
Abstract
Infections of vascular grafts are associated with significant mortality and morbidity risk and cost an estimated $640 million annually in the United States. Clinical presentation varies by time elapsed from implantation and by surgical site. A thorough history and physical examination in conjunction with a variety of imaging modalities is often essential to diagnosis. For infected aortic grafts, there are several options for treatment, including graft excision with extra-anatomic bypass, in situ reconstruction, or reconstruction with the neo-aortoiliac system. The management of infected endovascular aortic grafts is similar. For infected peripheral bypasses, graft preservation techniques can be utilized, but in cases where it is not possible, graft removal and revascularization through uninfected tissue planes is necessary. Infected dialysis access can be surgically treated by complete or subtotal graft excision. Diagnosis, general management, and surgical approaches to infected vascular grafts are discussed in this review.
Introduction
Vascular graft infections occur infrequently, with an incidence that varies by surgical site but in general ranges from 0.5% to 6%. 1 The occurrence of a vascular graft infection can be catastrophic, and is associated with a significant increase in morbidity and mortality risk. The annual cost burden associated with vascular graft infections is $640 million in the United States. 1 Despite improving outcomes over the last few decades, vascular graft infections continue to pose clinical challenges to surgeons with regards to management, and several therapeutic options exist, each with their own respective advantages and disadvantages. In this review, we provide an overview of the pathogenesis, clinical presentation, and diagnosis of vascular graft infections, with a focus on surgical treatment of infected aortic, peripheral bypass, and dialysis access grafts.
Pathogenesis
Pathogenic mechanisms of graft infections include contamination and direct seeding of the graft during implantation, extension from a contiguous infected site, or hematogenous seeding from a remote site. Host-related factors known to increase graft infection risk include comorbidities such as diabetes mellitus, obesity, renal failure, liver disease, malnutrition, and the use of immunosuppressive medications. 2 Bloodstream infections present at the time of graft implantation also increase the risk of graft infection. Procedure-related risk factors include breaks in sterile technique, grafts placed in the groin, grafts tunneled subcutaneously, prolonged operative time, emergency surgery, reoperative surgery, prolonged preoperative hospitalization, and lack of appropriate perioperative antibiotic prophylaxis. 3 In addition, postoperative wound complications such as infections or lymphoceles increase the risk of developing a vascular graft infection.
Overall, Staphylococcus aureus and Staphylococcus epidermidis are the most common causative pathogens in vascular graft infections. 4 Although less common, graft infections due to gram-negative bacteria have increased in frequency. 5 The relative frequency of pathogens responsible for graft infections also varies by surgical site. In thoracic aortic and carotid operations, S. aureus is clearly the most common microbe implicated in graft infections. 6 In aortofemoral operations, S. aureus, S. epidermidis, and gram-negative bacteria all contribute roughly similar proportions. 6 In lower-extremity peripheral bypasses, S. aureus and gram-negative bacteria are most commonly identified as the causative agents, and they comprise a comparable proportion of cases. 6 As expected, gram-negative bacteria are responsible for nearly half of graft infections caused by graft-enteric erosion or fistula, with the remaining microbes comprising significantly lower proportions.
Methicillin-resistant Staphylococcus aureus, or MRSA, is causing an increasing percentage of vascular graft infections. 7 MRSA graft infections usually occur in hospitalized patients, with some reports demonstrating higher morbidity and mortality as compared to other pathogens due to antibiotic resistance and multiple virulence factors. Fungal graft infections can occur, but are much less common and typically limited to immunosuppressed patients. Pseudomonal graft infections are also uncommon, but are virulent and associated with anastomotic disruption and bleeding complications. 8 In general, infections occurring early after graft implantation are due to more virulent organisms such as S. aureus or gram-negative bacteria, whereas late infections are due to less virulent pathogens such as S. epidermidis. 9
Clinical presentation and diagnosis
Symptoms and signs of vascular graft infection can vary by the time elapsed from implantation and by the surgical site. Graft infections occurring early after implantation (within 4 months) typically show systemic signs of infection including fever, malaise and leukocytosis. 9 Bacteremia and wound infection may also be present. In aortic grafts, early infections can present with abdominal pain, abdominal distension, bleeding from anastomotic disruption, sepsis and/or ileus. Graft infections involving the groin or extremities can manifest with overlying erythema, induration, palpable fluid collection, purulence, and/or a pseudoaneurysm.
Vascular graft infections occurring late after implantation are generally more subtle with non-specific signs and symptoms. 9 Fever, leukocytosis and bacteremia may be absent. Graft thrombosis, anastomotic hemorrhage, pseudoaneurysm, graft-enteric erosion, graft-enteric fistula, and chronic draining sinuses are complications that may occur as a result of late graft infections.
The diagnosis of vascular graft infections first relies upon a thorough history and physical examination. Specific operative details should be obtained and particular attention paid to the risk factors for graft infections highlighted above. Surgical incision sites should be examined for classic signs of infection including erythema, induration, and purulent drainage. Perigraft fluid collections and anastomotic pseudoaneurysms may also be palpable. Symptoms and signs of infection at remote sites should also be evaluated, as seeding of pathogens through the bloodstream is a mechanism of graft infection. Signs of septic embolization may be evident on physical examination as well.
Basic laboratory studies are often non-specific in vascular graft infections. Findings include leukocytosis with a left shift and an elevated erythrocyte sedimentation rate. Cultures should be obtained from wounds or perigraft fluid in patients in whom infection is suspected, for both diagnostic purposes and to guide antimicrobial therapy. It is important to note that negative cultures do not reliably exclude graft infection, as bacteria can be slow growing. Cultures from remote sites including the bloodstream should also be obtained.
Imaging modalities include ultrasonography, computed tomography, magnetic resonance imaging, and radionuclide-labeled leukocyte scanning. The gold standard for graft infection diagnosis is computed tomography, particularly for intracavitary grafts and extracavitary grafts involving the neck, torso, or proximal limbs. 10 Findings suggestive of prosthetic graft infection on computed tomography include perigraft fluid or gas, perigraft stranding with loss of tissue planes, focal bowel wall thickening, and pseudoaneurysm (Figure 1). The presence of air or fluid surrounding the graft is normal in the immediate (days to weeks) postsurgical setting, and can complicate interpretation of the scan if an early graft infection is suspected. In later graft infections occurring at least a few months after implantation, perigraft fluid or air is more specific for infection as postsurgical changes detectable on computed tomography usually subside by that time. Computed tomography is also advantageous in that it allows for evaluation of the extent of infection, and can accordingly be useful for operative planning.
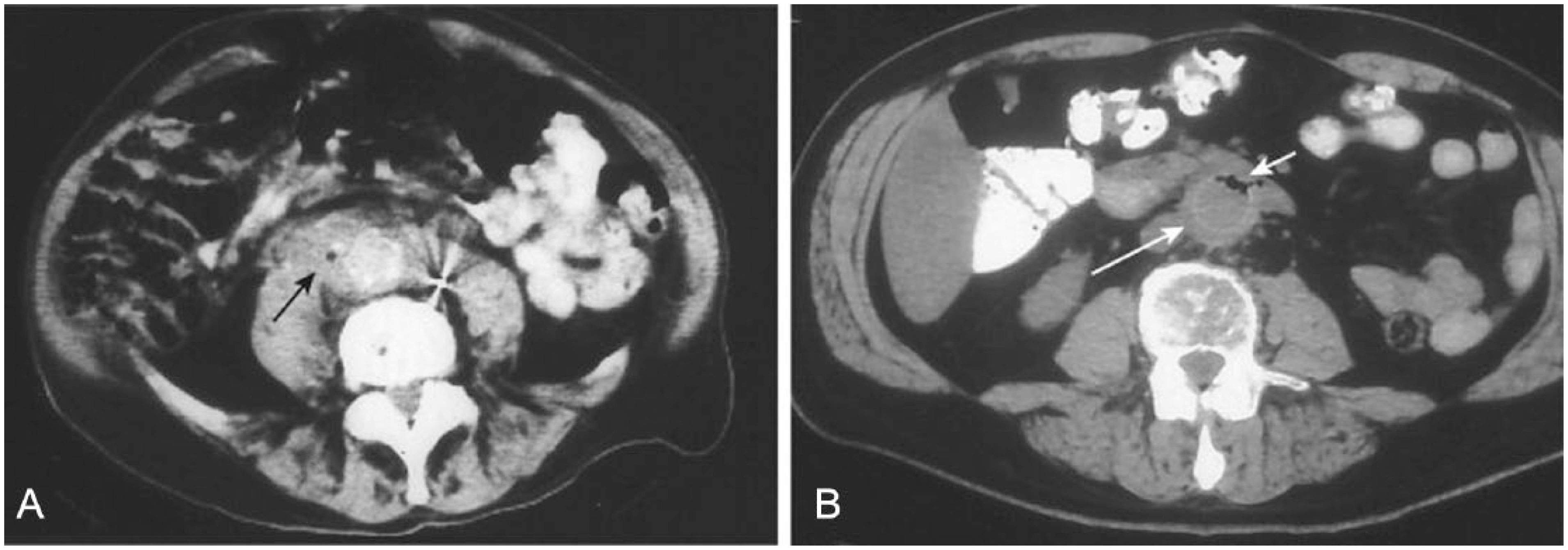
Computed tomography scans demonstrating (A) perigraft fluid and air (black arrow) and (B) thickened graft tissue (long white arrow) with graft and perigraft air (short white arrow). Reprinted from Reilly LM, Prosthetic vascular graft infection. In: Hallett JW, Mills JL, Earnshaw JJ, et al. (eds) Comprehensive Vascular and Endovascular Surgery, second edition, Elsevier, 2009, with permission.
Ultrasonography is non-invasive, can be performed at the bedside, and is particularly useful for evaluating extracavitary grafts. 11 Perigraft fluid collections or abscesses can be visualized on ultrasound and ultrasound-guided aspiration can be performed as well if desired. Duplex scanning is reliable in differentiating perigraft fluid from hematoma or pseudoaneurysms. It is also highly accurate in identifying graft thrombosis or stenosis.
Magnetic resonance imaging provides similar anatomic detail as computed tomography and is able to better distinguish perigraft fluid from inflammation and fibrosis. 12 However, it is more expensive, less tolerable to patients, and gadolinium has an uncommon but serious side effect of systemic fibrosis in patients with renal insufficiency. Radionuclide labeling of leukocytes is different from the aforementioned modalities in that it is a functional and not anatomical evaluation tool. Radionuclide scans can detect perigraft leukocyte accumulation, suggesting infection, with a sensitivity of 100% in most series although this finding is non-specific in the early postimplant period given that inflamed, healing tissues contain white blood cells.12,13 In cases where graft-enteric erosion or fistula is clinically suspected, endoscopy is essential for diagnostic evaluation (Figure 2). 14
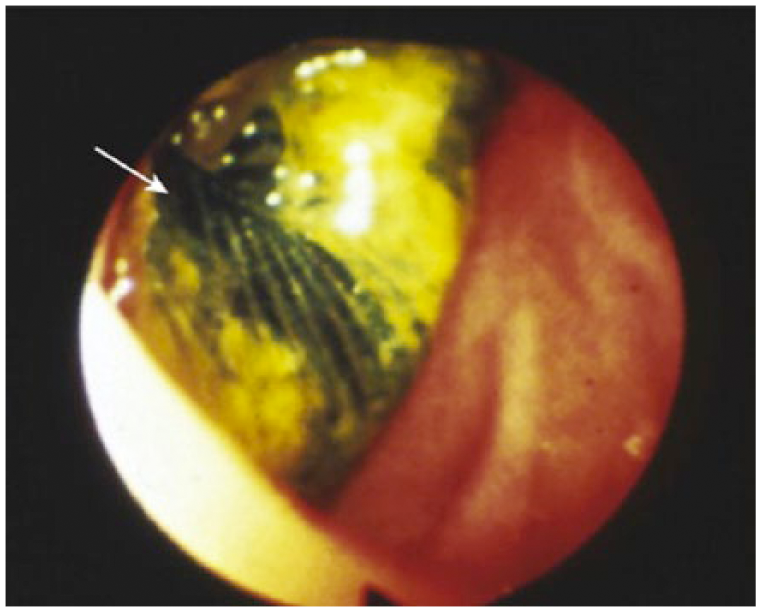
Endoscopy demonstrating a vascular graft (white arrow) visible from the duodenal lumen. Reprinted from Reilly LM, Prosthetic vascular graft infection. In: Hallett JW, Mills JL, Earnshaw JJ, et al. (eds) Comprehensive Vascular and Endovascular Surgery, second edition, Elsevier, 2009, with permission.
General approach to treatment
The basis of treating infected vascular grafts relies upon how sure the clinician is regarding the diagnosis and the severity of illness of the patient. The clinical presentation can be insidious or subtle in some cases. As mentioned previously, diagnosis can also be unclear as perigraft fluid is normal in the immediate postoperative period. In these cases in the ‘gray zone’, the decision to initiate antibiotic therapy should rely upon the clinical condition of the patient. Those who are symptomatic, with abnormal physical exam findings, or with leukocytosis or fever should be treated at the least with antibiotics and potentially with surgery.
In general, early aggressive surgical treatment is the gold standard (Figure 3). In other words, in cases where the diagnosis is clear, antibiotic therapy alone is infrequently successful and early aggressive surgical debridement with or without revascularization is necessary for any chance of cure. There are specific instances where the decision is very clear and indicative of aggressive surgical therapy – sepsis, anastomotic disruption, aortoenteric fistula, and involvement of particularly virulent organisms such as pseudomonas or MRSA. If none of these conditions are met, consideration can be given to partial graft excision or debridement of infected tissue. There should be a low threshold for total graft excision if there is any indication that the patient is deteriorating clinically after graft preservation approaches have been attempted. Vascularized flaps or negative-pressure wound therapy can be utilized as adjuncts as well.
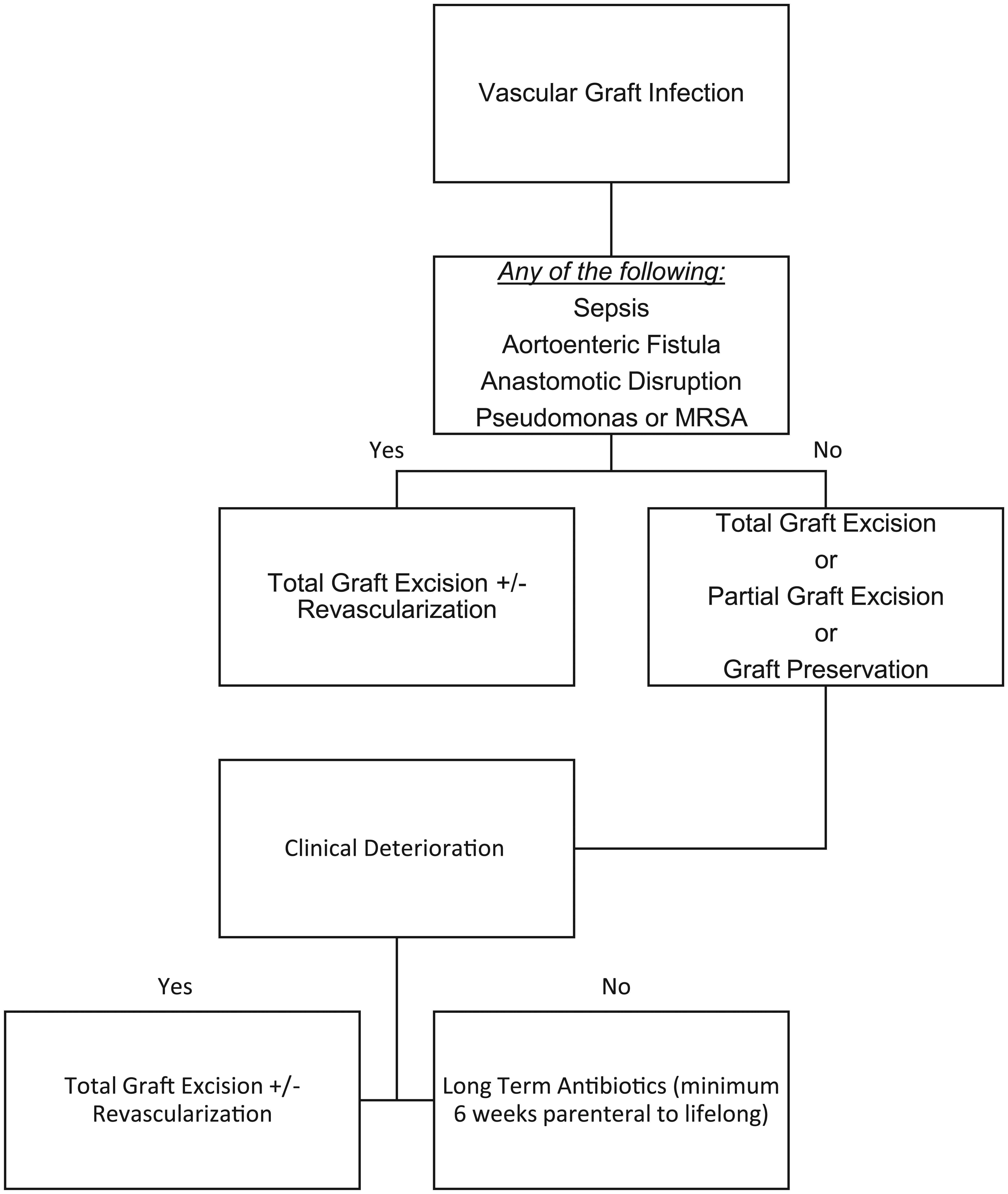
Algorithm for the general approach to managing infected vascular grafts.
In some cases, total graft excision is associated with very high surgical risk due to the patient’s comorbidity burden or the extent of the surgery required, or both. These clinical scenarios are a double-edged sword because although the patient may have high baseline risk, their ability to tolerate a severe infection that will likely not improve without surgical treatment is also limited. Not surprisingly, therefore, these cases where there is graft infection in the setting of substantial baseline patient risk are associated with even greater mortality and morbidity.
There are no randomized data to dictate how long antimicrobial therapy should be continued after source control, although most would agree that at least 4–6 weeks of parenteral antibiotics are necessary. Some of these patients are placed on lifelong antibiotics, particularly if subtotal or partial graft excision or other graft preservation strategies are employed. Typically, broad spectrum parenteral antibiotics such as vancomycin and piperacillin/tazobactam are initiated, and antibiotics are tailored after culture data have resulted. Virulent organisms such as pseudomonas and MRSA should be covered until cultures are finalized. Antibiotic management can be further complicated if culture data are negative. If clinical suspicion was equivocal, then some would advocate for a shorter course of antibiotics or discontinuation of antibiotics with monitoring of clinical status. If clinical suspicion remains, particularly in the setting of graft preservation, then broad spectrum antibiotics are typically continued for at least 4 weeks.
Surgical options for the management of infected aortic grafts
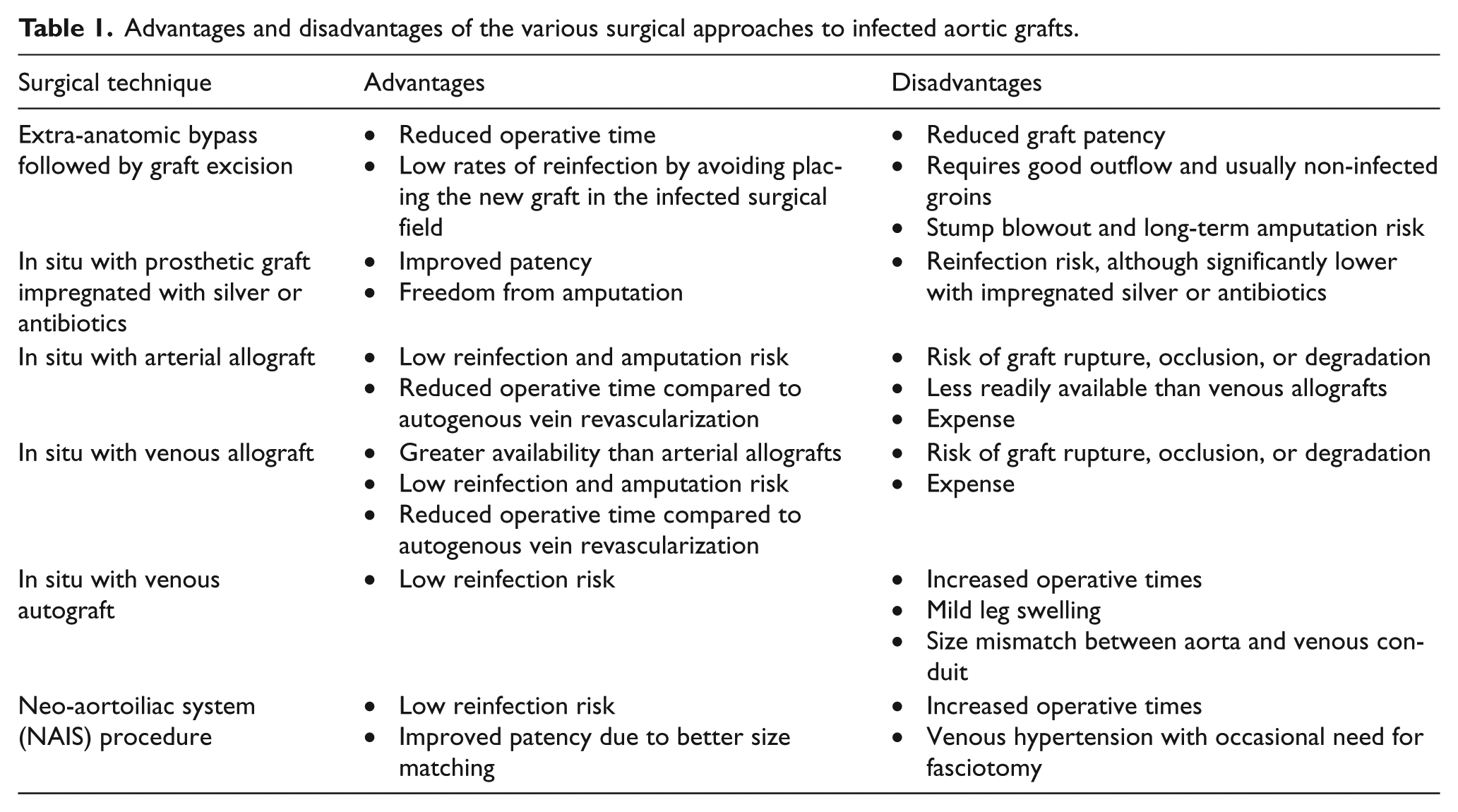
There are several surgical options for treating infected aortic grafts (Table 1). An extra-anatomic, or ex situ, bypass can be performed through non-infected tissue planes, followed by removal of the infected graft with debridement of infected tissue. This sequence is preferred in order to avoid prolonged tissue ischemia if the graft removal were performed prior to revascularization. The operation can be staged with a 1 to 5-day interval to avoid a prolonged operative time. The typical extra-anatomic bypass is an axillobifemoral bypass using ringed polytetrafluoroethylene. A prosthetic femoral-femoral bypass can be performed if the groins are free of infection, otherwise autogenous vein, or venous or arterial allografts should be utilized to minimize reinfection risk. Good outflow is essential to maintaining patency of these grafts, which can often be difficult due to the multilevel disease that is frequently present in these patients.
Advantages and disadvantages of the various surgical approaches to infected aortic grafts.
Other surgical options include excision of the infected graft with immediate in situ reconstruction. Aggressive debridement and removal of infected tissue is performed. Reconstruction options for the in situ approach include in-line placement of a prosthetic graft or tissue graft, with the latter encompassing arterial allografts, venous allografts, and venous autografts.
For prosthetic grafts, polytetrafluoroethylene or polyester conduits can be utilized. To lower the risk of reinfection, which remains a primary concern with this technique, grafts impregnated with silver or antibiotics such as rifampin have been used. The new prosthesis is wrapped in omentum, and muscle flap coverage at the groin sites can also be performed if they are involved. Parenteral antibiotics are administered for at least 6 weeks post-operatively with some groups recommending lifelong oral antibiotics. 15
There are several operative principles to keep mindful of when using cryopreserved arterial allografts. These grafts should be thawed immediately before implantation. As with other conduits, creating a tension-free anastomosis is important. When sizing the arterial allograft, it is important to remember that these have less tensile strength than prosthetic grafts. 16 Side branches of the arterial allograft should be sutured, with avoidance of metal clips or ties. Reinforcement of the anastomosis with pieces of allograft can also be performed. Similar to in situ prosthetic reconstruction, wide debridement of infected tissue with postoperative parenteral antibiotics for at least 6 weeks is recommended.
Cryopreserved vein allografts have also been used in an effort to improve patency rates as compared to axillofemoral bypass, and to reduce operative time by eliminating the need for autogenous vein harvest. Similar to arterial allografts, vein allografts reduce the risk of recurrent infection. Another advantage of venous allografts is that they are more readily available than arterial allografts.
Ultrasonography should be used for preoperative assessment in cases where autogenous vein is selected for reconstruction. Most commonly, the great saphenous vein or femoral vein is used. The vein should be greater than 6 mm in diameter, as smaller veins increase the risk of reduced patency due to size mismatching. Techniques to address size discrepancy include plication of the anterior aorta and joining of both vein grafts together to form a larger graft. In addition to flow limitations from size mismatch, autografts are more prone to kinking or external compression relative to prosthetic grafts. Similar to peripheral bypasses, the saphenous vein can be reversed or the valves can be eliminated with a valvulotome.
The neo-aortoiliac system, or NAIS, procedure utilizes femoropopliteal veins for vascular reconstruction. 17
Outcomes of interest include mortality, amputation rates, stump blowout, recurrent infection, graft occlusion or stenosis, pseudoaneurysm, and bleeding. With extra-anatomic bypass and graft excision, the 30-day mortality rates have improved over time, in general ranging from 5% to 25%.4,18–21 Late mortality has been 20% and 45% in most series.18,20,21 Limited graft patency has been the principal disadvantage with this technique. Primary patency rates at 1 year have ranged from 60% to 90% and at 5 years from 40% to 75%.22,23 Low rates of reinfection by avoiding placement of the new graft in the infected surgical field is a principal advantage of this technique. The reinfection rates for extra-anatomic bypass have ranged from 0% to 15% in prior series.22,24 Stump blowout is also an infrequent but devastating complication.22,24 Finally, the rates of lower extremity amputation have typically ranged from 0% to 15% in recent literature.21–23
The 30-day mortality rates for in situ reconstruction with antibiotic-impregnated prosthetic grafts have ranged from 0% to 20%, with more recent series being in the 5–10% range.21,25 Reinfection rates range from 5% to 20%.21,25 Amputation rates of 0–5% have been reported in multiple series with this approach.21,25
For revascularizations involving autogenous vein, 30-day mortality rates have ranged from 5% to 10%.26,27 Reinfection rates, as expected, are low at 0–5%, with graft thrombosis in 0–5% and amputation rates of 0–10%.26,27 Primary 5-year patency of over 90% has been reported. 27 The operative times for this approach are significant and have averaged 6 to 9 hours, with significant reductions when using multiple teams. Mild leg swelling can also commonly occur with this approach, although the rates of chronic venous insufficiency have been very low.
In the NAIS procedure, the 30-day mortality is approximately 10%.17,28 The 5-year primary patency rates have ranged from 75% to 90%. 29 Amputation rates at 30 days have ranged from 2% to 7%. 29 Similar to other non-prosthetic cases, the rates of reinfection are low at less than 2%. 29 Venous insufficiency and hypertension can occur with fasciotomy rates in the 10–15% range. 29
With cryopreserved allografts, 30-day mortality is 5–15% and primary patency at 3 years is 80–100%.30–32 Graft rupture generally occurs in less than 10%, reinfection in 0–6% and amputation in 0–5%.30–32 Graft occlusion or aneurysmal degradation each occurs in less than 10% of patients.30–32
Surgical options for the management of infected endovascular aortic grafts
Endovascular approaches to aortic disease have been utilized at exponentially higher rates in recent years. Although the data are limited, endovascular graft infection occurs at a much lower rate than with open aortic grafts. The reported rates have generally been less than 1.2%.33,34 Risk factors for developing endovascular aortic graft infection include hematogenous seeding from other infected sites, endoleak, multiple endovascular procedures, and increased length of the stent-graft. A subset of infected endovascular grafts present as graft-enteric erosion or fistula.
The operative principles of managing infected endovascular aortic grafts parallel those of open aortic grafts. Excision of the stent-graft with wide debridement of infected tissue is often performed. Revascularization options include those highlighted previously. Particular attention should be paid to the type of device that was used and the specific anatomy, including extent of the stent-graft. Suprarenal fixation of the stent-graft necessitates suprarenal or supraceliac proximal control. 35 Some reports have demonstrated successful treatment without graft excision in high-risk patients without graft-enteric fistulae or erosions who responded to a minimum 6-week course of intravenous antibiotics. Endovascular repair of graft-enteric fistulae or infected pseudoaneurysms have also been reported with low procedural morbidity, but these usually represent a bridge to definitive repair. 36
Data regarding outcomes of the rare aortic stent-graft infection are limited. The operative mortality risk with stent-graft excision and revascularization is significant and ranges from 20% to 30%. 33 With the non-operative approach consisting of parenteral antibiotics and abscess drainage, the mortality rates are also high, ranging from 35% to 45%, underscoring the importance of operative treatment in the vast majority of cases. 37
Surgical options for the management of infected peripheral bypass grafts
In contradistinction to infected aortic grafts, infected peripheral bypass grafts pose greater risk to loss of limb as opposed to loss of life, although sepsis and bleeding complications can occur and have devastating outcomes. Graft preservation techniques are used more frequently with infected peripheral bypass grafts than with aortic grafts. Graft removal is generally indicated, however, when the graft is occluded, when there is anastomotic disruption, or when signs or symptoms of sepsis develop. Partial graft excision limited to infected portions of the graft can also be performed.
An important concept is the timing of the graft infection. Infections occurring early after bypass typically occur in the setting of a postoperative wound infection. In these cases, graft preservation with aggressive wound debridement and muscle flap coverage is an appropriate option if the patient is not clinically septic and there is no hemorrhage. The graft preservation technique can be performed in a staged manner, with the initial operation consisting of wound debridement and a second operation 2 days later consisting of further debridement as necessary and coverage with a well-vascularized muscle flap. Parenteral followed by oral antibiotics are usually continued for up to 6 months, with antibiotic choice being guided by cultures obtained intraoperatively.
In peripheral graft infections occurring late after initial bypass, graft salvage is typically not possible. In these scenarios, preoperative ultrasound assessment of potential vein conduits is important. Graft removal with infected tissue debridement and revascularization with autogenous vein is performed. Revascularization can be performed first through uninfected tissue planes using fresh anastomotic sites prior to graft excision. As this is not always possible, sewing the new autogenous vein to the areas where the infected graft was removed is also reasonable if the proximal and distal anastomotic sites are of appropriate tissue quality.
Multiple studies in the literature have reported on outcomes of managing infected peripheral bypass grafts.38–40 Operative mortality rates have ranged from 0% to 18%. Major amputation has occurred in 0–25%, with the higher rates occurring in patients who were not revascularized. Because revascularization is typically performed with autogenous vein, rates of reinfection are low at 0–10%. This comes at the expense of a higher rate of conduit failure, occurring in upwards of 35% of patients.
Surgical options for the management of infected dialysis access grafts
Infection of prosthetic dialysis access grafts is a frequent complication and a source of major morbidity in this patient population. These patients tend to have comorbidities associated with increased infection risk at baseline, and repeated cannulation of the graft exposes it to bacterial contamination. When hemodialysis graft infection occurs, the traditional surgical treatment has been complete graft excision, infected tissue debridement, and placement of temporary hemodialysis access. The wounds are typically left open with wet-to-dry dressing changes performed twice daily.
Some groups have described subtotal excision of the graft, leaving a small cuff of prosthetic on the artery if it is well incorporated to reduce nerve injury and hemorrhage. 41 This technique can be employed if there is no overt sepsis. Partial graft excision can also be performed if there is no overt sepsis or bleeding. 41 If this technique is to be used, preoperative duplex evaluation should be suggestive of only partial infection of the graft with no perigraft fluid around the remaining portions of the prosthesis. It is also important that the non-infected areas of the graft be well incorporated. The advantage of the partial excision approach is that portions of the graft are available for dialysis and that placement of temporary access is not required. These benefits may be especially relevant in patients with limited access options.
Some studies have demonstrated higher complication and local infection rates with partial graft excision compared to total graft excision, although rates of hemorrhage and graft-associated sepsis appear similar. 42 A large series demonstrated successful outcome in all patients treated with total graft excision or subtotal graft excision, with uniform healing of the wounds by secondary intention. 41 With partial graft excision, 74% achieved graft patency and wound healing, although again, the benefits were that a temporary dialysis catheter was not required and the site could be used for continued dialysis. The failed partial graft excisions underwent total graft excision due to non-healing wounds. There were no hemorrhagic or septic events with this technique.
Conclusions
Vascular grafts are invaluable tools in the armamentarium of the vascular surgeon. However, as with other foreign bodies, they pose a risk of infection to the patient. The management of infected vascular grafts and the impact of this complication on patient outcomes vary with the surgical site, although the clinical sequelae can be catastrophic. In general, treatment entails broad spectrum antibiotics and wide debridement of infected tissues, including removal of the graft (Table 2). Revascularization can be achieved by in situ replacement of the infected graft or placement of a new graft through non-infected tissue planes. Graft-preserving techniques have also been described and have been met with success in select cases.
Key concepts in the diagnosis and management of infected vascular grafts.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.