
Abstract

A 39-year-old male was referred to our cardiovascular clinic because of an ankle–brachial index (ABI) that was lower on the left side than on the right side (0.84 vs 1.1) at a routine health examination. He denied claudication but did relate congenital thinning of his lower abdominal wall combined with erectile dysfunction, urinary dribbling, left-sided penile deviation, and azoospermia.
Physical examination was remarkable for pronounced periumbilical atrophic skin (Panel A) without rectus abdominis development but with palpable left dorsalis pedis and posterior tibial artery pulses. No left-sided peripheral aneurysms were detected. Left hemiscrotal hypoplasia and left penile deviation were noted.

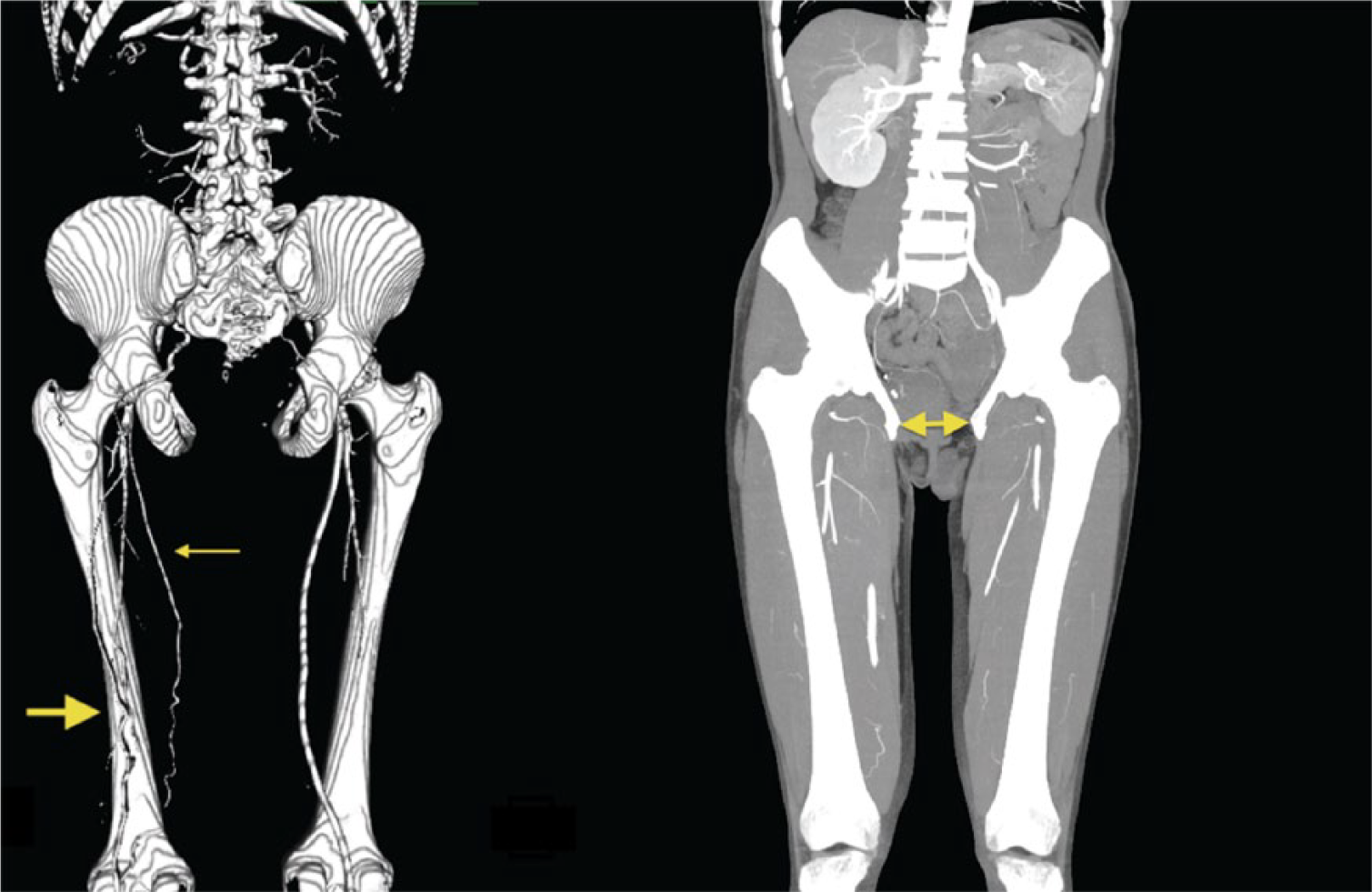
Computer tomographic (CT) arteriography with 3-D reconstruction revealed a hypoplastic left superficial femoral artery (SFA) with an anomalous persistent sciatic artery (PSA) extending to the popliteal artery (Panel B, left, thin arrow: SFA; thick arrow: PSA). The left anterior tibial, posterior tibial, and peroneal arteries were patent. Additional CT abnormalities included left renal agenesis and absence of the pubic symphysis (Panel B, right, double arrow: left renal agenesis and absence of pelvic symphysis).
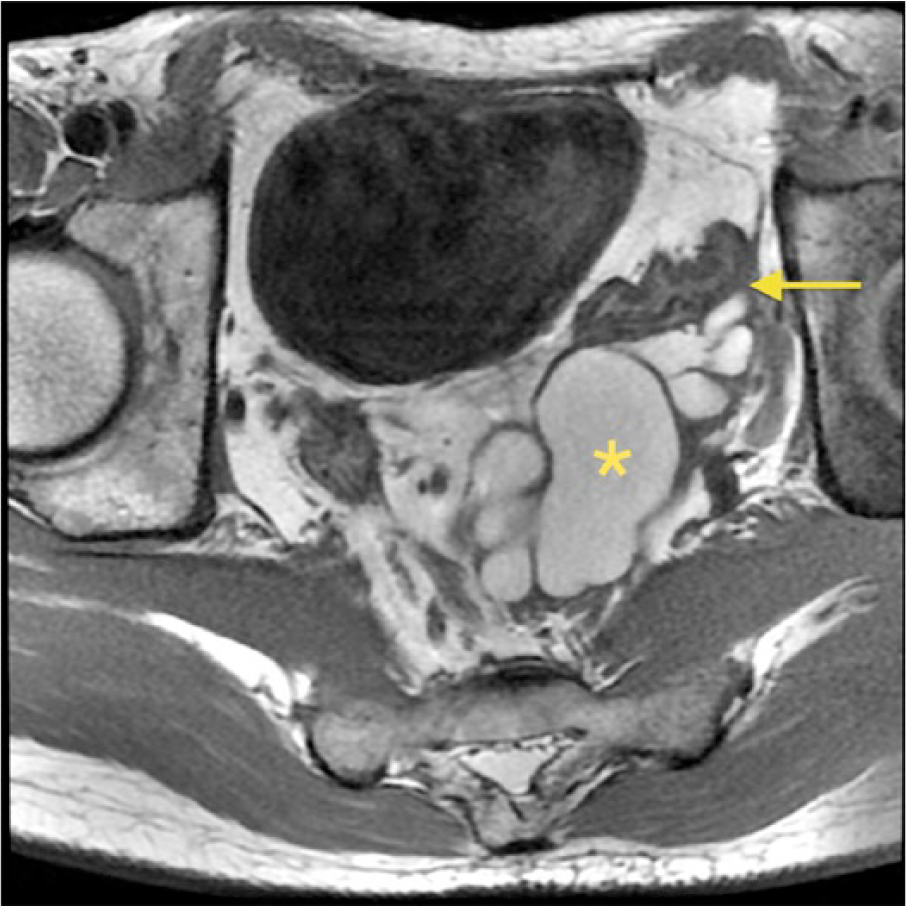
Magnetic resonance imaging (MRI) of the pelvis displayed a 7.9 × 7.4 × 7.6-cm multiloculated, thin-walled cystic structure behind the urinary bladder suggestive of a seminal vesicle cyst (Panel C, asterisk: left seminal vesicle cyst; arrow: left vas deferens, T1 weighted with fat saturation, axial). Urinary bladder exstrophy, hypoplasia of the left corpus cavernosum, absence of pubic floor musculature, left gonadal vein engorgement, and dysplasia of the abdominal wall were also noted.
The relationship between PSA and genitourinary anomalies is unclear, but may be embryologic in nature. 1 During embryonic development, both sciatic and primary renal arteries branch off from the common iliac artery. PSA is likely due to maldevelopment of the distal mesonephric duct. Moreover, our patient also suffered from (left side) maldevelopment of the urogenital sinus and fold that failed to mature into the urinary bladder and penis. PSA may be explained by a defect in the lower abdominal wall (failure of mesenchymal cells to migrate between the surface ectoderm and the urogenital sinus during the 4th gestational week). 2 Genitourinary tract anomalies should be suspected when a PSA is diagnosed and further evaluated if clinically indicated. Since the PSA was diagnosed without symptoms of claudication or an associated aneurysm, observation was recommended.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.