
Abstract

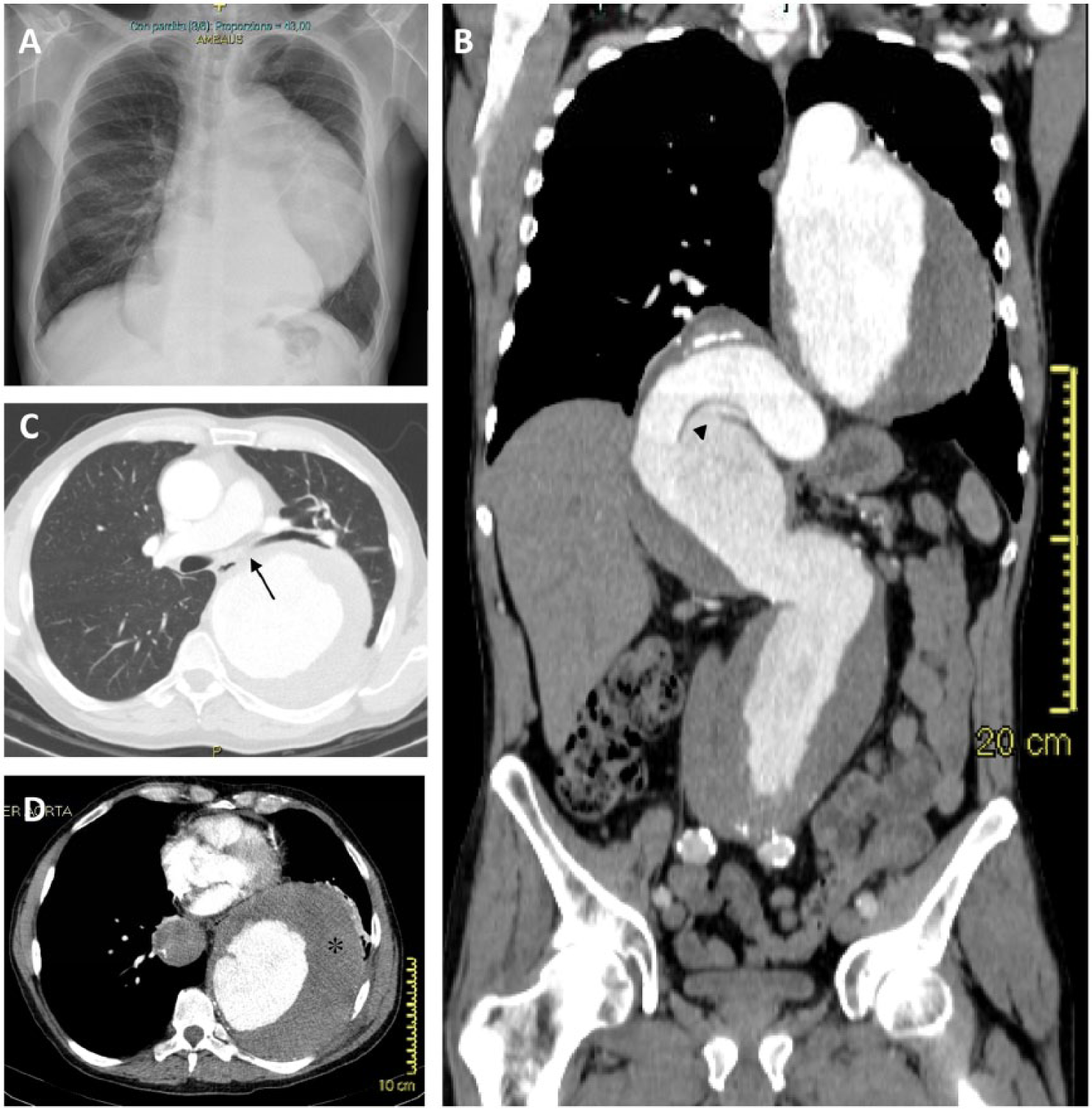
A 65-year-old man with a history of arterial hypertension presented with a persistent cough for 3 months. He was a former smoker who had quit 15 years ago; there was no family history of aneurysm or connective tissue disease. Physical examination revealed decreased breath sounds and dullness at the left middle-lower lung. A chest X-ray showed a large mediastinal mass consistent with a markedly enlarged aortic profile, without inflammatory alterations of the lung parenchyma (Panel A). Thoraco-abdominal contrast-enhanced computed tomography revealed a large aneurysm of the aorta extending from the isthmus to the aorto-iliac bifurcation, configuring a thoraco-abdominal aneurysm (TAA) with type II extension according to the modified Crawford classification (Panel B); the left main bronchus and its inferior branch were compressed and dislocated by the aneurysm (Panel C, arrow); the maximum axial diameter of the descending thoracic aorta was 15 × 13 cm with an eccentric parietal thrombus (Panel D, asterisk); at the thoraco-abdominal transition, the artery angled with evidence of parietal dissection (Panel B, arrowhead), and the maximum size of the aneurysm at the abdominal tract was 9.5 × 8.6 cm below the renal arteries.
After vascular surgery consultation, the patient underwent urgent repair with hybrid technique. The postoperative course was complicated by lower extremity paraparesis due to spinal cord ischemia, acute kidney injury and polymicrobial sepsis. There was no evidence of progressive enlargement of the aneurysmal sac after the 3-month follow-up but the neurological sequelae have not improved despite an intensive rehabilitation program.
TAAs are usually asymptomatic and often identified incidentally on imaging studies for other purposes. The presence of symptoms depends on the location and the size of the aneurysm and includes local mass effect symptoms such as dysphagia, hemoptysis, dyspnea, hoarseness, and recurrent pneumonitis. 1 Here we reported for the first time a case of giant dissecting TAA presenting as a chronic cough due to progressive compression of the left main bronchus.
Only a few cases of TAA with a maximum diameter > 10 cm have been reported, and the absolute risk of rupture and the optimal indications for treatment in these cases are still uncertain. 2 Recent endovascular innovations have led to alternative approaches for TAA correction. 3 Despite major progress in the knowledge of pathophysiology and operative strategies, further improvements in end-organ protective strategies are needed to decrease the incidence of potentially devastating postoperative ischemic complications.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.