
Abstract
We sought to investigate the possible association between the area of the epiaortic fat pad (EAFP) and dimensions of the ascending aorta. A total of 193 individuals underwent transthoracic echocardiography (TTE) prospectively. The area of the EAFP was traced anterior to the aortic root and correlated with the diameter of the aorta. The mean area of the EAFP was 5.16 ± 2.28 cm2. Absolute and indexed dimensions of the ascending aorta had a significant correlation with the area of the EAFP (p <0.001 for all). In a multivariate linear regression model, age >65 (p <0.001), body mass index >30 kg/m2 (p = 0.02) and a history of hyperlipidemia (p = 0.003) were identified as independent predictors of the area for EAFP. In conclusion, both the absolute and indexed diameters of the ascending aorta at the different segments that directly come into contact with the EAFP linearly correlate with the area of the EAFP measured by TTE.
Introduction
Perivascular adipose tissue increasingly gains attention as a paracrine modulator of vascular remodeling and has been implicated in the pathogenesis of various vasculopathies. 1 Perivascular fat is reported to contribute to the progression of atherosclerosis and associated vascular dysfunction.2,3 Epicardial fat is a visceral fat deposit, located between the myocardium and visceral pericardium. It is known to contribute to local inflammation and is implicated in coronary atherosclerosis. 4 The extent of periaortic and epicardial fat has been reported to correlate with absolute dimensions in both thoracic and abdominal aorta.5,6
The development of a reliable imaging method by non-contrast enhanced multi-detector computed tomography (CT) has enabled us to quantify the volume of periaortic fat tissue by using a relatively less invasive technology. 7 Using this technology, a recent study has described a direct correlation between the volume of periaortic fat and the dimensions of both thoracic and abdominal aorta. 3 However, this method is cost inhibitive and is not applicable in routine practice. Another study has shown a greater thickness of epicardial adipose tissue, measured by transthoracic echocardiography (TTE), in patients with a relatively larger diameter of the ascending aorta (>37 mm). 5 However, this measurement is limited since it only measures one dimension and therefore differentiating the pericardium from the epicardium anterior to the right ventricle could be challenging in certain patients. Nonetheless, the echocardiographic measurement of the area for epiaortic fat pad (EAFP), which is adipose tissue confined anteriorly to the aortic root, the right ventricular wall and the visceral pericardium, could easily be achieved in clinical practice. This measurement was the base of the estimate for the extent of the periaortic adipose tissue in our study.
We investigated the association between the area of the EAFP with the dimensions of the aortic root, sinotubular junction and the diameter of the ascending aorta at 3 cm and 5 cm distal to the annulus. We hypothesized that there is a direct correlation between the dimensions of the EAFP and the diameters of the underlying ascending aorta measured at different levels. We evaluated the linear relationship between this area and dimensions of the ascending aorta. According to the latest guidelines of the American Society of Echocardiography (ASE) and the European Association of Echocardiography (EAE), we further examined our findings as indexed dimensions of the aorta in order to correct for body surface area (BSA).8,9
To our knowledge, the correlation with the indexed dimensions of the ascending aorta and the area of the EAFP has not been previously investigated. We aimed to examine the linear regression interactions between the area of the EAFP (independent factor) and the indexed dimensions of the ascending aorta (primary outcome variables). We hypothesized that correcting the dimensions to the BSA would negatively affect the observed correlation between the size of the area of the EAFP and the indexed diameters of the aorta that are in direct contact with this fat pad.
Methods
IRB/consent
This is a cross-sectional prospective study conducted in a teaching heart hospital affiliated with Tabriz University of Medical Sciences. The study protocol was reviewed and approved by the local institutional review board and ethics committee.
Study population
A total of 193 healthy volunteers were enrolled and a written informed consent was obtained from each participant.
Subjects were excluded if they had hypertension (defined as a history of taking antihypertensive medication(s) or blood pressure over 140/90 mmHg checked twice before enrollment). Additionally, patients were not enrolled if they had echocardiographic evidence of left ventricular hypertrophy, bicuspid aortic valve, and rheumatic heart valve disease; any degree of aortic stenosis; more than mild aortic regurgitation; Marfan syndrome, Ehlers-Danlos syndrome or any other connective tissue disease; congenital heart disease; and had undergone a previous cardiac operation. Demographic information as well as subjects’ weight and height, and traditional risk factors for coronary heart disease were documented. Patients were flagged as diabetic if they had a fasting blood glucose level >126 mg/dL or were currently on oral hypoglycemic medications and/or insulin. Hyperlipidemia was defined as a serum total cholesterol level ⩾220 mg/dL and/or triglyceride ⩾150 mg/dL.
Echocardiographic measurements
Each patient underwent a two-dimensional (2D) TTE evaluation performed by an experienced cardiologist. A second cardiologist checked the recorded measurements and if there was a disagreement the case was excluded. In a modified long-axis view focusing on the area anterior to the aortic root (AR) and right ventricular outflow tract, we measured the area encircled by the anterior wall of the AR, the free wall of the right ventricle and the visceral pericardium in end-systole (Figure 1A). The measurement was repeated in three cycles and the average value was called EAFP. A sample measurement is depicted in Figure 1B. The diameters of the ascending aorta were measured at the levels of AR, sinotubular junction (STJ), 3 cm distal to the aortic annulus (AA3) and 5 cm distal to the aortic annulus (AA5). All aortic measurements were performed in 2D modes in end-systole and from leading edge to leading edge at the perpendicular plane to the aortic long-axis. Reported aortic diameters were divided by the BSA of each patient and reported as indexed sizes.
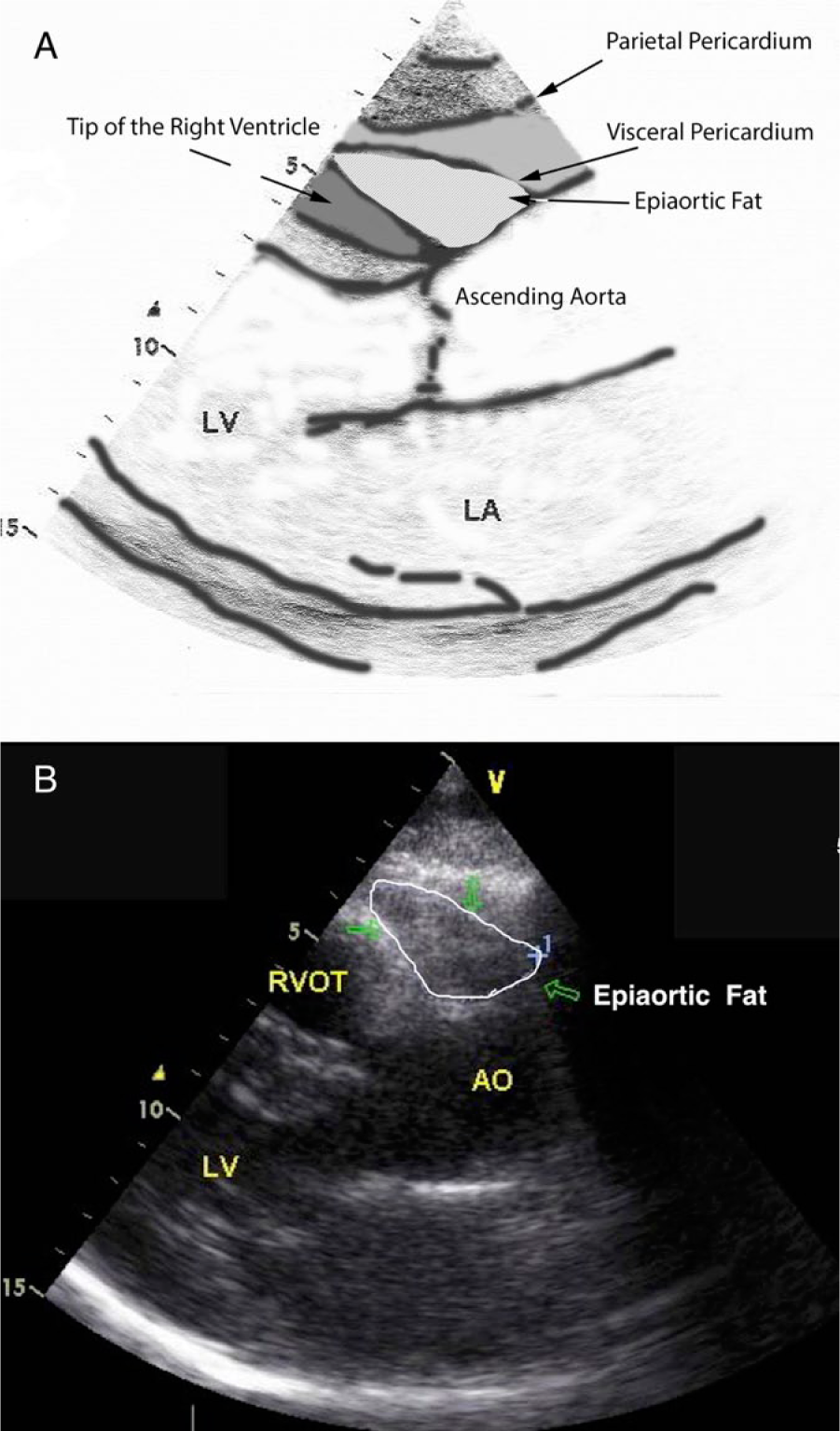
(A) Schematic drawing showing the anatomical boundaries of the epiaortic fat pad. (B) Measurement of the area of the epiaortic fat pad which was 5.45 cm2 in the case depicted. (AO, aorta; LA, left atrium; LV, left ventricle; RVOT, right ventricular outflow tract.)
Reliability analysis
In order to evaluate the inter-observer reliability of the measurement of the size of the EAFP, 20 additional subjects who met the inclusion criteria were examined. A third cardiologist, who was blinded to the measurements performed by the two other cardiologists, reviewed the echocardiography studies of the cases and repeated the measurements. The intraclass correlation coefficient was 0.921 with 95% confidence interval (CI): 0.952–0.992 (p-value <0.001).
Statistical analysis
Data obtained from the early parts of this study were used as the pilot to calculate the sample size. The AR diameter was used as the primary outcome variable for sample size determination. Patients were divided into two equal groups based on the median value of the area of the EAFP, which was calculated as 4.71 cm2. The average diameter of the AR was 2.93 cm for the patients with an EAFP ⩽4.71 cm2 and 3.27 cm for those with an EAFP >4.71 cm2. With a standard deviation of 0.40 cm, a total of 14 patients were required in each group to obtain a power of 0.80. All collected data were entered into a Microsoft Excel worksheet and transferred into SPSS® version 22.0 (IBM Inc., Chicago, IL, USA) for statistical analysis. Numerical data were expressed as mean ± standard deviation and categorical variables were reported as frequency with percentage. Independent two-tailed t-tests were used to compare the means for various groups. Univariate linear regression was used to predict each absolute and indexed diameter using the measured area of the EAFP. Furthermore, a multivariate linear regression model was constructed to identify the coefficients for the predictors of the size of the EAFP. Null hypotheses were rejected with a 95% CI and alpha error of 0.05.
Results
A total of 250 individuals were approached. Fifty-seven subjects were excluded from enrollment (32 for a history of hypertension and 25 for specific findings on TTE which were mentioned in the exclusion criteria). After the exclusion process, 193 individuals, including 70 men and 123 women, were enrolled in this prospective study. The mean age of participants was 47.5 ± 15.6 years. Demographic data and baseline characteristics of the study population are summarized in Table 1.
Demographic data and general study variables.
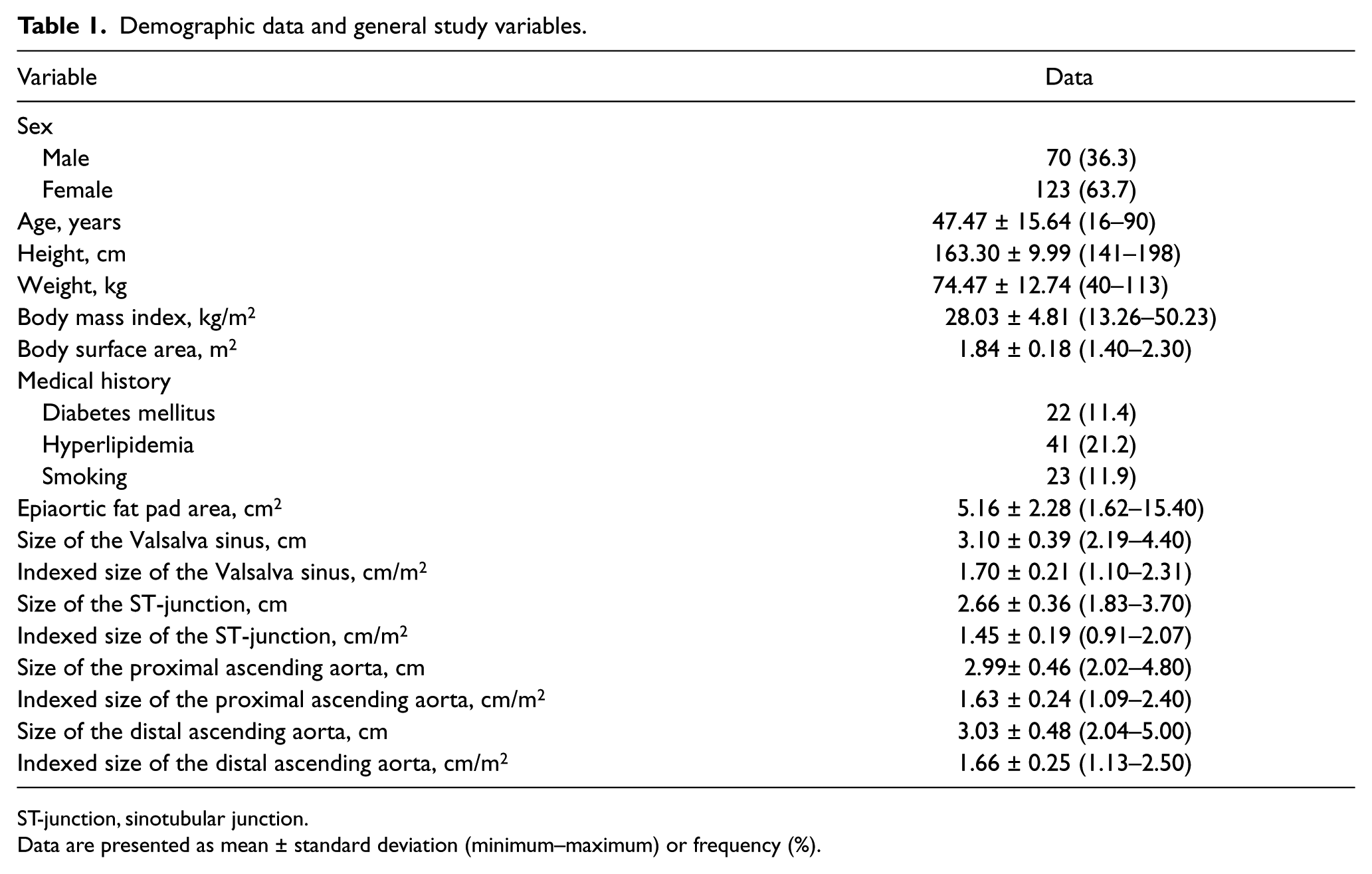
ST-junction, sinotubular junction.
Data are presented as mean ± standard deviation (minimum–maximum) or frequency (%).
In univariate linear regression, EAFP positively correlated with absolute dimensions of AR (r = 0.420), STJ (r = 0.419), AA3 (r = 0.482) and AA5 (r = 0.460) (p-value 0.001 for all). For each 1-cm2 increase in EAFP, the absolute dimension of AR increased by 0.72 mm, STJ increased by 0.66 mm, AA3 increased 0.97 mm and AA5 increased 0.97 mm. In univariate linear regression, EAFP positively correlated with indexed dimensions of AR (r = 0.295), STJ (r = 0.317), AA3 (r = 0.393) and AA5 (r = 0.376) (p-values were all <0.001). For each 1-cm2 increase in EAFP, the indexed dimensions of AR increased by 0.28 mm, STJ increased by 0.26 mm, and AA3 and AA5 increased by 0.42 mm. Table 2 shows univariate linear regression analysis of EAFP in predicting the absolute and index values of AR, ST-junction and aortic diameter at a distance of 3 cm and 5 cm from the aortic annulus. Figures 2 and 3 show the linear correlation between EAFP and the absolute and indexed diameters of the AR, STJ and ascending aorta at 3 cm and 5 cm distal the aortic annulus, respectively.
Univariate linear regression analysis of epiaortic fat pad area in predicting the absolute and index values of aortic root, sinotubular junction and aortic diameter at 3 cm and 5 cm distal to the aortic annulus.
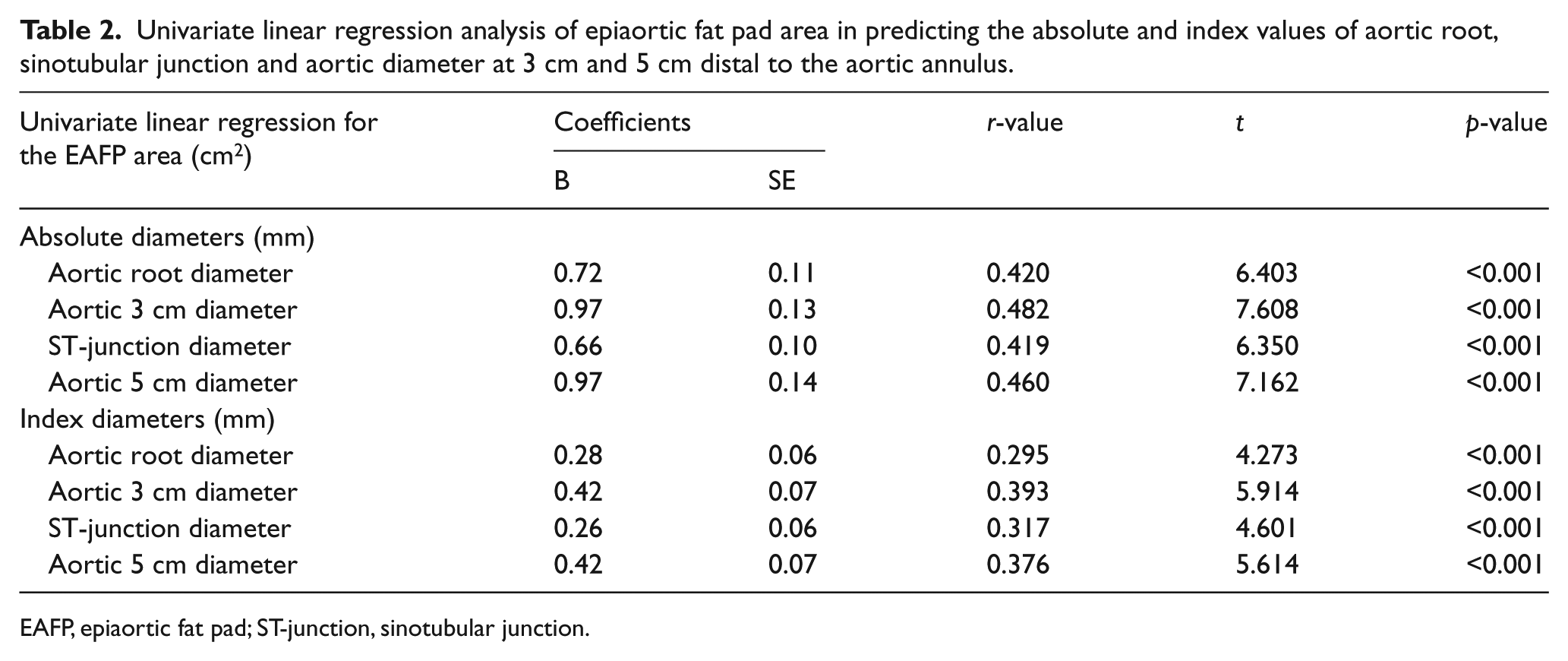
EAFP, epiaortic fat pad; ST-junction, sinotubular junction.
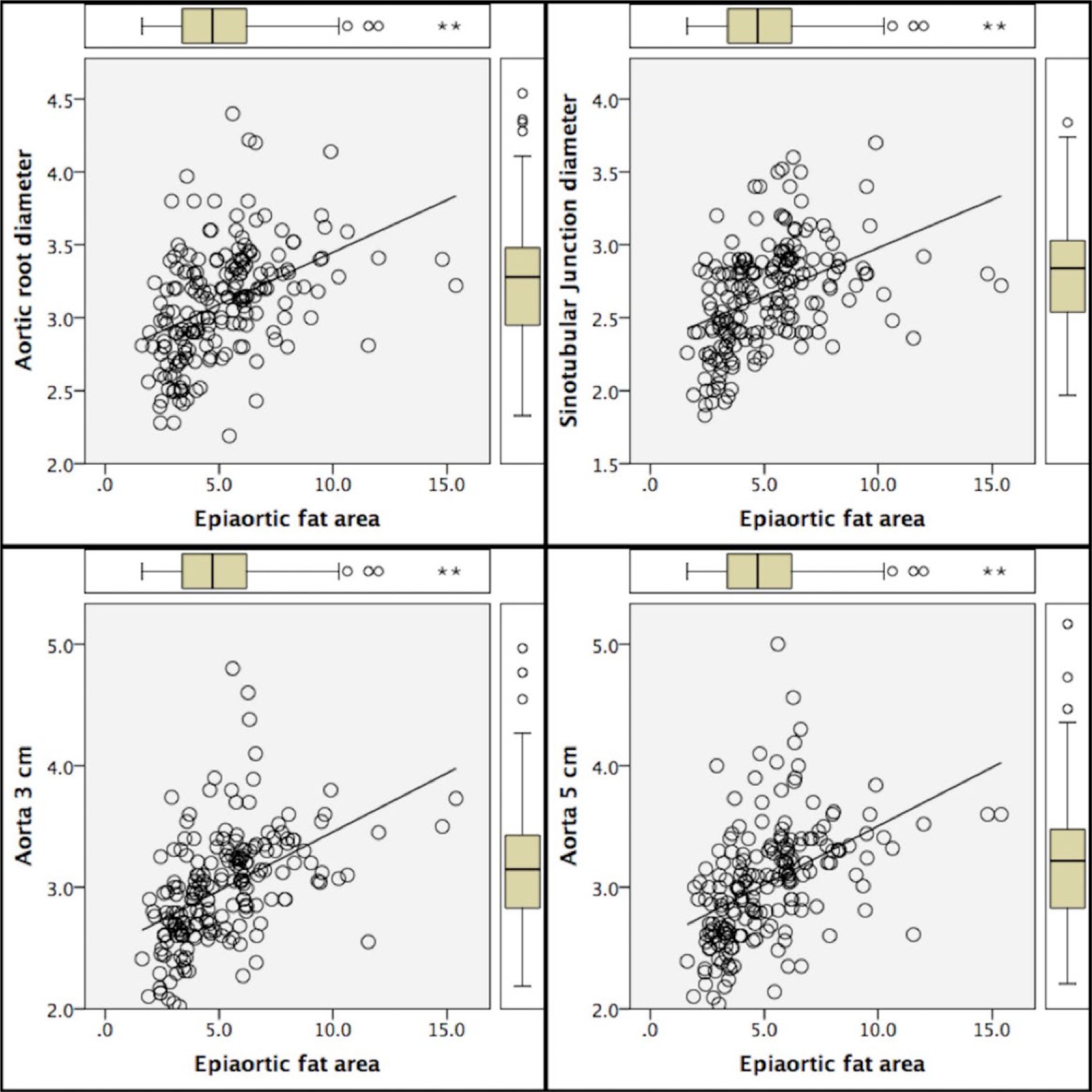
Linear correlation between the epiaortic fat pad (EAFP) and the diameters of the aortic root (AR), sinotubular junction (STJ) and ascending aorta at 3 cm and 5 cm distal to the aortic annulus.
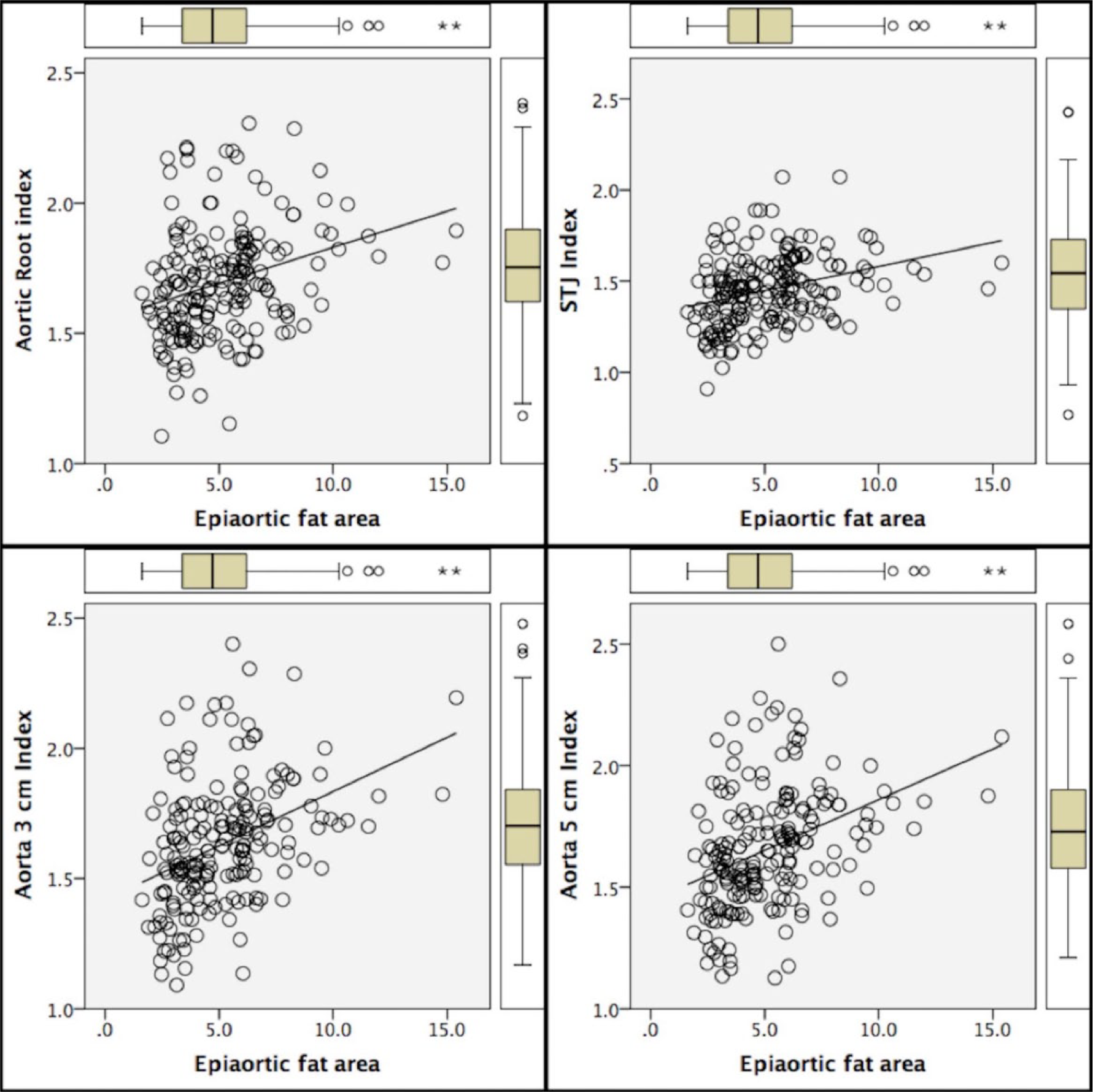
Linear correlation between the epiaortic fat pad (EAFP) and the indexed diameters of the aortic root (AR), sinotubular junction (STJ) and ascending aorta at 3 cm and 5 cm distal to the aortic annulus.
Table 3 shows the univariate linear regression of multiple independent factors associated with the size of the EAFP area (cm2). History of diabetes mellitus (p-value = 0.026), history of hyperlipidemia (p-value <0.001), age >65 years (p-value <0.001) and a body mass index (BMI) >30 kg/m2 (p-value <0.003) had a significant correlation with greater EAFP. In contrast, gender and smoking status were not associated with the size of EAFP in univariate analysis. Multivariate linear regression analysis was performed to identify the confounding factors that contribute to the size of EAFP. Despite the trend in multivariate analysis, in smaller dimensions of EAFP among female patients, there was no gender difference in the size of EAFP (p-value = 0.076). A BMI over 30 kg/m2, age >65 years and a history of hyperlipidemia were also identified as independent predictors of EAFP (p-values = 0.020, <0.001 and 0.003, respectively). Table 4 shows the multivariate regression analysis results for identification of the independent factors for prediction of EAFP.
The t-test and univariate linear regression of multiple independent factors associated with the size of the epiaortic fat pad area (cm2).
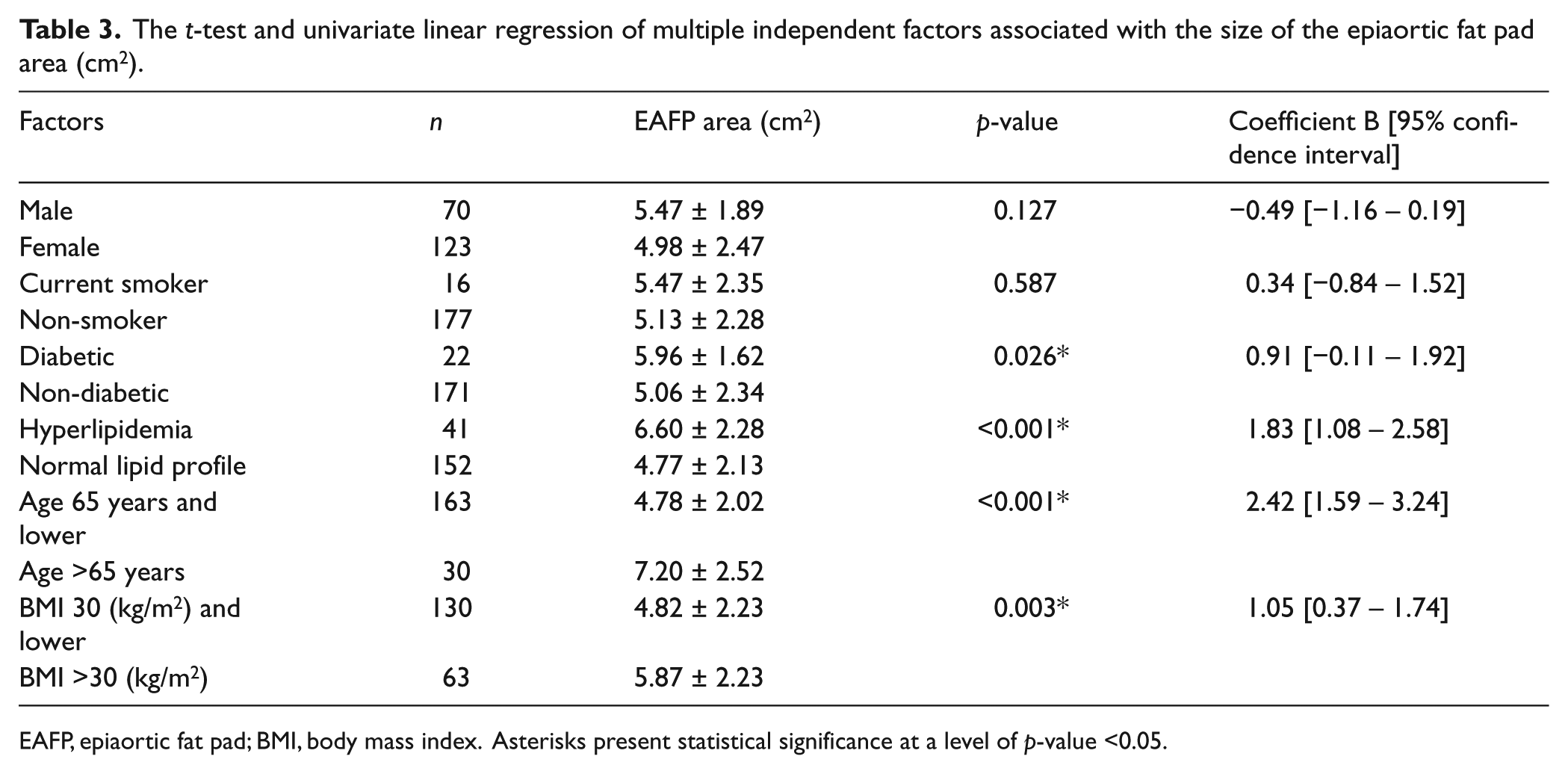
EAFP, epiaortic fat pad; BMI, body mass index. Asterisks present statistical significance at a level of p-value <0.05.
Multivariate linear regression model predicting the area of the epiaortic fat pad.
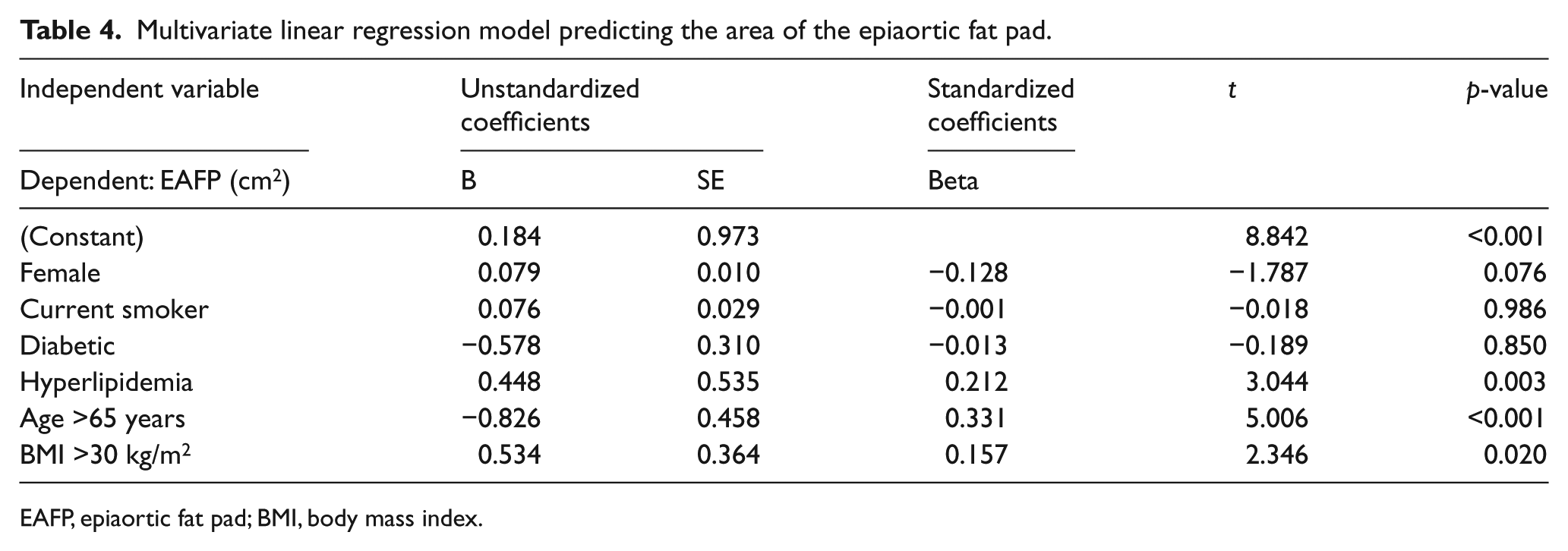
EAFP, epiaortic fat pad; BMI, body mass index.
Discussion
According to our findings, the size of the EAFP correlates with the dimensions of the underlying ascending aorta at the different segments that directly come into contact with it. Perivascular adipose tissue is considered an ectopic fat deposit with a predominantly local effect. 10 This tissue originally has anticontractile properties, which are lost with the development of obesity. 11 Periaortic fat is considered a subtype of perivascular adipose tissue. 10 Reduced differentiation of adipocytes, higher levels of inflammatory cytokine production, and down-regulation of anti-inflammatory adipokines is reported in periaortic adipose tissue of atherosclerotic aorta. 3
In a study by Britton et al., a higher periaortic fat volume was associated with a worse metabolic profile for cardiovascular disease. 12 In another study, the periaortic fat was associated with the presence of cardiovascular risk factors even after it was adjusted for BMI. 13 The association was also demonstrated between periaortic fat and abdominal aorta and coronary calcium. 14 In a study on obese mice, there was evidence for increased macrophage infiltration and cytokine expression in the adipose tissue surrounding the aorta, which led to aneurysmal changes of the abdominal aortic wall. 15
Britton et al. examined the correlation of excessive thoracic periaortic fat with the prevalence of cardiovascular risk factors in 3246 patients who were originally enrolled in the Framingham Heart Study. 12 These investigators demonstrated a higher prevalence of excessive periaortic fat in patients with advanced age, higher BMI and waist circumference, and those who were diagnosed with metabolic syndrome. 12 Similarly, in our study, higher BMI (>30 kg/m2), advanced age (>65 years) and history of hyperlipidemia were identified as independent predictors of greater EAFP. Our findings are consistent with the growing body of published reports suggesting a local effect of perivascular adipose tissue. Perivascular adipose tissue and visceral adipose depot are shown to associate with microvascular dysfunction and aortic stiffness beyond generalized body adiposity. 16
Periaortic adipose tissue quantification has been subject of a number of studies and different methods have been proposed for its measurement. Schlett et al. proposed a protocol for volumetric quantification of periaortic adipose tissue using non-contrast enhanced multi-detector computerized tomography (CTA). 7 This protocol was used in a number of studies.2,6,12,14,17 Cardiac magnetic resonance imaging (cMRI) also has been used for quantification of periaortic adipose tissue volume. 13 While the routine application of CTA and cMRI in clinical practice is not feasible, TTE is a non-invasive, relatively inexpensive and readily available method. Quantification of thoracic periaortic fat volume is not feasible with TTE. However, the anterior portion of EAFP can easily be measured.
It is postulated that periaortic adipose tissue serves as a local source of proinflammatory cells and cytokine mediators with ensuing inflammation leading to aortic remodeling and subsequent dilation.6,18 The correlation of thoracic periaortic and epicardial adipose tissue with the dimensions of the ascending aorta has been examined in two studies.5,6 Canga et al. report a greater thickness of epicardial adipose tissue, measured by TTE, in patients with a relatively larger ascending aorta diameter. 5 One large study has examined the correlation of periaortic fat volume and dimensions of aortas in more than 3000 patients. The authors report that the periaortic fat volume correlates with the dimensions of both thoracic and abdominal aorta. 12 The observed correlation persists even after adjustment for age, gender and BMI. Although the exact mechanism for this association is not clear, the paracrine effects of local growth factors and passive thermogenic effects are mentioned as the likely causes of aortic remodeling.11,18–21 In fact, epicardial adipose tissue serves as perivascular adipose tissue for coronary arteries, 22 and affects atherogenesis. 23 Interestingly, the absence of epicardial fat or separation of segments of coronary artery by a myocardial bridge may prevent the development of atherosclerotic plaques in the related segments. 24
The correlation of EAFP with the dimensions of the ascending aorta was also examined and a significant correlation between EAFP and absolute/indexed dimensions was observed. The area of EAFP could serve as a clinically applicable substitute for the periaortic fat volume. Latest guidelines from the ASE and the EAE emphasize that the dimensions of the AR should be adjusted for the BSA. 7 The basis for this recommendation was due to the fact that the dimensions of the AR correlate with BSA and advanced age. Interestingly, both of these factors affect the extent of fat deposition around the aorta.12,13,25 Since a lower BSA is shown to correlate with a higher incidence of adverse events in aortic aneurysms, the use of indexed dimensions is superior and far more informative than providing absolute diameters of the aorta. 11 Additionally, the index values take BSA into account and correct the aortic dimensions for individual body habitus. 11 It was found that the correlation between the area of EAFP and dimensions of the ascending aorta remains significant even if indexed dimensions are evaluated.
Establishment of the existing correlation between EAFP and dimensions of the ascending aorta could have potential clinical application. Longitudinal studies could shed light on the possible predictive value of the extent of EAFP and the rate of increase in dimensions of the dilated ascending aorta and possibly aortic aneurysms. Though multi-detector CT imaging has established its place for quantification of periaortic fat volume for research purposes, introducing a surrogate index that can easily be obtained by TTE (more feasible in point-of-care testing) would be advantageous. Whether greater periaortic adipose tissue could identify the subgroups of patients with more rapid progression of aortic dilation remains an area for further research.
Limitations
We did not correlate EAFP area measurements in TTE with periaortic fat volumes reported in CT/MRI scans. This correlation needs to be investigated in future studies. Moreover, we do not have any follow-up data. Therefore, no conclusion regarding the effect of EAFP on the rate of progression of the dimensions of the ascending aorta can be drawn. Our study population consisted of healthy volunteers who presented with normal aortic dimensions. Further studies focusing on patients with aortic pathology/aneurysms are warranted.
Conclusion
Both absolute and indexed diameters of the ascending aorta at the different segments that directly come into contact with EAFP linearly correlate with the area of EAFP measured by TTE.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.