
Abstract

Keywords
What is thoracic outlet syndrome?
Thoracic outlet syndrome (TOS) is an uncommon condition that can happen when the nerves, artery, or vein to the arm is compressed by one or more structures that make up the thoracic outlet (Figure 1).
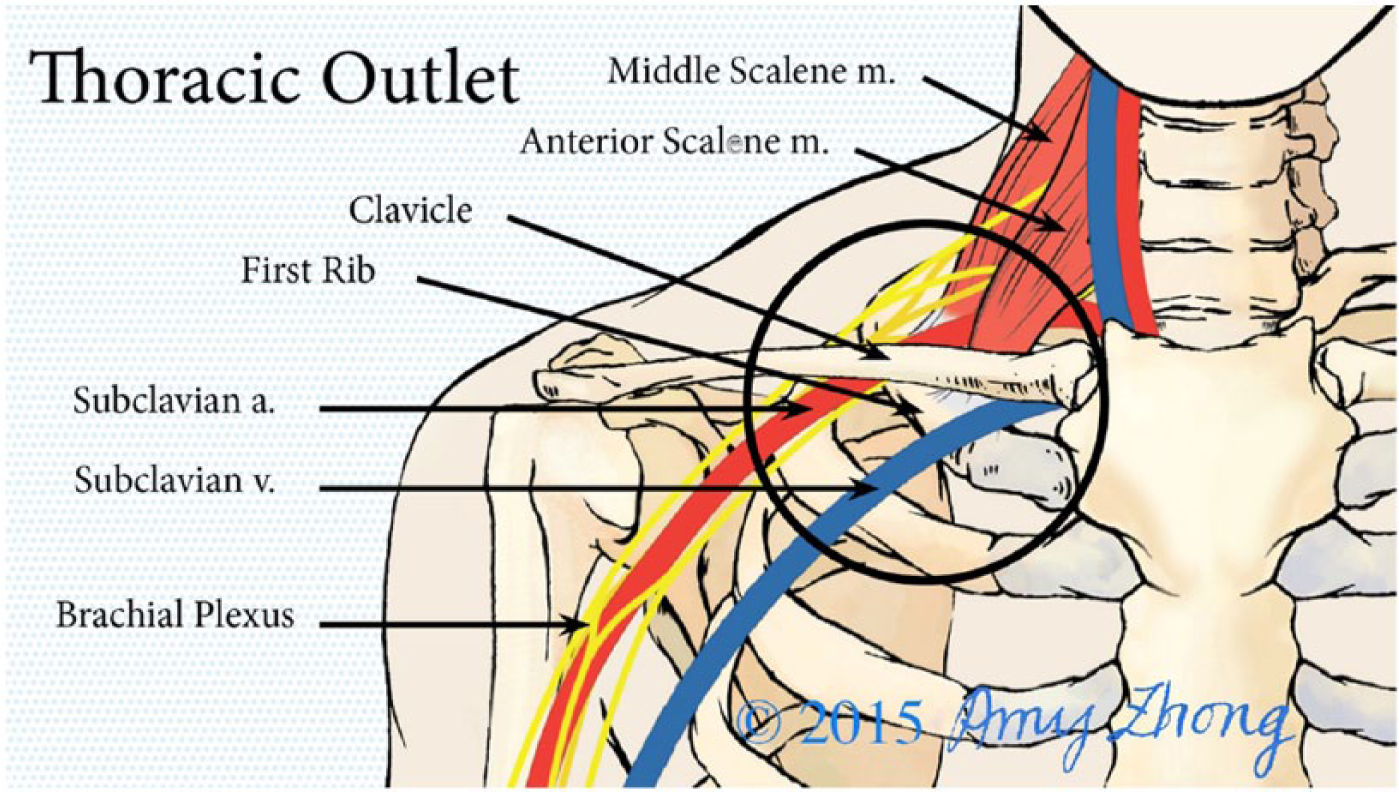
Diagram of the anatomy of the thoracic outlet showing the subclavian artery, vein, and brachial plexus (nerve bundle) passing through the anterior scalene muscle, which attaches to the first rib. (Illustration printed with permission. © Amy Zhong.)
Typically, TOS involves the first rib and anterior scalene muscle but can also be caused by a ‘cervical rib’. A cervical rib is an extra rib that connects to the cervical spine at the base of the neck. This extra rib may fuse with the first rib, which can then cause compression, particularly on the nerves and subclavian artery. The subclavius muscle, which attaches to the front of the first rib, can also compress the subclavian vein.
A past history of trauma or injury can also contribute to the development of thoracic outlet syndrome. The healing process of a collarbone fracture results in extra bone formation, which may cause compression of the nerves or blood vessels. Whiplash or other motor vehicle accident injuries can lead to spasms of the anterior scalene muscle, causing narrowing of the thoracic outlet.
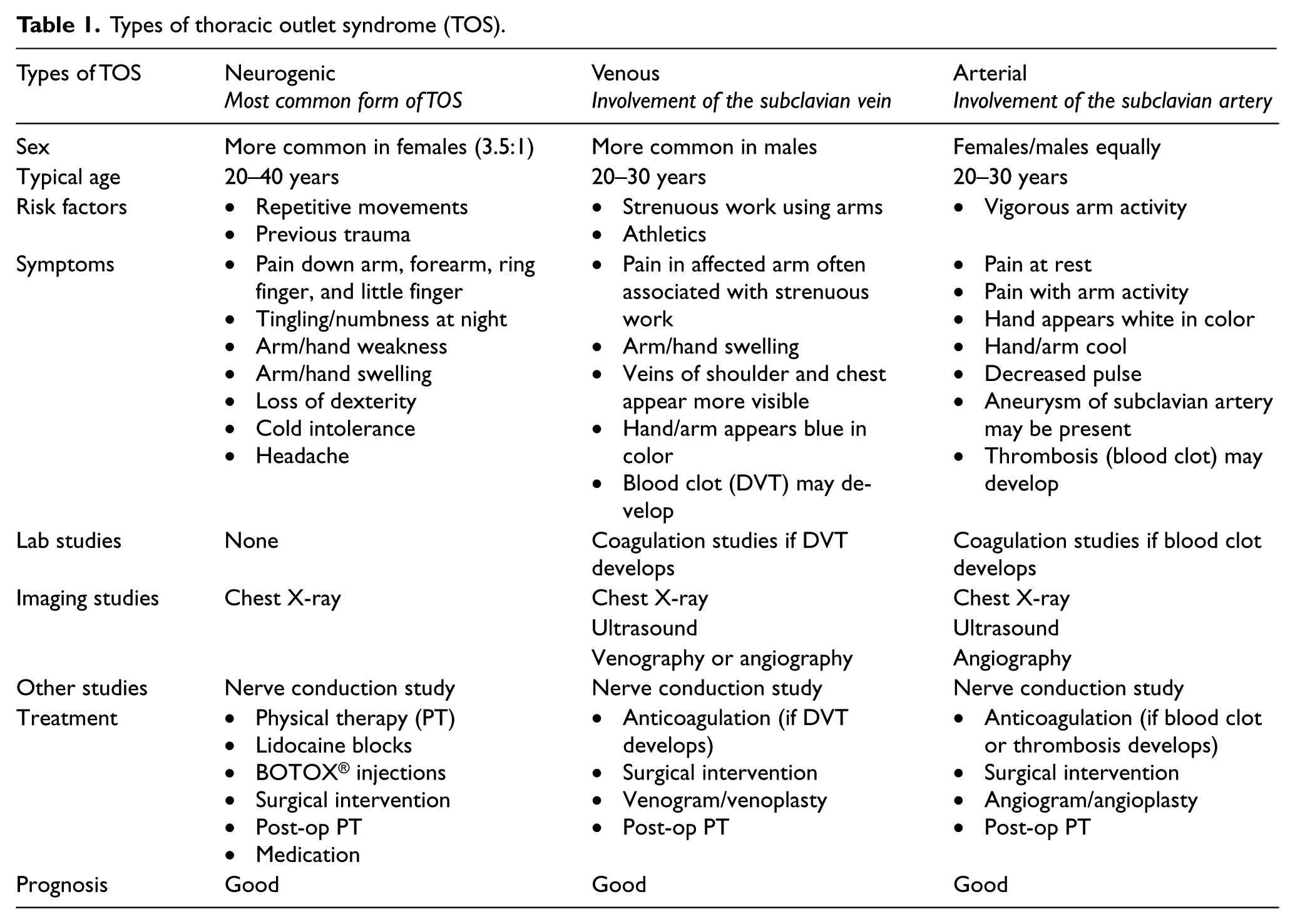
There are three different types of thoracic outlet syndrome, as shown in Table 1. The diagnosis is based on which structure is compressed, and it is occasionally possible to have more than one type. ‘Neurogenic’ (involving the nerves) is the most common type of thoracic outlet syndrome and the most difficult to diagnose. It occurs as a result of compression of the brachial plexus at the level of the thoracic outlet. The brachial plexus is the network of nerves that arise from the spinal cord and travel to the arm.
Types of thoracic outlet syndrome (TOS).
Venous thoracic outlet syndrome can occur due to compression of the subclavian and axillary vein over time. With compression, scar tissue can form inside of the vein, which can create a web-like matrix that eventually decreases the blood flow in the vein. This reduction in flow can cause a blood clot to form in the vein, a condition called deep vein thrombosis or DVT. This may be seen in a condition called Paget–Schroetter syndrome, or effort thrombosis, when repetitive shoulder and arm muscle use leads to DVT in the arm veins.
Arterial TOS occurs when the subclavian artery is compressed, which often happens when a cervical rib is involved. Arterial TOS can cause dilation of the arteries, known as aneurysms, which can predispose to blood clots that need to be addressed urgently.
Patients with a history of trauma or injury to any structures in or around the thoracic outlet are at increased risk for TOS. Patients who have occupations requiring chronic repetitive motion can also be at increased risk. High-level athletes who compete in swimming, rowing, baseball (especially pitchers), weightlifting, or any other sport that involves the muscles around the neck and shoulder are also at risk, particularly for venous TOS.
What are the signs and symptoms of thoracic outlet syndrome?
Symptoms of neurogenic TOS include numbness and tingling down the arm. Symptoms often worsen with activities that involve overhead reaching, such as taking an item off a high shelf, or extending the arms, such as typing. Color or temperature changes can occur in the arm, but swelling is uncommon.
In venous TOS, swelling is typically the first symptom. It can be preceded by a few days of soreness or a ‘tourniquet-like’ feeling in the arm. The veins across the chest and arm may become prominent, especially with physical activity. The symptoms may be severe and can come on suddenly, which often leads patients to the emergency room. A blood clot (DVT) in the subclavian vein is typically diagnosed.
Arterial TOS can cause coolness, achiness, and soreness of the arm without swelling. These symptoms are worse with overhead activity and can cause the palms to look pale due to decreased blood flow. There may be a prominent pulse in the area over the collarbone if an aneurysm (dilated artery) is present. When clots in the subclavian artery travel down the arm, other blood vessels in the arm or hand can become blocked, requiring immediate surgical attention. Table 1 shows which patients are at risk for developing the different types of TOS. Some symptoms can overlap, and patients can occasionally have more than one type, so further evaluation with a careful physical examination and ultrasound tests may be necessary.
How is thoracic outlet syndrome diagnosed?
Thoracic outlet syndrome is diagnosed through a combination of patient history, physical examination findings, and imaging studies. Since TOS is rare, the diagnosis can be easily missed, and it is common for patients to have seen multiple specialists without a clear diagnosis or understanding of the cause of their symptoms. A physical therapist or even the patient might be the first to suspect the diagnosis.
Depending on the type of TOS that is suspected, patients are evaluated with a variety of physical examination tests that help to confirm the diagnosis. Common tests for neurogenic TOS include the Adson’s maneuver, the elevated arm stress test (EAST), and the upper extremity tension test (also known as Elvey’s test). In the Adson’s maneuver, the radial pulse at the wrist is felt while the arm is raised away from the body. This test alone does not confirm a diagnosis of TOS, since some people with no symptoms can have a decrease or disappearance of the pulse at the wrist with moving the arm away from the body. The elevated arm stress test (EAST) is also performed with the arms elevated to provoke symptoms. The upper extremity tension test (Elvey’s test) checks for pinching of the nerve at the thoracic outlet. Peripheral nerves are tested along with range of motion in the arm.
Frequently, patients with TOS symptoms may have had many diagnostic tests including magnetic resonance imaging (MRI) studies, computed tomography (CT or CAT) scans, nerve conduction studies (NCS), electromyography (EMG), or ultrasounds. Imaging can help with the diagnosis of venous or arterial TOS, but patients with neurogenic TOS may have normal tests. Nevertheless, these tests may be necessary to look for other more common diagnoses.
For venous or arterial TOS, common tests used for diagnosis include CT or Doppler ultrasound studies. Occasionally, a venogram may be performed to diagnose and treat TOS. A venogram is a procedure in which a small tube is inserted into the vein, and dye is injected into it to show the veins under real-time X-ray imaging. Thrombolysis may be needed, which is a procedure that dissolves blood clots. Angiography (which is similar to venography except that the dye is used to see the arteries instead of the veins) may be useful in arterial TOS.
How is thoracic outlet syndrome treated?
The treatment depends on the type of TOS. Neurogenic TOS is often initially treated with thoracic outlet-specific physical therapy. Many patients are able to get relief without the need for surgical intervention. If symptoms do not improve with physical therapy alone, in some cases botulinum toxin A (BOTOX®) injections into the anterior and middle scalene muscles can be tried in conjunction with physical therapy. Surgical decompression procedures are an option if less invasive treatments are not successful.
The treatment of venous TOS depends on how long the condition has been present. Patients who have the sudden onset of venous TOS and have arm DVT are frequently treated first with thrombolysis (clot-busting medications) to dissolve the thrombosis, along with blood-thinning medications. Treatment is then continued with a surgical decompression procedure to relieve the compression on the vein that caused the arm DVT to form. Blood flow in the vein frequently can be improved by inflating a small balloon inside the vein and inserting a stent to prop the vein open. Open surgical venous reconstruction is rarely necessary.
Patients with arterial TOS often require surgical decompression procedures to remove the rib and/or scalene muscles, including reconstruction procedures for the damaged artery, which may be aneurysmal (dilated) or contain a blood clot.
Physical therapy remains an integral part of recovery after any surgical intervention. Patients may also have to remain on blood thinners for a period of time after surgery.
Conclusion
Thoracic outlet syndrome is a rare disorder that can be challenging to diagnose accurately. The treatment plan depends on the type of TOS (neurogenic, venous, or arterial) and should be tailored to best address the patient’s symptoms and expectations.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.