
Abstract

An 84-year-old male presented with a 6-month history of progressive swelling of the distal left lower limb. Notable history included bilateral popliteal artery bypasses performed many years previously for popliteal aneurysmal disease. Peripheral vascular examination revealed strong femoral pulses but absent popliteal, dorsalis pedis and posterior tibial pulses bilaterally. As well as features of chronic arterial insufficiency, a left-sided popliteal fossa mass was noted along with venous congestion and pitting oedema to the mid-thigh.
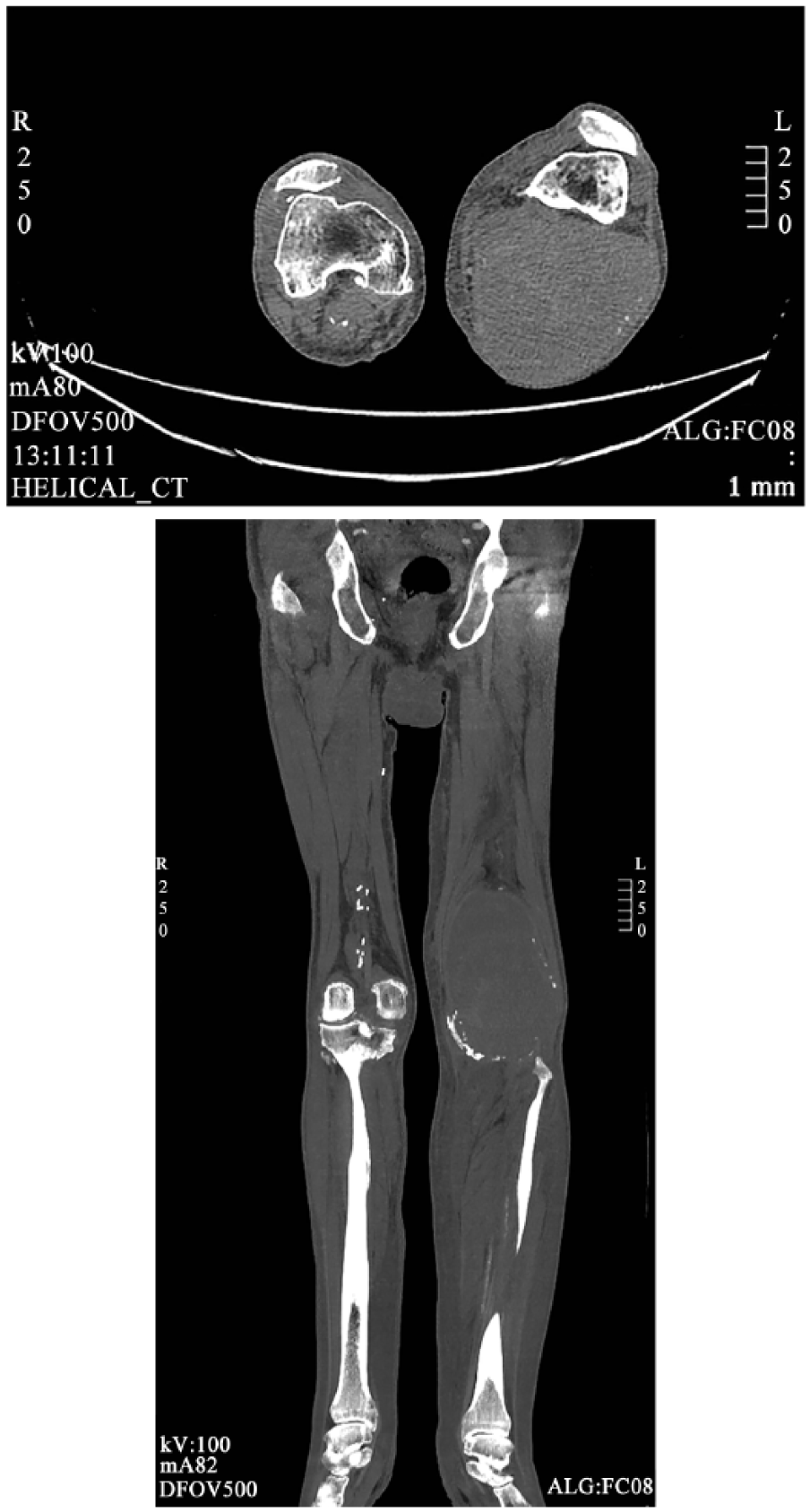
Ultrasound compression venography was performed, demonstrating compressible veins in the left groin and distal thigh. A 13.5 × 7.5 × 9.5-cm mass in the left popliteal fossa (Panel A) was suggestive of a partially thrombosed aneurysm with persistent inflow. The popliteal vein could not be identified due to extraneous compression, with distal veins similarly compressed due to oedema. Subsequent computed tomography angiography demonstrated a patent left common iliac diameter of 3.3 cm, with good perfusion of both profunda femoral and superficial femoral arteries (SFA). The popliteal artery was demonstrated to occlude above the aneurysm, now measuring 10.7 cm transversely and 18 cm craniocaudal (Panels B-1 and B-2), with faint three-vessel runoff.

Elective decompression and ligation with a view to popliteal bypass was planned. Previous operative scars were excised and proximal SFA was controlled via a distal thigh incision. Intraoperative findings revealed a giant 25 × 15 × 15-cm aneurysmal sac, which was decompressed and explored with ligation of two inflow vessels using 3.0 Prolene. Absence of flow was initially noted in the anterior tibial and tibial-peroneal trunk; however, this was spontaneously restored with strong biphasic flow noted on intraoperative Doppler assessment. Given the unexpected patency of the original bypass graft following decompression, no further intervention was deemed necessary, and the wound was closed with vacuum drains left in the approximated cavity. No immediate or early postoperative complications were noted.
Popliteal artery aneurysms account for 70% of peripheral aneurysms, and have a notable association with abdominal aortic aneurysms in around 30% of cases. 1 Although no definitive pathophysiological process is attributed to aneurysm formation, important aetiological factors may include atherosclerosis, genetic predisposition and haemodynamic stress. 2 Current suggested management includes open surgical ligation and popliteal bypass; however, this remains under contention.3,4 This case highlights how ligation and bypass does not reliably abolish collateral circulation, which can lead to future sac expansion and rupture as well as the need for operator dynamism during vascular surgery.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.