
Abstract
Patients on hemodialysis (HD) have abnormalities of calcium-phosphate (CaP) homeostasis and high CaP product contributes to atherosclerosis pathogenesis and adverse events. Patients on HD with critical limb ischemia (CLI) are at risk for major amputation and death because of advanced systemic atherosclerotic disease. The aim of this study was to evaluate the relationship between CaP product and amputation-free survival (AFS) in CLI after endovascular treatment (EVT). We retrospectively analyzed 221 CLI patients on HD. In Kaplan–Meier analysis, AFS was significantly lower in patients with CaP product ⩾55 mg2/dL2 compared to those with CaP product <55 mg2/dL2 (54.3% vs 78.5%, p = 0.002). However, neither serum phosphate nor calcium levels were individually associated with AFS. In multivariate analysis, CaP product ⩾55 mg2/dL2 was an independent predictor for AFS in CLI patients on HD (hazard ratio, 3.03; 95% confidence interval, 1.78–5.15; p-value <0.001). We concluded abnormal CaP homeostasis was associated with lower AFS after EVT in CLI patients on HD, and can serve for their risk stratification.
Introduction
Patients with chronic kidney disease (CKD) are at high risk for advanced atherosclerosis and cardiovascular disease compared with patients without CKD; 1 23–45% of patients with hemodialysis (HD)-dependent advanced CKD have peripheral artery disease (PAD).2–4 Critical limb ischemia (CLI) is the most advanced manifestation of PAD with rest pain and/or tissue loss, and CLI patients on HD have significantly lower major amputation-free 5 and overall survival 6 compared to CLI patients without HD. Abnormalities of serum calcium and phosphorus are commonly found in patients with CKD in association with cardiovascular calcification and arterial dysfunction, 7 and higher serum phosphorus levels and the calcium-phosphate (CaP) product are associated with mortality in the overall population on chronic HD. 8 Little is known about the association of abnormalities of CaP homeostasis with adverse events after endovascular therapy (EVT) in CLI patients on HD, which is the subject of this study.
Methods
Study population
This retrospective study used data from a physician’s database of two centers (Shinshu University School of Medicine and Kansai Rosai Hospital) in Japan on 221 consecutive CLI patients (290 limbs) on HD who underwent EVT between March 2012 and July 2013, after excluding patients who refused revascularization, presented with acute limb ischemia, or were unable to provide consent. Demographic, clinical features and medical history were extracted including age, gender, lower limb characteristics, activities of daily life before EVT (non-ambulatory status was defined as wheelchair use or being bedridden), prior coronary artery disease or cerebrovascular disease, presence of concomitant atherosclerotic risk factors and medications. The study protocol was developed in accordance with the Declaration of Helsinki and approved by the ethics committee of each center. All patients gave written informed consent prior to revascularization.
Outcomes
The primary outcome of this study was amputation-free survival (AFS), defined as freedom from major amputation or all-cause death, at 1 year. Major amputation was defined as above-ankle amputation of an index limb. All-cause death was determined from the database of each hospital or confirmed by telephone call.
Assessment of kidney function and measurement of calcium and phosphorus
Estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease formula 9 at admission. Duration of HD was calculated from the date of the start of HD to the date of final follow-up. The primary causes of HD were collected from medical records. All participants underwent dialysis thrice weekly (Monday, Wednesday, and Friday, or Tuesday, Thursday, and Saturday).
Until now, there was no consensus for specific timing of blood samples to assess serum calcium and phosphorus. Based on a previous report, serum phosphorus levels measured on Monday or Thursday were significantly higher than those measured midweek, particularly in CKD on dialysis. 10 Therefore, we collected all blood samples to measure serum creatinine, calcium, and phosphorus levels in the morning in a fasting state on Monday or Thursday, 3 days after the last dialysis. Serum phosphorus and calcium levels were measured using a standard colorimetric method and an autoanalyzer (Hitachi, Tokyo, Japan). The CaP product (in mg2/dL2) was calculated by multiplying the serum calcium level (in mg/dL) by the serum phosphate level (in mg/dL) on admission. 8 Kidney Disease Outcomes Quality Initiative (KDOQI) clinical practice guidelines recommended that serum corrected calcium should be maintained at <10.2 mg/dL, serum phosphate should be maintained at <5.5 mg/dL, and serum CaP product should be maintained at <55 mg2/dL2 in patients on HD. 11 In this study, we used these cut-off values to assess the relationship of CaP homeostasis with adverse outcomes in CLI patients on HD.
Assessment of limb status and approach of revascularization
CLI was defined on the basis of the TransAtlantic Inter-Society Consensus (TASC) guidelines, 12 including tissue loss or ischemic rest pain lasting over 2 weeks with an absolute ankle pressure <50 mmHg or a toe pressure <30 mmHg. Tissue loss was evaluated by a plastic surgeon, interventional cardiologist, or vascular surgeon who recorded the location and extent of non-healing ulceration or gangrene. The ankle–brachial index (ABI) and skin perfusion pressure (SPP) was regularly measured to assess the hemodynamic status of the lower limb before revascularization. SPP <40 mmHg indicated the presence of ischemia leading to tissue loss or rest pain. Lower-extremity angiography was performed on all patients to assess the location and severity of arterial obstruction compromising flow to the wound bed. Indication of EVT for TASC II D lesions was decided by consensus among vascular team members depending on comorbidity factors and the general condition of the patient. EVT strategy was left to the operator’s discretion at each participating center. 12 All procedures were performed based on the angiosome concept, 13 and procedural success was defined as the achievement of one-straight-line flow without any flow limitation. If the angiosome-based revascularization failed, EVT of a non-angiosome-based lesion was performed to achieve the previously reported wound blush. 14 Dual antiplatelet therapy (aspirin at 100 mg/day and clopidogrel at 75 mg/day or cilostazol at 200 mg/day) was started prior to EVT. Medical treatment for risk factors of atherosclerosis, including hypertension, hyperlipidemia, and diabetes, was performed at the discretion of their physician.
Statistical analysis
Continuous variables are presented as mean ± SD if normally distributed and as median and interquartile if not normally distributed. Normality was assessed by the Shapiro–Wilk W test. Categorical variables are described as number and percentage. Differences in continuous variables among the patient groups according to CaP product were compared by Wilcoxon or Kruskal–Wallis tests, while proportions were compared using contingency table analysis. A Kaplan–Meier test was performed to assess cumulative major amputation or mortality rate in the study population. The log-rank test was used to compare survival curves. Multivariate Cox regression analysis was performed to determine predictors for major amputation or all-cause death. A CaP product ⩾55 mg2/dL2, and clinically specified predictors (body mass index (BMI) <18.5 kg/m2, non-ambulatory status, serum C-reactive protein (CRP) >5.0 mg/dL, serum albumin levels <3.0 g/dL and a history of heart failure) achieving p⩽0.05 in univariate analysis were entered into the multivariate Cox regression analysis. The variance inflation factor (VIF) was used to check for multicollinearity for each variable; none of the VIF values were greater than 2. Statistical analysis was performed using the Statistical Package for Social Sciences, version 21 software (SPSS Inc., Amonk, NY, USA), and a p-value of 0.05 was considered statistically significant.
Results
Baseline characteristics
Baseline characteristics of study participants are summarized in Table 1. The mean age of the overall population was 71±8 years. Among the participants, 32.6% were female and the mean duration of HD was 9.4±7.0 years. The distribution of CaP product in our population is shown in Figure 1. Lower limb and lesion characteristics are shown in Table 2. Among the 221 patients, 92.7% had tissue loss (Rutherford classification 5 or 6) and 47.1% were isolated below the knee (BTK). According to TASC II criteria, 20.3% of patients (45/109) had type C or D femoropopliteal artery lesions; according to TASC 2000 criteria, 81.9% of participants (181/197) had type D BTK lesions.
Baseline patient characteristics in the study population.
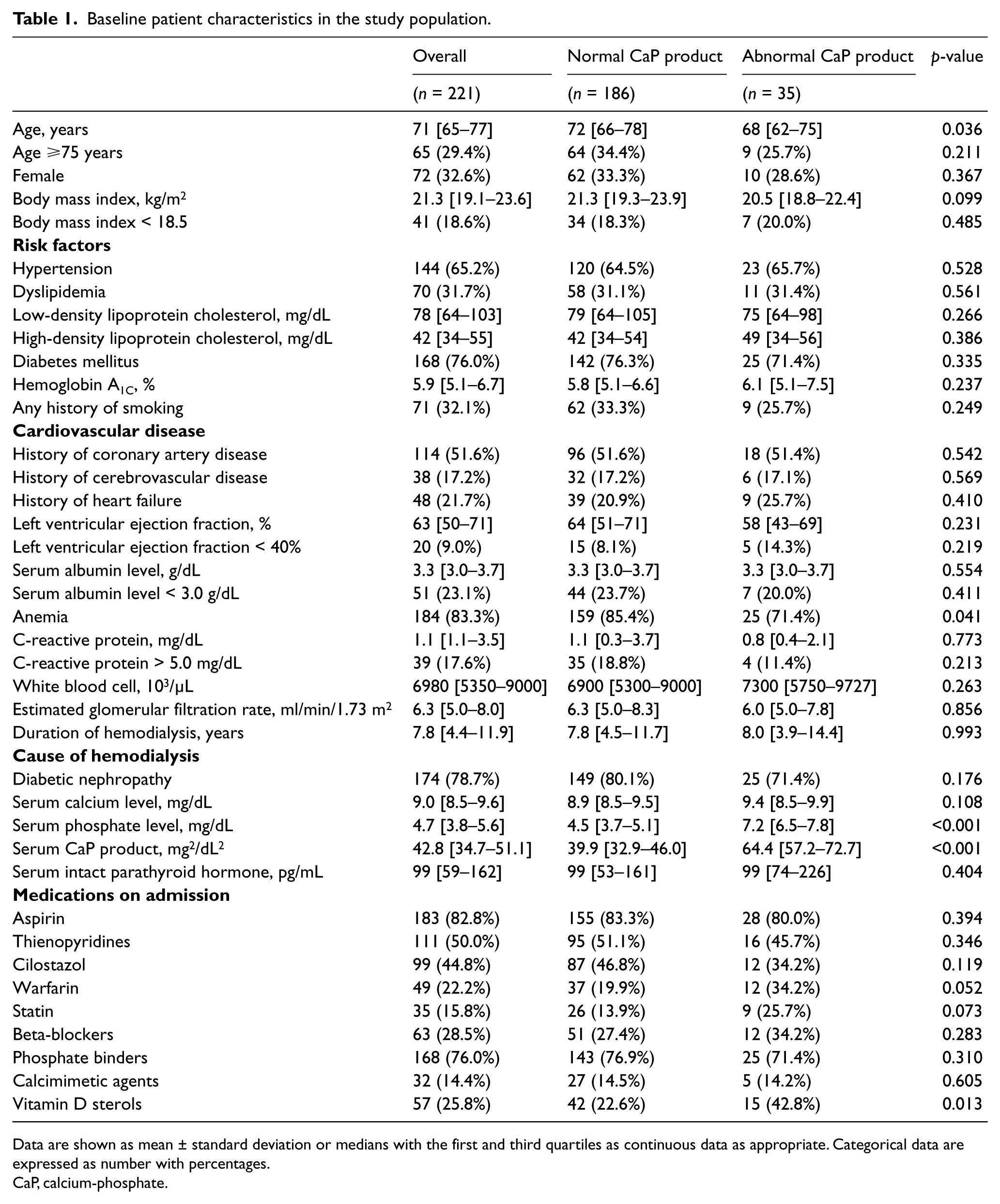
Data are shown as mean ± standard deviation or medians with the first and third quartiles as continuous data as appropriate. Categorical data are expressed as number with percentages.
CaP, calcium-phosphate.
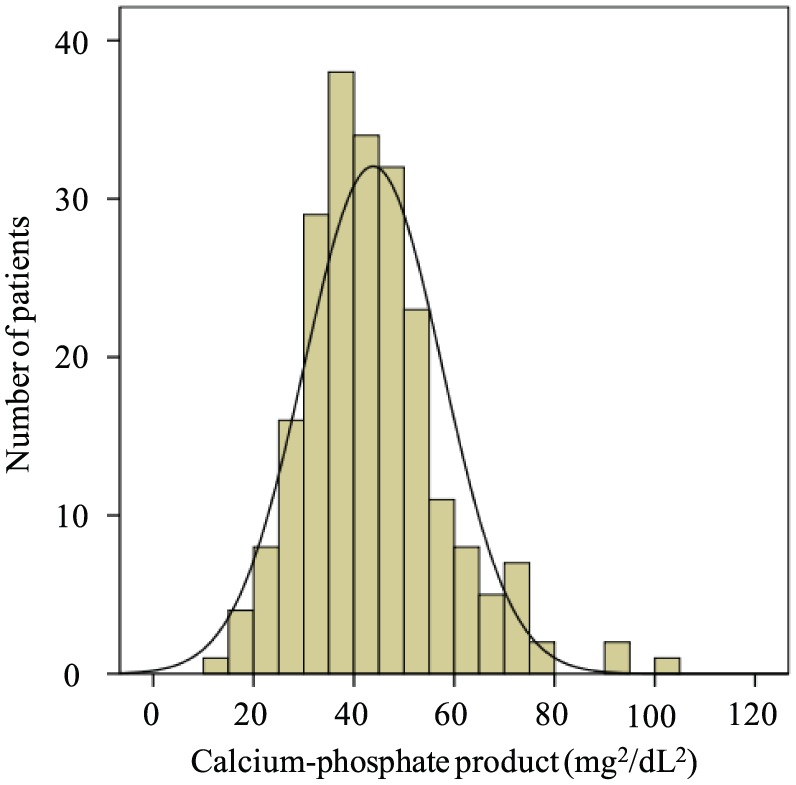
The distribution of calcium-phosphate product.
Baseline limb and lesion characteristics.
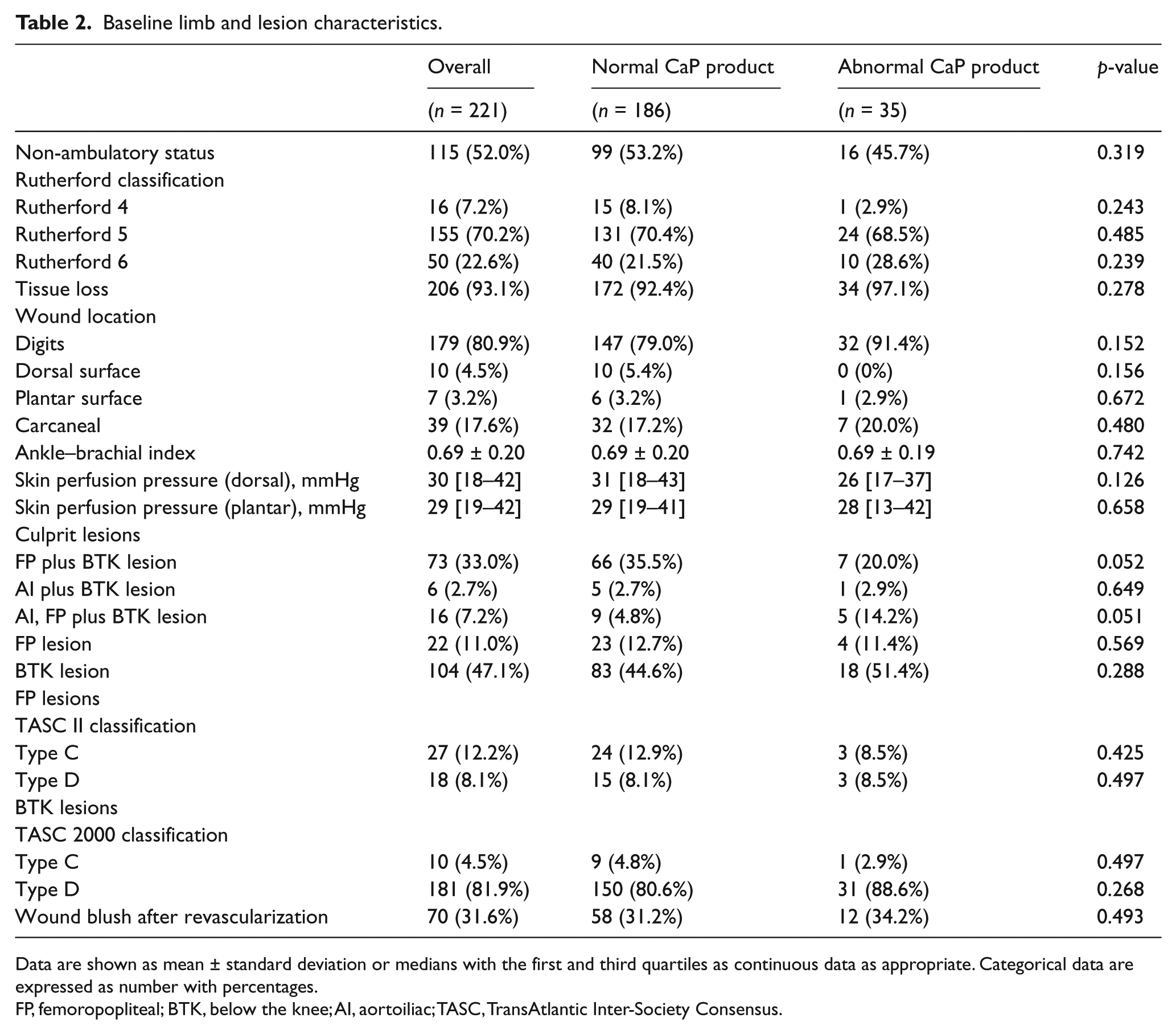
Data are shown as mean ± standard deviation or medians with the first and third quartiles as continuous data as appropriate. Categorical data are expressed as number with percentages.
FP, femoropopliteal; BTK, below the knee; AI, aortoiliac; TASC, TransAtlantic Inter-Society Consensus.
Amputation-free survival after endovascular treatment
Of 221 patients, 181 (81.9%) completed the 1-year follow-up. During the follow-up period, the incidence of major amputation and all-cause death was 25.3% (n=56), including 35 cases of all-cause death (cardiac death, 18; infection, 10; multiple organ failure, 3; respiratory failure, 2; and unknown, 2) and 21 cases of major amputation. In Kaplan–Meier analysis, AFS was not significantly different at 1 year between the patients with serum phosphorus < 5.6 mg/dL vs ⩾ 5.6 mg/dL (78.2% vs 64.3%, p = 0.063) and between patients with serum calcium < 10.2 mg/dL vs ⩾ 10.2 mg/dL (76.1% vs 60.0%, p = 0.080) (Figure 2). On the other hand, CLI patients with serum CaP product ⩾ 55 mg2/dL2 had significantly lower AFS compared to those with serum CaP product < 55 mg2/dL2 (54.3% vs 78.5%, p = 0.002) (Figure 3). We also performed Kaplan–Meier analysis according to the AFS baseline on the quartiles of CaP product (10.9–34.8 vs 34.9–42.8 vs 42.9–51.0 vs 51.1–103.2). Although there was no statistical significance, the patients with high CaP product were more likely to have a high incidence of death or major amputation than the patients with low CaP product (81.8% vs 80.0% vs 71.4% vs 65.5%, p = 0.252).
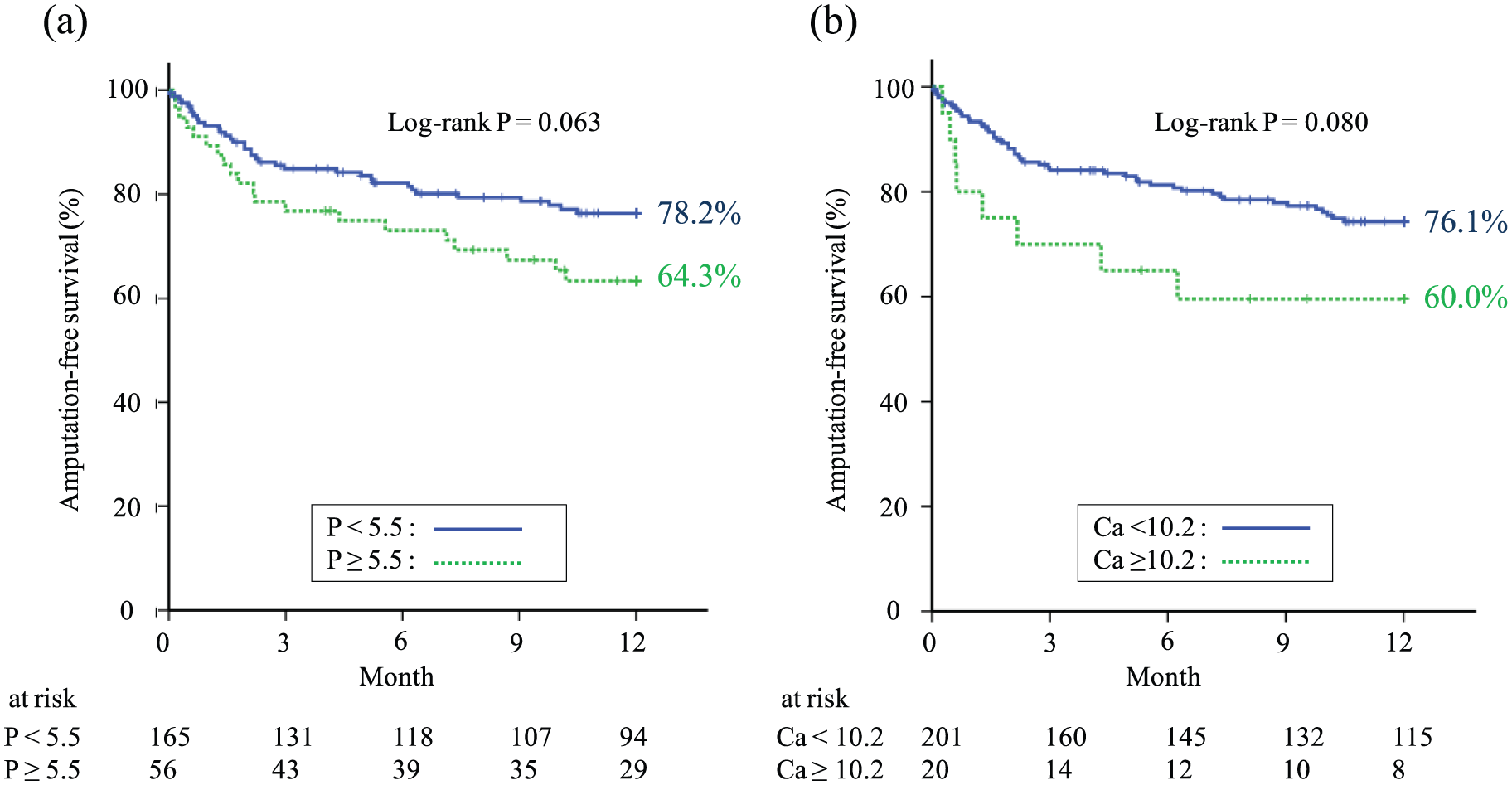
Kaplan–Meier analysis of amputation-free survival (AFS) by serum calcium level and serum phosphate level in patients with critical limb ischemia on hemodialysis. There was no significant difference in AFS between patients with serum phosphate level <5.5 mg/dL vs. 5.5 >mg/dL (A) or between patients with serum calcium level < 10.2 mg/dL vs. >10.2 mg/dL (B).
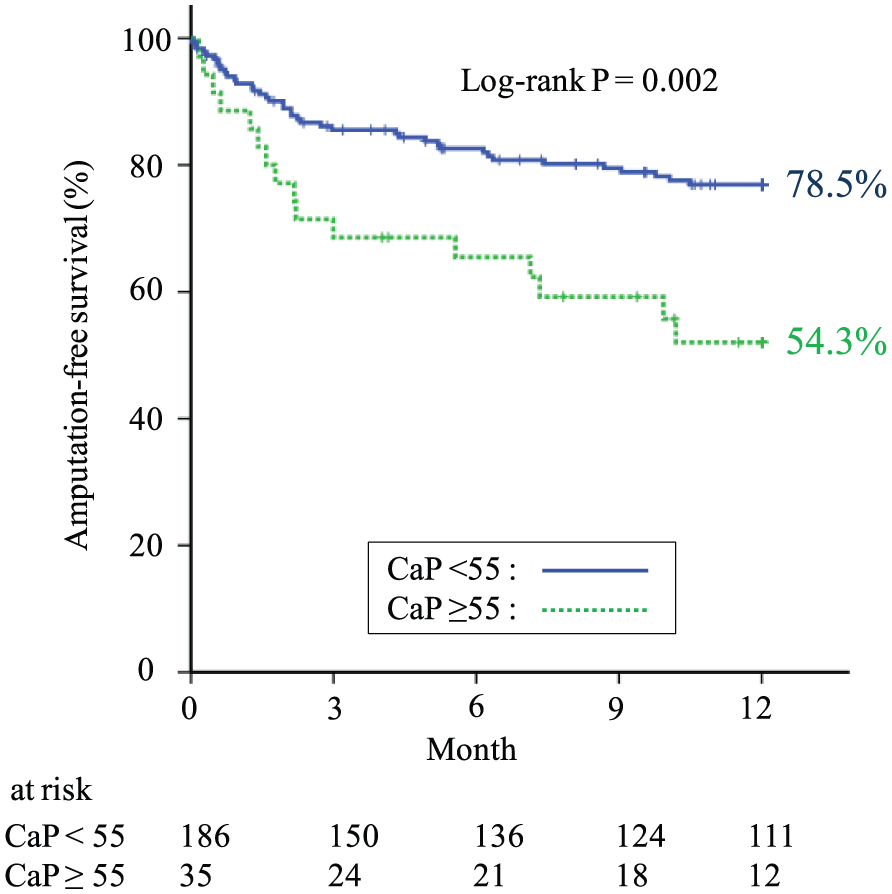
Kaplan–Meier analysis of amputation-free survival (AFS) by serum calcium-phosphate (CaP) product in patients with critical limb ischemia on hemodialysis. The patients with serum CaP product ⩾55 mg2/dL2 had significantly lower AFS compared to those with serum CaP product <55 mg2/dL2 (54.3% vs 78.5%, p=0.002).
Multivariate Cox regression analysis was performed to identify specific predictors of AFS and demonstrated that non-ambulatory status (hazard ratio [HR] 2.78, 95% confidence interval [95% CI] 1.41–5.45, p = 0.003), BMI <18.5 kg/m2 (HR 2.01, 95% CI 1.11–3.62, p = 0.021), serum albumin level < 3.0 g/dL (HR 1.96, 95% CI 1.06–3.64, p = 0.033), history of heart failure (HR 1.96, 95% CI 1.09–3.52, p = 0.024), and serum CaP product ⩾ 55 mg2/dL2 (HR 2.76, 95% CI 1.50–5.08, p <0.001) were independent predictors of major amputation or all-cause death (Table 3).
Cox-regression analysis of amputation-free survival in critical limb ischemia patients on hemodialysis.
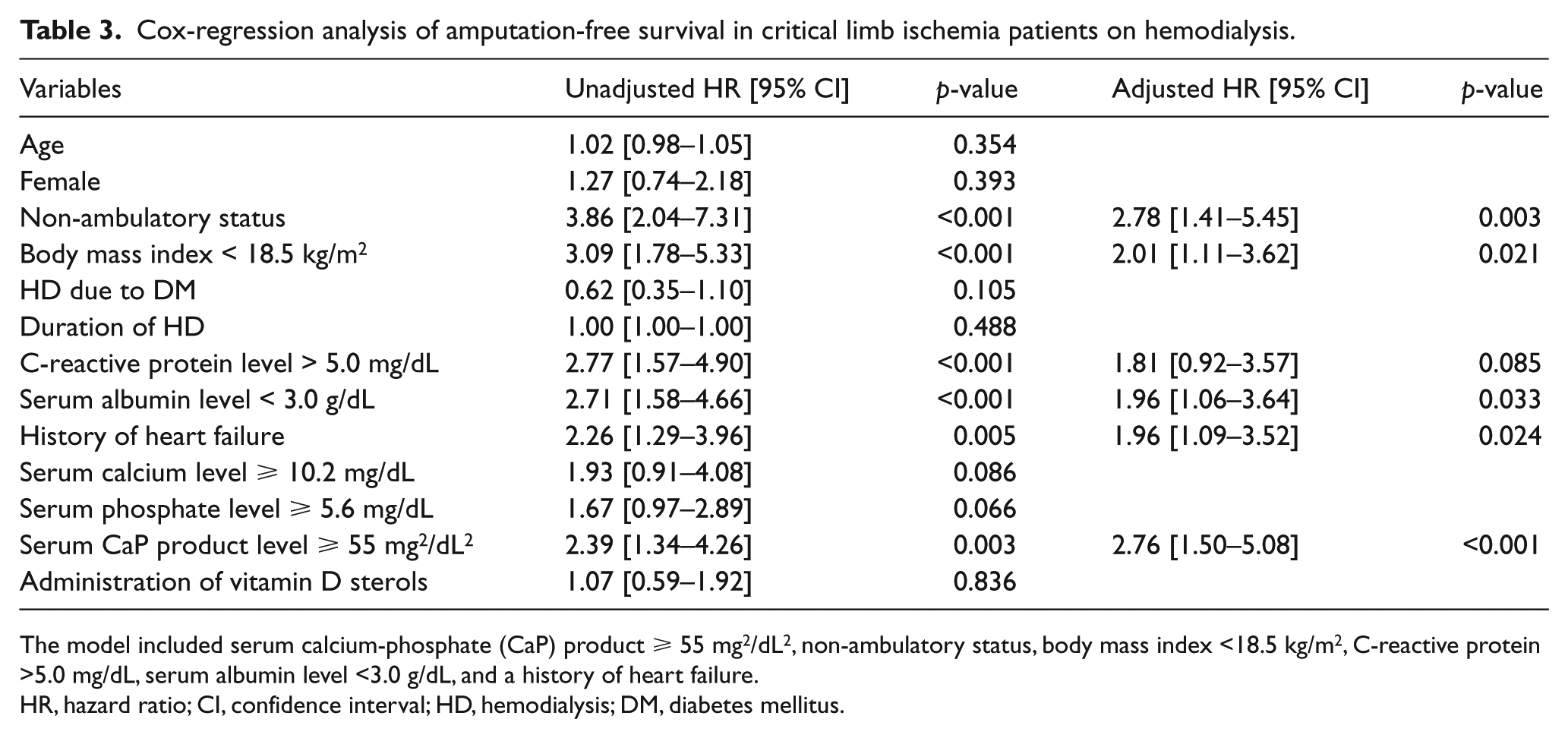
The model included serum calcium-phosphate (CaP) product ⩾ 55 mg2/dL2, non-ambulatory status, body mass index <18.5 kg/m2, C-reactive protein >5.0 mg/dL, serum albumin level <3.0 g/dL, and a history of heart failure.
HR, hazard ratio; CI, confidence interval; HD, hemodialysis; DM, diabetes mellitus.
Discussion
In the present study, CLI patients on HD with serum CaP product ⩾ 55 mg2/dL2 had significantly lower AFS compared to those with serum CaP product < 55 mg2/dL2. Our results suggest that the CaP product may be useful in identifying high-risk CLI patients on HD undergoing EVT.
Patients with CKD are at high risk for developing atherosclerosis, cardiovascular disease, 1 and PAD. 15 These subjects tend to have diabetes and are susceptible to contrast-induced renal impairment during EVT. 16 In patients on HD, an abnormality of CaP homeostasis causes high serum calcium and/or phosphorus levels in association with a high rate of cardiovascular disease. 17 Hyperphosphatemia has been thought to be the main mechanism of high CaP product. 18 High serum phosphate levels enhance the synthesis of parathyroid hormone and resulted in increased CaP product. 19 High CaP product directly increases smooth-muscle cell calcification and the expression of OSf2/Cbfa-1 and osteocalcin. 20 OSf2/Cbfa-1 is the only transcriptional activator of osteoblast differentiation, causing ectopic calcification. 21 Because of these mechanisms, high CaP product contributes to vascular calcification. Although the relationship of high serum phosphate or CaP product with pathophysiology of CLI has not been well understood, the mechanism might have significant impact on worsening atherosclerosis in patients with CLI on HD.
In this study, we found an association of elevated serum CaP product ⩾ 55 mg2/dL2 with reduced AFS among a cohort of patients with CLI on HD. Although our population was unique, an association of elevated CaP product to adverse outcomes has been reported previously in other populations. There was a difference in the patient populations studied; nevertheless, AFS at 1 year (72.9%) was relatively better than previous data even though the study included patients on HD with diverse lesions. One major possibility for the difference might be the historical background of each study. Previous studies5,21,22 enrolled CLI patients before 2010, while the present study enrolled them from 2010 to 2013; advances in CLI patients’ care have been achieved recently, and multidisciplinary care for CLI was advocated and established after 2010. 23
A previous study linked arterial calcification to an elevated serum CaP product, and patients on HD with an elevated serum CaP product have 2.5 to 5 times the coronary artery calcium score compared to non-dialysis patients. 24 The extent of coronary artery calcification has been found to add prognostic value to traditional risk factors for coronary artery disease. 25 The presence of calcification in ⩾1 coronary arteries has been shown to increase the risk of coronary death or nonfatal infarction. 26 More than half of deaths were of cardiac origin in this study; therefore, our data are consistent with those of a previous study which demonstrated that an elevated serum CaP product is associated with high mortality, particularly cardiac.
Serum CaP product is easily calculated by multiplying serum calcium and phosphate levels, which are readily determined by blood testing. Although CLI patients on HD have been recognized as a high-risk population, the current study demonstrated CLI patients on HD with a better prognosis than previous data, namely those with CaP product <55 mg2/dL2.
Limitations
There are several limitations in this study. First, this is a retrospective analysis of CLI patients on HD in two centers and it may have selection bias. Because several previous studies demonstrated that patients with high CaP product have a high incidence of adverse clinical outcomes, our results were not significantly changed from performing the current study prospectively. Second, although CaP product is highly related to the adequacy of dialysis, we did not collect data about dialysis adequacy or completeness of sessions. Third, the 1-year follow up was completed in only 81.9% of the overall population. There were no significant differences in the follow-up rate between the patients with abnormal CaP product (83.3%) and those with normal CaP product (81.6%). Fourth, complete wound healing rate and wound healing time were not investigated. The primary goal of CLI treatment is to achieve wound healing, which should be an important outcome measure in future analysis of serum CaP product. Fifth, the current study revealed that serum CaP product was an independent predictor for the adverse outcomes of major amputation or death in CLI patients on HD; further investigation is warranted to determine if this also applies to the overall CLI population and other outcomes, such as stroke.
Conclusions
We demonstrated that a high level of serum CaP product (i.e. ⩾55 mg2/dL2) was associated with poor AFS in CLI patients on HD. Even though CLI patients on HD have been recognized as a high-risk population, it is possible to further divide them into low- and high-risk groups based on the serum CaP product. Early intervention to achieve CaP homeostasis in CLI patients on HD might reduce adverse outcome occurrence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.