
Abstract
Socioeconomic status (SES) as reflected by residential zip code may adversely influence outcomes for patients with acute pulmonary embolism (PE). We sought to analyze the impact of neighborhood SES on in-hospital mortality, use of thrombolysis, implantation of inferior vena cava (IVC) filters and cost of hospitalization following acute PE. We used the 2003–2011 Nationwide Inpatient Sample (NIS) for this analysis. All hospital admissions with a principal diagnosis of acute PE were identified using ICD-9 codes. Neighborhood SES was assessed using median household income of the residential zip code for each patient. Over this 9-year period, 276,484 discharges with acute PE were analyzed. There was a progressive decrease in in-hospital mortality across the SES quartiles (p-trend <0.001). The incidence of in-hospital mortality across quartiles 1–4 was 3.8%, 3.3%, 3.2%, and 3.1%, respectively. Despite low rates of thrombolytic utilization in this cohort, we observed a progressive increase in the rate of thrombolysis utilization across the SES quartiles (1.5%, 1.6%, 1.7%, 2.0%; p-trend <0.001). There was no significant difference in the use of IVC filters across the SES quartiles (p-trend=0.9). The mean adjusted cost of hospitalization among quartiles 2, 3, and 4, as compared to quartile 1, was significantly higher by $1202, $1650, and $1844, respectively (p-trend<0.001). In conclusion, patients residing in zip codes with lower SES had increased in-hospital mortality and decreased utilization of thrombolysis following acute PE compared to patients residing in higher SES zip codes. The cost of hospitalization for patients from higher SES quartiles was significantly higher than those from lower quartiles.
Introduction
Acute pulmonary embolism (PE) is a leading cause of morbidity and mortality worldwide. It has been estimated that about 300,000 people in the United States die from acute PE, and the diagnosis in a substantial number of cases is not made until autopsy.1,2 A study of hospitalized patients from Olmsted County, Minnesota estimated that the average annual incidence of venous thromboembolism in the United States was as high as one episode per 1000 registered patients. 1 Despite the considerable clinical burden of this disease, epidemiological correlates of this disease remain incompletely understood.
Socioeconomic disparities have been noted in the current healthcare delivery system in the United States for several time-sensitive clinical presentations, including acute coronary syndromes and acute ischemic stroke.3–9 Similar data are, however, lacking for outcomes following acute PE. In the last decade, eliminating disparities in healthcare delivery in the Unites States has been governed largely by the Healthy People 2010 initiative, which has aimed to improve the overall health among all citizens. 10 It can be hypothesized that disparities in outcomes might be mediated by differences in biologic risk factors and comorbidities among patients from different socioeconomic strata. Disparities may also be related to a delay in recognition of symptoms, a delay in presentation to the hospital or differences in the etiology of acute PE. In addition, disparities in the utilization of treatments like thrombolysis for treatment of acute PE might differentially affect outcomes across the various socioeconomic strata.
There is emerging literature to suggest that the place of residence might play an important role in influencing the outcome following acute ischemic stroke and acute myocardial infarction.4,7,11–16 Although these neighborhood effects are poorly understood, they may in part be mediated or moderated by individual socioeconomic, behavioral or biologic risk factors. 7 Other cultural, clinical, economic, geographic and access-related variables may also influence the timeliness of presentation for first medical assessment. While these variables are difficult to individually quantify, SES measured by zip code could serve as a useful surrogate for these intangibles. Several prior studies have validated this approach for imputing individual SES in epidemiologic settings.10,17–20 A residential zip code-based classification of SES may thus reflect the aggregate characteristics of its residents and the prevailing healthy and unhealthy habits. This serves to provide an insight into environmental attributes (like availability and accessibility of healthcare resources) that may have a direct or indirect impact on its residents’ health.
In this analysis, we aimed to determine whether there were differences in outcomes for patients presenting with acute PE based on neighborhood SES. We also aimed to determine whether there were differences in treatment, including administration of thrombolysis and placement of inferior vena cava (IVC) filters, based on neighborhood SES. In addition, we analyzed the differences in in-hospital costs for patients presenting with acute PE, stratified by neighborhood SES. Furthermore, we evaluated the trend in the disparity of in-hospital mortality between the SES strata across the study duration.
Methods
Data source
Data were obtained from the Nationwide Inpatient Sample (NIS) from 2003 to 2011. The NIS is sponsored by the Agency for Healthcare Research and Quality (AHRQ) as a part of the Healthcare Cost and Utilization Projection (HCUP). The NIS contains discharge level data from approximately 8 million hospitalizations annually from about 1000 hospitals across the United States. This database is designed to represent a 20% stratified sample of all hospitals in the country. Location (urban or rural), teaching status, geographic region, patient volume and hospital ownership are the criteria used for stratified sampling of hospitals into the NIS.
Study population
The NIS provides up to 15 diagnoses and 15 procedures for each hospitalization record for the years 2003–2009. The number of diagnoses coded in the database was expanded to 25 for the years 2010–2011. All these have been coded using the standard International Classification of Diseases, 9th edition, Clinical Modification (ICD-9 CM) codes. The first diagnosis in the database is referred to as the ‘principal diagnosis’ and is considered the primary reason for admission to the hospital. All hospitalizations with the principal diagnosis of acute PE were included in our study. These were identified using the ICD-9 CM codes of 415.11 (iatrogenic pulmonary embolus), 415.12 (septic pulmonary embolus), 415.13 (saddle embolus) and 415.19 (other pulmonary embolus). To avoid double counting of hospitalizations, patients who presented as a ‘transfer-in’ from another healthcare facility were excluded from analysis.
We used the HCUP Clinical Classification Software (CCS) to identify patient comorbidities and procedures. 2 CCS has been developed by the AHRQ for clustering patient diagnoses and procedures into a manageable number of clinically meaningful categories. 2 Baseline characteristics available for analysis included age, gender, race, primary source of payment, Elixhauser comorbidities defined by AHRQ, along with other clinically relevant comorbidities such as smoking.1,21 Hospital characteristics such as region (Northeast, Midwest, South, West), bed size (small, medium, large), location (rural, urban), hospital ownership (federal, private) and teaching status were also included.
The primary variable of interest was the SES, assessed using a patient’s residential zip code. The NIS has classified each zip code into quartiles based on the median household income of each zip code. In the year 2011, these quartiles corresponded to: quartile 1: $1–$38,999; quartile 2: $39,000–$47,999; quartile 3: $48,000–$62,999; quartile 4: $63,000 or more. Residential zip code-based classification of SES is known to reflect aggregate characteristics of its residents and an insight into environmental attributes (like available healthcare resources) that may have a direct or indirect impact on its residents’ health. We chose to utilize the residential zip code-based classification to reflect on SES because of its successful validation in prior studies, along with the fact that it reflects aggregate characteristics over individual characteristics, which often govern healthcare delivery.10,17–20
Study outcomes
The primary outcome of our study was in-hospital mortality. The secondary outcomes analyzed included thrombolysis and use of inferior vena cava (IVC) filters. Patients undergoing thrombolysis were identified using ICD-9 CM procedure codes of 99.10 (injection of thrombolytics) or V45.88 (alteplase administration with transfer from another facility). Patients undergoing IVC filter placement were identified using the ICD-9 CM procedure code 38.7. In addition to these outcomes, we also analyzed the differences in cost of hospitalization stratified by residential zip code quartile. The NIS database provides the total charges for hospital stay that were claimed by the respective hospital. The total charges of each hospital stay were converted to cost estimates using the group, average, all-payer, in-hospital cost and charge information from the detailed reports by hospitals to the Centers of Medicare and Medicaid Services (CMS). All costs and charges were converted to projected estimates for the year 2011, after accounting for annual inflation rates based on consumer price index data available from the US Bureau of Labor Statistics. 22
Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD) and categorical variables are presented as proportions. For comparing the means of continuous variables between three or more categories, we utilized one-way analysis of variance (ANOVA). In cases of significant differences detected using ANOVA, pairwise comparisons were performed utilizing Bonferroni correction for multiple comparisons. The chi-squared test was utilized for comparison of categorical variables.
Survey statistics traditionally used to analyze complex semi-random survey designs were employed to analyze these data. Since the data from NIS represent a collection of scattered hospital clusters, analysis was structured to account for a complex, multistage, probability sampling. NIS recommends the use of ‘strata’ for constructing analysis clusters, which include geographic census region, hospital ownership, teaching status, urban/rural location, and bed size. Furthermore, the analysis is stratified into individual hospitals, which serve as primary sampling units for the analysis. In the NIS database, each hospital admission is linked to a ‘discharge weight’ that can be utilized to calculate projected national estimates for all hospital-related outcomes, after accounting for the hierarchical structure of the dataset.
Multivariable hierarchical logistic regression analysis with exchangeable working matrix was utilized to compare outcomes between the zip code quartiles. For this analysis, we utilized the variable ‘nis_straum’ as the strata, variable ‘hospid’ as the primary sampling unit (clustering variable) and the variable ‘discwt’ as the sampling weight. The analysis of all outcomes has been presented after adjusting for age, gender, race, 29 Elixhauser comorbidities, smoking, primary payor, and hospital characteristics. We assessed for the interaction between race and zip code-based SES in all regression models with the study outcomes as dependent variables. The highest SES zip code quartile (quartile 4) has been used as the reference category for all comparisons. Since the variable ‘race’ had ~22% missing data, we utilized multiple imputation for missing data using ordered logistic regression accounting for the clustered nature of the dataset by incorporating hospital characteristics into the multiple imputation model.
All statistical analyses were performed using the statistical software Stata v 13.1 (StataCorp, College Station, TX, USA). All statistical tests were two-tailed; a p-value <0.05 was considered significant. Owing to the de-identified nature of this publicly available administrative database, an institutional review board review was not necessary for the conduct of this study.
Results
Patient characteristics
Over a 9-year period (2003–2011), a total of 276,484 discharges with a principal diagnosis of acute PE were analyzed. Based on the cluster design of the dataset, the estimates derived from the analysis represent outcomes from 1.4 million United States patients admitted with acute PE. Figure 1 demonstrates the annual incidence of acute PE during the last decade, stratified by the SES quartiles. As seen in the figure, there has been a significant increase in the incidence of acute PE. However, despite this improvement, there appears to be a persistent disparity in acute PE incidence between the SES quartiles. Table 1 demonstrates the baseline characteristics of the entire study population, stratified by the SES quartiles. There were clinically small yet statistically significant differences in the mean age and the gender distribution across the SES quartiles. Similarly, there were significant differences in the racial distribution across the SES quartiles. Overall, 60.2% of all patients residing in quartile 1 were white individuals as compared to 84.7% of patients in quartile 4 (p<0.001). In addition, patients in quartile 4 were more likely to have private insurance as the primary payment source as compared to the lower quartiles (44.5% versus 24.7%, p<0.001).
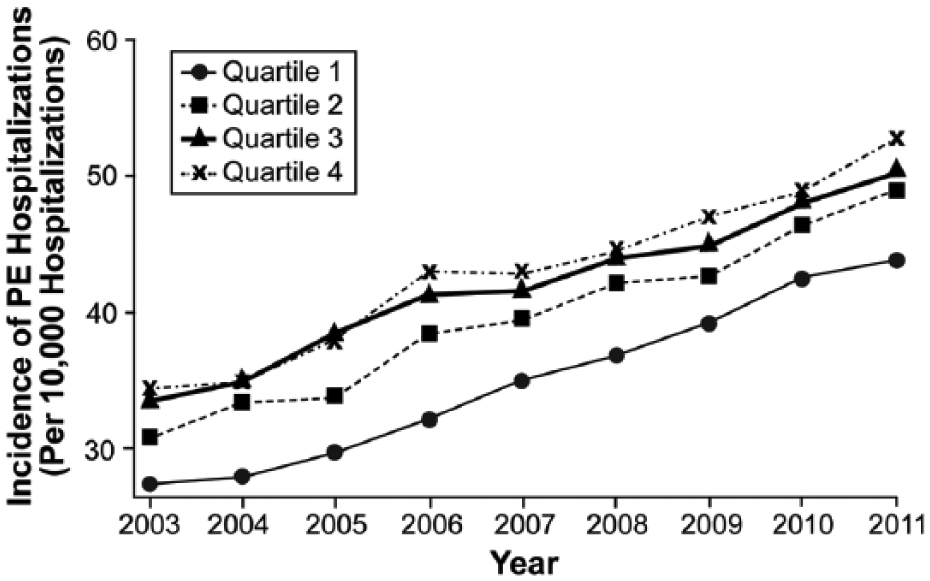
The trend of annual incidence of acute PE (per 10,000 hospitalizations) over the study duration, stratified by income-based socioeconomic quartile.
Baseline characteristics stratified by zip code-based socioeconomic status quartile.
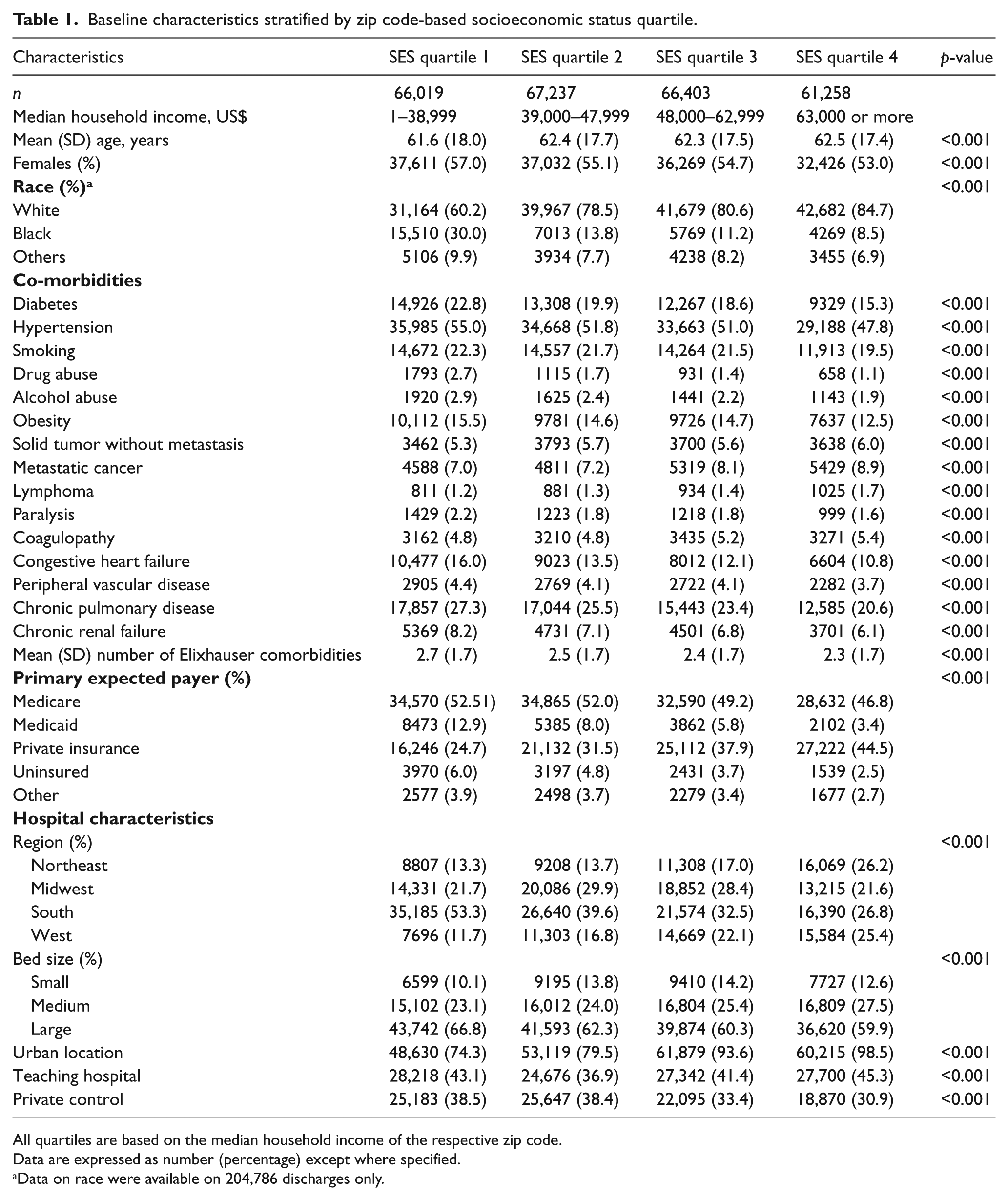
All quartiles are based on the median household income of the respective zip code.
Data are expressed as number (percentage) except where specified.
Data on race were available on 204,786 discharges only.
The differences in the distribution of medical comorbidities between the different SES quartiles are also illustrated in Table 1. There were small but statistically significant decreases in the prevalence of diabetes, hypertension, smoking, obesity, peripheral vascular disease and chronic renal failure across the SES quartiles (p<0.001 for all comparisons). In addition, we noted that there was a significantly higher prevalence of alcohol abuse and drug abuse among residents of lower SES quartiles as compared to higher quartiles (p<0.001 for both comparisons). The prevalence of chronic pulmonary disease was significantly higher in quartile 1 (27.3%) as compared to quartile 4 (20.6%, p<0.001). In addition, there was a progressive increase in the prevalence of solid tumors, metastatic cancers and lymphomas across the SES quartiles (p<0.001 for all comparisons).
Mortality, thrombolysis and IVC filter use
Figure 2 demonstrates the incidence and adjusted odds ratio (OR) for the primary and secondary outcomes across the SES quartiles. There was a highly significant trend indicating progressively lower in-hospital mortality across the SES quartiles (p-trend<0.001). The incidence of in-hospital mortality across quartiles 1–4 was 3.8%, 3.3%, 3.2%, and 3.1%, respectively. In adjusted analysis, there was a significantly higher mortality among patients from quartile 1 as compared to quartile 4 patients [OR (95% CI): 1.23 (1.15–1.32)]. In addition, there was a significant increase in the utilization of thrombolysis across the SES quartiles (1.5%, 1.6%, 1.7%, 2.0%; p-trend <0.001). In adjusted analysis, there was a significantly lower utilization of thrombolysis among patients from quartile 1 as compared to quartile 4 [OR (95% CI): 0.82 (0.73–0.92)]. However, there was no significant difference in the utilization of IVC filters across the SES quartiles on adjusted analysis (p-trend: 0.9). Figure 3 demonstrates the variation in the trend of in-hospital mortality among patients admitted with acute PE over the study duration. Although there has been a considerable reduction in in-hospital mortality over the years in all SES categories, a significant difference in the in-hospital mortality rates has remained between the highest and lowest SES patients admitted with acute PE. Figure 4 demonstrates the variation in the risk-adjusted disparity in in-hospital mortality between quartile 1 and quartile 4, across the study duration. We observed that there was a trend towards a progressively lower disparity in in-hospital mortality between quartile 1 and quartile 4 patients, across the study duration (p-trend<0.001).
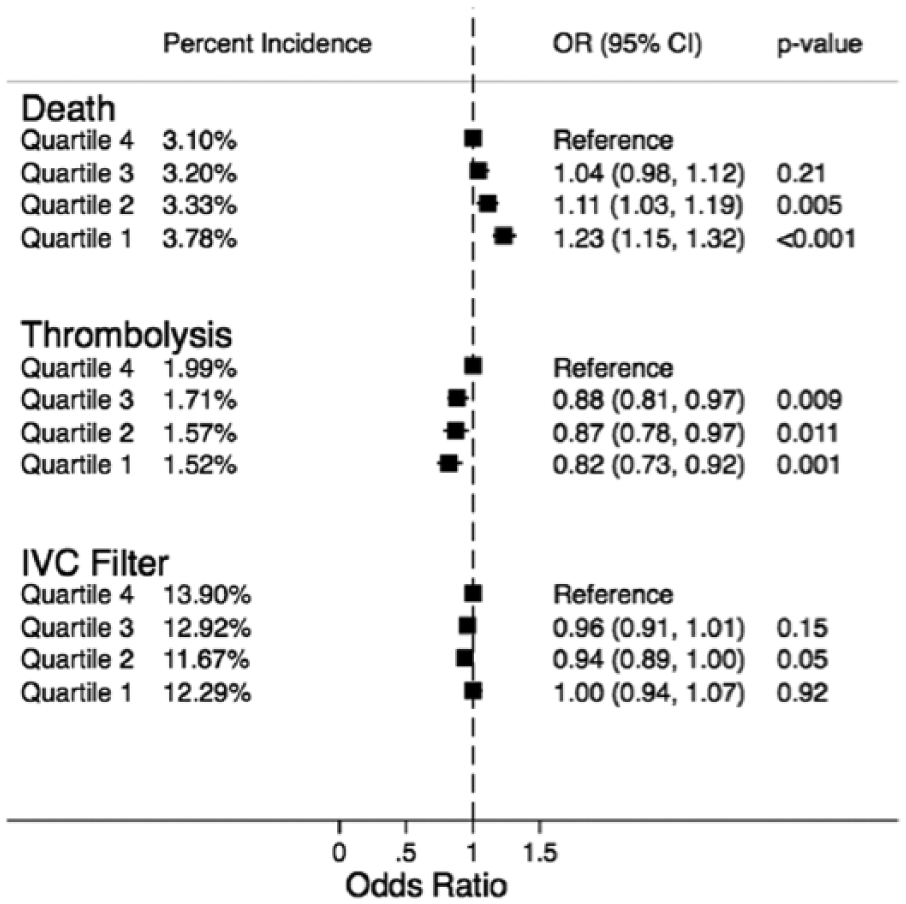
The percent incidence and adjusted odds ratio for in-hospital mortality, thrombolysis and use of inferior vena cava (IVC) filters, stratified by zip code-based socioeconomic quartiles. All quartiles were based on the median household income of the respective zip code. All comparisons were drawn with reference to the highest quartile. (Quartile 1: $1–$38,999, quartile 2: $39,000–$47,999, quartile 3: $48,000–$62,999, quartile 4: $63,000 or more.)
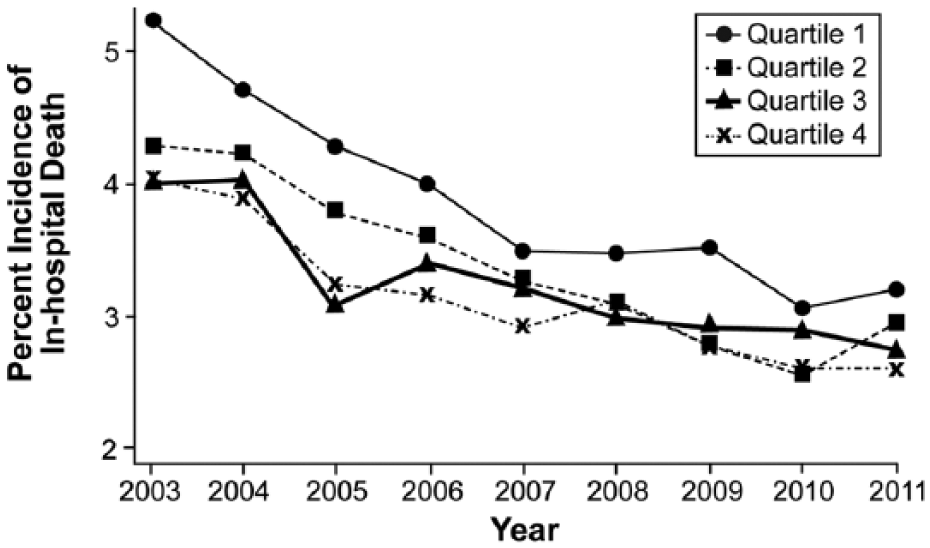
Trend of in-hospital mortality across the four socioeconomic quartiles across the entire study duration (2003–2011). (Quartile 1: $1–$38,999, quartile 2: $39,000–$47,999, quartile 3: $48,000–$62,999, quartile 4: $63,000 or more.)
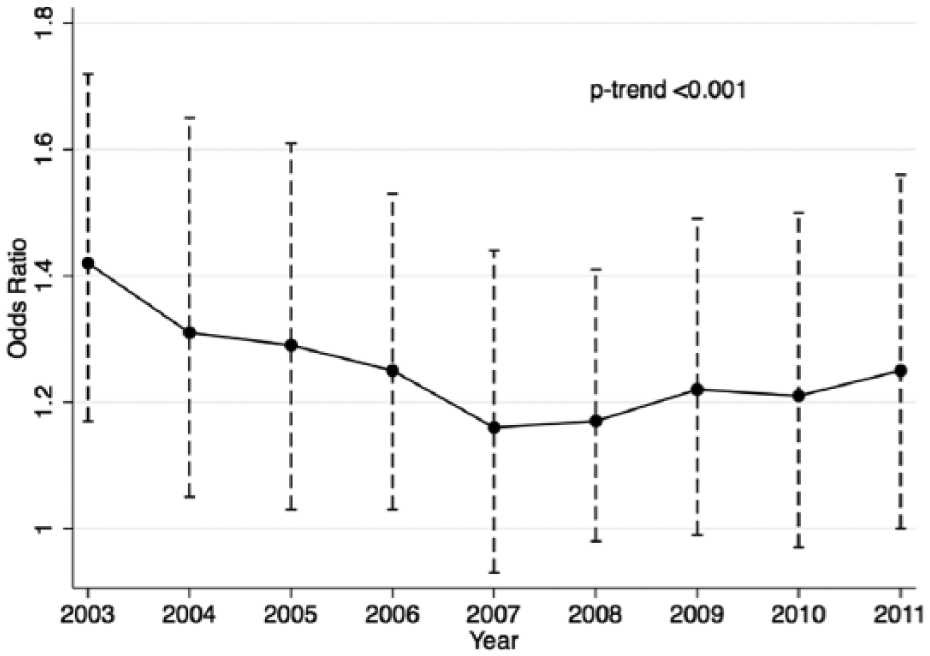
Variation in the risk-adjusted disparity in in-hospital mortality between quartile 4 (highest SES) and quartile 1 (lowest SES), across the study duration. The y-axis represents adjusted odds ratios for in-hospital mortality among quartile 1 patients compared to quartile 4 patients, derived using multivariable logistic regression analysis adjusting for demographic characteristics, clinical comorbidities as well as hospital characteristics.
Cost of hospitalization
The mean (±SD) cost of hospitalization was $12,120 ± $13,036, $11,802 ± $12,912, $12,290 ± $13,183, and $13,330 ± $15,355 among SES quartiles 1–4, respectively. After adjustment for baseline demographic and clinical characteristics, including primary payment source, the adjusted costs of hospitalization for patients from SES quartiles 1, 2, and 3 were significantly lower when compared to the cost of hospitalization for patients from SES quartile 4 (p⩽0.001 for all comparisons). Compared to quartile 1, the mean adjusted costs of hospitalization of quartiles 2, 3, 4 were higher by $1202 (95% CI: $798–$1606), $1650 (95% CI:$1165–$2135), and $1844 (95% CI: $1298–$2391), respectively.
Subgroup analyses
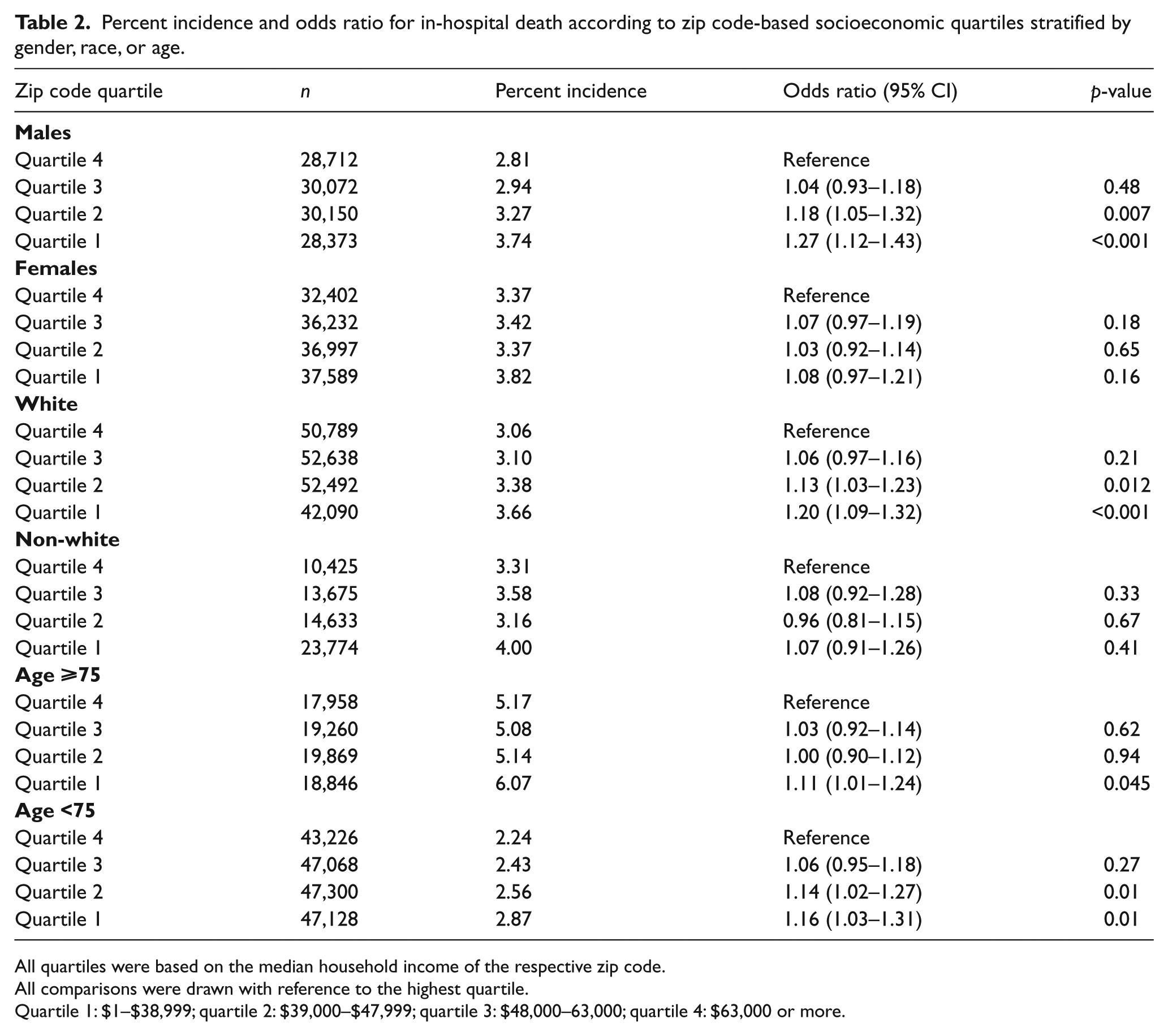
Subgroup analyses demonstrating the differential impact of gender, race, and age on in-hospital death is shown in Table 2. With respect to gender-based strata, the in-hospital mortality among males from the lowest SES quartile was significantly higher than males from the highest SES quartile [OR (95% CI): 1.27 (1.12–1.43)]. Although the overall in-hospital mortality was higher among females as compared to males, there were no differences in in-hospital mortality among females across the SES quartiles. Similarly, the differences in in-hospital mortality across the SES quartiles were more pronounced among the white as compared to non-white population. Furthermore, the incidence of in-hospital mortality was significantly higher among elderly patients (⩾ 75 years) as compared to their younger counterparts in all SES quartiles (p<0.001 for all comparisons). Although in-hospital mortality among the elderly was similar in SES quartiles 2–4, elderly from the lowest SES quartile had a significantly higher odds or in-hospital death [OR (95% CI): 1.11 (1.01–1.24)]. In the younger cohort, there was a significantly higher incidence of in-hospital mortality among patients from the lower SES as compared to those from higher SES quartiles. Overall, the SES mortality association was stronger for the younger cohort as compared to the older cohort (p-interaction: 0.03).
Percent incidence and odds ratio for in-hospital death according to zip code-based socioeconomic quartiles stratified by gender, race, or age.
All quartiles were based on the median household income of the respective zip code.
All comparisons were drawn with reference to the highest quartile.
Quartile 1: $1–$38,999; quartile 2: $39,000–$47,999; quartile 3: $48,000–63,000; quartile 4: $63,000 or more.
Discussion
We have evaluated the impact of the residential zip code-based classification of SES upon in-hospital mortality following acute PE utilizing a large representative nationwide sample in the United States. We observed an increasing disparity in the incidence of acute PE between the socioeconomic quartiles over the last decade. Results from this administrative dataset suggest that the overall in-hospital mortality rate following acute PE has declined over time. Our analysis has demonstrated a significant disparity in both in-hospital outcomes for acute PE patients depending on residential zip code. We also noted a progressive increase in the absolute and adjusted in-hospital mortality after acute PE with a progressive decline in the median household income of a patient’s residential zip code. Furthermore, there was a highly significant trend indicating a progressively reduced thrombolytic utilization among patients from lower SES quartiles, as compared to those from higher quartiles. In addition, the cost of hospitalization for patients from the lower SES quartiles was significantly lower as compared to those from higher SES quartiles.
The differences in neighborhood SES have been consistently associated with variations in morbidity and mortality related to cardiovascular and cerebrovascular disease.7,9,23–25 Individuals residing in neighborhoods with a lower SES have a higher prevalence of comorbidities such as hypertension, diabetes, obesity and smoking, which might account for increased mortality among patients from a lower neighborhood SES. However, the differences in these comorbidities are unlikely to be the sole explanation for differences in clinical outcomes. The differences in several observed clinical outcomes persist between the SES quartiles despite adjustment for baseline comorbidities, suggesting that other factors in healthcare access and delivery likely play a role. In the setting of acute ischemic stroke, lower SES has been demonstrated to limit access to medical care and to bias these patients to present to smaller, low-volume hospitals with lower utilization of evidence-based therapies.6,7,9
To the best of our knowledge, there is scant evidence regarding the impact of neighborhood SES upon outcomes following treatment of acute PE. A study published in 1981 demonstrated an increased incidence of PE among subjects with < 8 years of education compared to subjects with longer education. 26 Rosengren et al. demonstrated an association between SES variables such as persistent stress and low occupational class with the risk of future PE among male subjects. 17 A recently published Swedish study demonstrated that low income; single marital status and a lower level of education were independently associated with an increased risk of venous thromboembolism in a 13-year prospective follow-up of over 18,000 patients. 27
Over the last few decades, we have made remarkable progress in healthcare delivery and outcomes for patients with acute PE. 18 This improvement is likely secondary to improvement in anticoagulation management along with risk-factor management, with possibly higher use of thrombolysis in patients with shock secondary to PE. Our analysis has demonstrated a progressive reduction in in-hospital mortality across the study duration. Although the risk-adjusted disparity in in-hospital mortality has significantly narrowed in recent years, it continues to persist even in modern times. Several socioeconomic and socio-cultural factors including education, access to healthcare resources, income and awareness might play important roles in determining the delay in presentation, potentially impacting the outcome. The impact of surrounding environment becomes highly significant in the context of treating a time-sensitive disease like acute PE. Further, one could argue that the impact of environment, substituted by an aggregate zip code income, might provide a greater degree of insight into society–health dynamics and interactions than individual parameters such as household income.
Many prior studies have demonstrated significant socioeconomic disparities in the utilization of thrombolysis for the treatment of acute ischemic stroke and percutaneous coronary intervention among acute myocardial infarction.4,5,8,28–30 Although the overall rates of thrombolysis in this cohort were low, there was an apparent disparity according to socioeconomic class in this large representative population. It must be recognized that unlike acute myocardial infarction and acute ischemic stroke, acute PE is often misdiagnosed or underdiagnosed in clinical settings. The current study demonstrated a considerable difference in adjusted hospital cost among various SES strata. Whether this represents an underutilization of resources for patients from lower SES zip codes or an overutilization of resources for patients from higher SES zip codes is not completely clear from this analysis. Interestingly, we did not find any significant difference in the use of IVC filters across the SES quartiles. However, utilization of IVC filters in venous thromboembolism is heterogeneous, and many of the indications for insertion of IVC filters revolve around contraindications to anticoagulation.10,31 This possibly suggests that the proportion of patients with contraindications to anticoagulation like bleeding might be similar across the socioeconomic strata.
In addition to assessment of the relationship of neighborhood SES with adverse outcomes after acute PE, our study also provides some additional insight that might form the basis of future analyses. We observed a significant interaction of gender with outcome across the various socioeconomic strata. Whether these gender-based outcome differences reflect true biological differences or are more indicative of differing socioeconomic profiles that render female gender a surrogate for poor outcome is a matter of speculation at this time. Similarly, elderly patients have been traditionally believed to possess a guarded prognosis due to multiple comorbidities, greater delay in seeking medical care, atypical presentations, less physiologic reserve and a higher degree of hemodynamic compromise compared to younger patients. We observed that the neighborhood SES and mortality association appeared to be stronger for the younger than the elderly population. Our experience in acute myocardial infarction has revealed similar findings where the association between neighborhood SES and mortality appeared to be considerably less marked among older patients.4,32,33 Although the mechanisms underlying these associations are unclear, potential hypotheses include improved coping skills among older individuals, perhaps attributable to having lived longer under adverse socioeconomic circumstances along with increased access to healthcare resources owing to public insurance programs like Medicare available to the elderly.
Limitations
Our study has several limitations. First, NIS is an administrative database, which may be subject to errors in coding of diseases or procedures. Second, this is a retrospective observational study, which may be subject to traditional biases of observational studies like selection bias. However, these limitations might be partially alleviated by the large size of the NIS database and a uniform representation of all regions of the United States. Third, we utilized median household income of the entire zip code to ‘impute’ the SES of each patient. The capability of an individual measure like the median household income of the entire zip code to directly relate to the SES of an individual patient may be somewhat limited. However, the inaccuracy that results from the misclassification of individual SES based on the SES of the surrounding neighborhood (so-called ‘ecologic fallacy’) might be completely offset by the lack of occurrence of an ‘individualistic fallacy’, whereby there is an incorrect assumption that the health of an individual subject is not affected by the neighborhood that he/she lives in. 23 In addition, adverse outcomes following acute PE may be affected by numerous variables including disease severity, symptom awareness, and pre-hospital care, which were not always available consistently in the NIS database. Lastly, we have included only those hospitalizations where acute PE was the principal diagnosis for hospitalization. Owing to the heterogeneous nature, the hospitalizations where acute PE was a secondary diagnosis (e.g. post-surgical) were not included, which might lead to some bias in the effect estimates. Furthermore, the in-hospital dataset fails to capture the patients where acute PE was managed on an outpatient basis. Owing to the current treatment practices prevalent in the United States, this number is likely to be a small proportion of all acute PE cases.
Conclusions
There was a higher incidence of in-hospital death among patients residing in low SES zip codes, as compared to those residing in high SES zip codes. Moreover, there was a reduced utilization of thrombolysis among patients from low SES zip codes. In addition, the cost of hospitalization was significantly higher for those who belonged to a high SES zip code as compared to those who belonged to a low SES zip code.
Footnotes
Acknowledgements
The authors would like to acknowledge the help of Ms Kathryn Brock in editing the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.