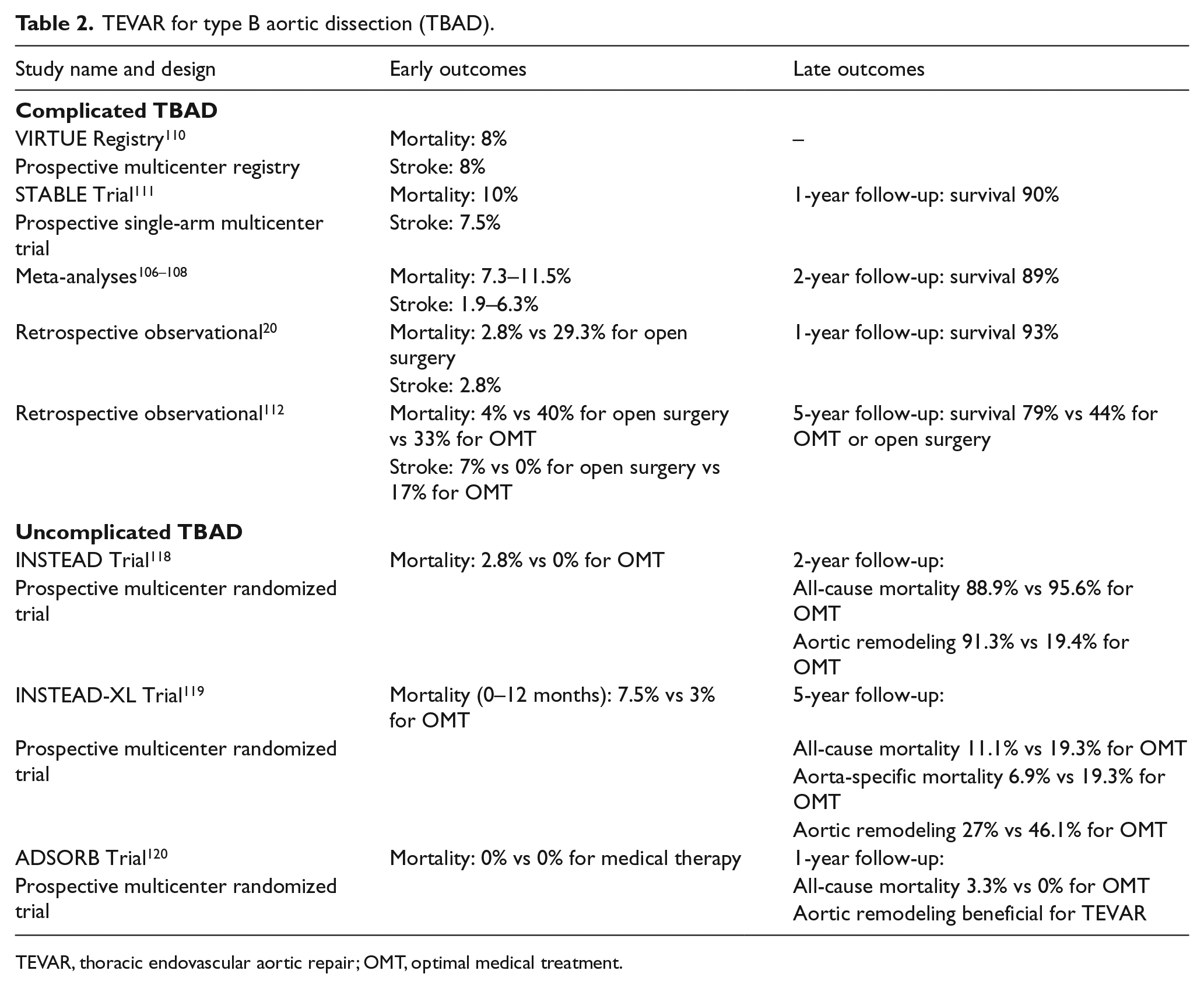
TEVAR, thoracic endovascular aortic repair; OMT, optimal medical treatment.
Complicated TBAD
TEVAR for complicated TBAD has proved to be superior to OMT alone in the mid-term. 70 Szeto et al. reported a decrease in 30-day mortality for open repair versus TEVAR as well, from 29.3% to 2.8% in open surgery versus endovascular repair, respectively. 20 Currently, there are three meta-analyses published which report the short and mid-term result in complicated TBAD patients treated with TEVAR.106–108 In-hospital mortality ranged from 7.3% to 11.5% and stroke from 1.9% to 6.3%. TEVAR is now considered the gold standard for complicated TBAD.8,21,51,109 A prospective multicenter European clinical registry showed a 30-day mortality of 8%, with 8% risk of stroke and 2% risk of spinal cord ischemia in 50 acute TBAD patients. 110 In addition, the initial results of a single-arm multicenter study for endovascular treatment of complicated TBAD using a composite device design (PETTICOAT technique), which includes an uncovered infra-diaphragmatic aortic stent in addition to standard TEVAR, showed a 1-year mortality of 10%. 111 Stroke, transient ischemic attack and progression of dissection were seen in 7.5%, 2.5% and 5% of patients, respectively. Another observational study confirmed the beneficial outcomes of TEVAR for acute complicated TBAD, with an in-hospital mortality of 4%, 40% and 33% for TEVAR, open surgery and medically treated patients, respectively. 112 In complicated TBAD, those presenting with visceral malperfusion represent a cohort with poorer outcomes. In these patients, although visceral patency after TEVAR is excellent (up to 97%), 30-day mortality remains high (ranging between 31% and 62%), as well as aortic related complications during follow-up.113–115
Uncomplicated TBAD
Management of uncomplicated TBAD is usually OMT; however, there is on-going debate about the possible beneficial role of TEVAR for these patients. TEVAR has shown promising results in this cohort,116,117 and, recently, two trials have been conducted to assess the benefit of elective TEVAR in these patients. The INSTEAD trial, which included TBAD patients in the subacute and chronic phase, found that there was no survival benefit of TEVAR compared to OMT alone after a 2-year follow-up. 118 TEVAR did show favorable results between 2 and 5 years of follow-up, since both all-cause and aorta-specific mortality were improved with TEVAR in the long-term. 119 Moreover, the TEVAR group showed less progression of dissection, suggesting remodeling of the aorta after 5 years, compared to the medically managed group (27.0% vs 46.1%; p=0.04). TEVAR was also associated with stent-graft-induced false lumen thrombosis in 90.6%, while the rate of false lumen thrombosis in patients treated with OMT alone was 22.0% (p<0.001). 119 However, it was also reported that the initial mortality was higher in the TEVAR group compared to the OMT group and that many of these patients required re-interventions during follow-up. 119 Furthermore, the long-term benefits of TEVAR may not be achievable in older patients. Lastly, it must be noted that this study was industry sponsored and underpowered and should be interpreted accordingly.
The ADSORB trial is the only randomized trial which compared OMT plus TEVAR with OMT alone for acute uncomplicated TBAD. 120 This trial was underpowered for survival, and had a cut-off at 1-year follow-up. Even though the follow-up was short, a benefit for TEVAR in terms of aortic remodeling was found. Incomplete false lumen thrombosis was seen in 43% of patients managed with TEVAR plus OMT, versus 97% in the OMT cohort (p<0.001). Moreover, patients managed with TEVAR and OMT showed true lumen expansion and false lumen reduction, whereas patients treated solely with OMT showed an unchanged true lumen size with expansion of the false lumen. 120 As mentioned, the study was underpowered for survival, and also was industry sponsored, and therefore the same interpretation reservations should be considered as with the INSTEAD trial.
These limited but promising results of elective TEVAR for uncomplicated TBAD have led to a global discussion of whether all TBAD patients should be considered for TEVAR. Owing to the lack of definitive evidence, a patient-specific approach is currently advised for TEVAR in TBAD, reserving TEVAR for complicated patients or those suspected of complications (including aortic dilatation) during follow-up.21,121 A number of patients with uncomplicated TBAD might never suffer from disease progression and complications. Therefore, several studies have searched for predictors of adverse outcomes in uncomplicated TBAD patients. During the chronic course, complications are characterized by aneurysmal dilation >55 mm, an aortic yearly increase of >4 mm or a recurrence of symptoms despite best medical therapy (Figure 3). 1 The following signs have been associated with poor outcome and more rapid disease progression than baseline: patency of the presence of flow but absence of thrombus (FL) during follow-up, increased number of entry tears, initial aortic diameter ⩾4 cm with a patent FL, initial FL diameter ⩾22 mm in the proximal descending aorta, visceral vessel involvement and recurrent or refractory pain or hypertension.7,37,122–126
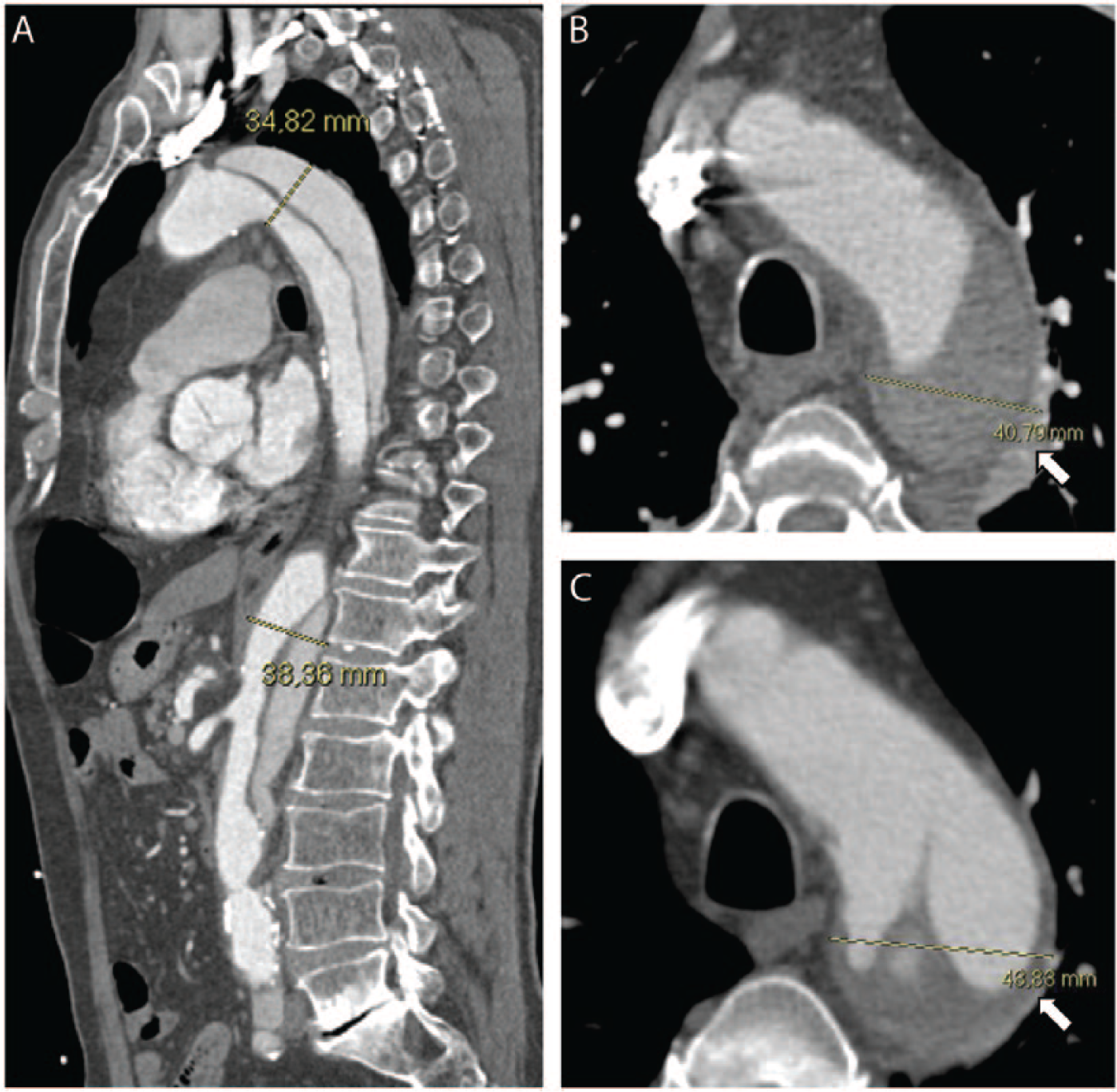
(A) Sagittal view on CTA imaging of an uncomplicated type B aortic dissection (TBAD) managed with medical therapy showing positive aortic remodeling at the 6-year follow-up. The descending thoracic aortic diameter is <4 cm. (B and C) Axial view of an uncomplicated TBAD showing (B) baseline aortic diameter (40.8 mm; white arrow) and (C) 3 mm growth at 1-month follow-up (43.8 mm; white arrow).
Connective tissue disorders
TEVAR has been reported to be feasible for Marfan patients (although this is controversial); 127 however, reintervention rates are high as Marfan-diseased aortas tend to dilate over time after TEVAR.128,129 These patients are at higher risk for TEVAR-related complications such as retrograde dissection and stent-graft-induced new entry tears.73,74,96,97,130 For TBAD patients with Ehlers-Danlos or Loeys-Dietz syndrome there are currently no data, besides a few case reports, to support any use of TEVAR, except in emergency situations to achieve hemodynamic stabilization as a bridge to definitive surgical therapy.21,131,132
Surgery
Open repair
Owing to advancements in endovascular techniques, open surgical repair for TBAD is currently reserved for patients in whom endovascular management is not feasible or has failed. The aim of open surgical repair is to replace the descending aorta with a graft, excising the intimal tear, restoring peripheral and visceral perfusion, and repairing or preventing aortic rupture. Currently, there are no randomized controlled trials available to compare the different open surgical techniques and therefore the level of evidence regarding optimal treatment is low. Generally, the descending aorta is exposed through a left posterolateral thoracotomy. Subsequently, the proximal entry tear is resected and a surgical graft is implanted to replace the dissected aorta. Partial cardiopulmonary bypass can be established through the left atrium and femoral artery and has been widely used. In patients with retrograde arch involvement of the dissection, full cardiopulmonary bypass, using the femoral artery and vein, may be required. Hypothermic circulatory arrest has been adopted for cerebral protection in a subset of patients who are managed with open proximal graft anastomosis,133–135 and may be accompanied by selective antegrade perfusion. Surgical aortic fenestration or extra-anatomical bypass has been used for treating ischemic complicated acute TBAD, but with the introduction of minimal invasive techniques this procedure is only used as an alternative treatment in case of contraindications or failure of endovascular management. 136 In patients presenting with complications such as imminent rupture, aortic expansion, or malperfusion syndromes, classic open surgery carries a significant risk of morbidity, including irreversible spinal injury and postoperative death.133–135
Although the results of open surgical repair of the descending aorta have improved over the last decades,137–140 they remain unsatisfying, with in-hospital mortality for TBAD patients of about 25–50%.24,109,141 The preoperative condition of the patient highly influences the outcome of surgical repair. Patients older than 70 years with hypotension/shock have less favorable outcomes, while those with a normal blood pressure at the time of surgery have better outcomes. 24 Preoperative severe visceral malperfusion and spinal cord ischemia are correlated with poor prognosis after open surgery, and therefore may be spared such invasive therapy. In addition, extensive co-morbidity, such as end stage malignant disease and severe chronic obstructive pulmonary disease are considered contraindications for surgical aortic repair.
Postoperative complications affect between 40% and 80% of surgically managed TBAD patients. 140 These mainly include respiratory failure (29%), shock (21%), acute renal failure (19%), sepsis (18%), stroke (9%), left vocal cord paralysis (9%), spinal cord ischemia (7%), visceral ischemia (5%), cardiac ischemia/infarction (3%), and limb ischemia (4%).24,51,109,137–141 Complications predominantly associated with the extent and duration of the operation are paraplegia, temporary paraparesis and stroke.24,51,140,141 To reduce neurological and renal complications, the use of extracorporeal circulation has been suggested; however, its benefits remain undetermined.51,137,140
Connective tissue disorders
Patients with connective tissue disorders (i.e. Marfan, Ehlers-Danlos, and Loeys-Dietz syndromes) and TBAD are at considerably higher risk of aortic dilatation and rupture.128,142 The gold standard for patients with Marfan or Loeys-Dietz syndromes complicated by TBAD remains open surgery, which offers the best beneficial long-term results for these patients.8,21,143 The surgical approach includes aortic repair through left thoracotomy or medium sternotomy using a frozen elephant trunk technique. 144 The role of surgical aortic repair in patients with Ehlers-Danlos syndrome is not clearly defined yet, since surgery may have devastating outcomes due to the fragility of the aortic tissue. 145 Nevertheless, when these patients present with aortic dissection, successful aortic surgery can be achieved with careful tissue handling and the use of pledgeted sutures. 144
Hybrid approach
For patients who present with both arch and distal aortic pathology, the risks of complete open surgery are high. Therefore, surgical aortic arch replacement with antegrade stenting of the descending thoracic aorta was introduced in the mid-1990s as the ‘frozen elephant trunk’ technique.146,147 This hybrid technique is currently associated with acceptable in-hospital mortality (ranging from 0% to 27.7%) and 5-year survival (ranging from 68% to 96%) for acute aortic dissection with arch involvement.148–151 Notably, these are pooled data from a review of small studies with limited follow-up data. Positive aortic remodeling, defined as postoperative partial or complete FL thromboses in the descending aorta, is reported in about 90% of the cases. 150 Finally, hybrid aortic repair has also been associated with promising outcomes for patients with connective tissue disorders (including Marfan, Ehlers-Danlos, and Loeys-Dietz syndromes). 151 However, these surgical interventions should be carried out in stages to reduce the risk of perioperative complications. Moreover, these patients require lifelong imaging surveillance due to the increased risk of aortic complications during follow-up. Their management should probably be referred to centers having the most experience with these procedures.
Genetics
Besides hypertension and atherosclerosis, familial aortic syndromes and connective tissue disorders are important etiologies of TBAD. It is therefore recommended that the aortas of first-degree relatives of patients with thoracic aortic dissection undergo imaging to identify potential asymptomatic aortic patients.8,152,153 Sequencing of genes known to cause familial thoracic aortic dissection may also be considered in patients with a family history of aortic dissection to determine if gene mutations are responsible for the aortic pathology. 8 Candidate genes associated with aortopathy are being increasingly identified, and commercially available tests currently include COL3A1, TGFBR1, TGFBR2, TGFB2, SMAD3, ACATA2, and FBN1. Several studies aim to identify more gene mutations related to aortic dissection.154,155 Such genetic testing should only be done in collaboration with medical geneticists with appropriate patient counseling. Routine genetic testing has been shown to be valuable in revealing important information regarding familial aortic pathologies, which should be discussed in detail during patient counseling. 154 Such data can provide genetically personalized care since it has increasing implications for the choice of management. 154 Therefore, if one or more first-degree relatives of a patient with aortic dissection are found to have aortic dilatation or dissection, referral to a geneticist may be considered.
Summary
In summary, TBAD continues to be a challenging clinical problem, and remains a life-threatening disorder, in spite of significant advances. Prompt diagnosis, aggressive medical therapy, urgent intervention for complicated cases, and emerging endovascular interventional options have all contributed to a significant decline in the morbidity and mortality associated with this disease. Challenges remain, however. There is still significant controversy about optimal procedural intervention, especially in uncomplicated TBAD. At present, endovascular intervention for complicated TBAD has become the standard, modified with adjunct procedures or hybrid intervention when necessary. Aggressive medical therapy, focusing on blood pressure control, is essential for all TBAD patients. Future study and procedural innovations should continue to improve outcomes, and address the role of interventional therapy for uncomplicated TBAD patients, as well as the effectiveness of genetic testing for TBAD patients and their families.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: UM Faculty Group Practice, Ann and Bob Aikens, Varbedian Aortic Research Fund, Terumo BCT, Mardigian Foundation, WL Gore & Associates, Inc., William and Flora Hewlett Foundation, and Medtronic.