
Abstract

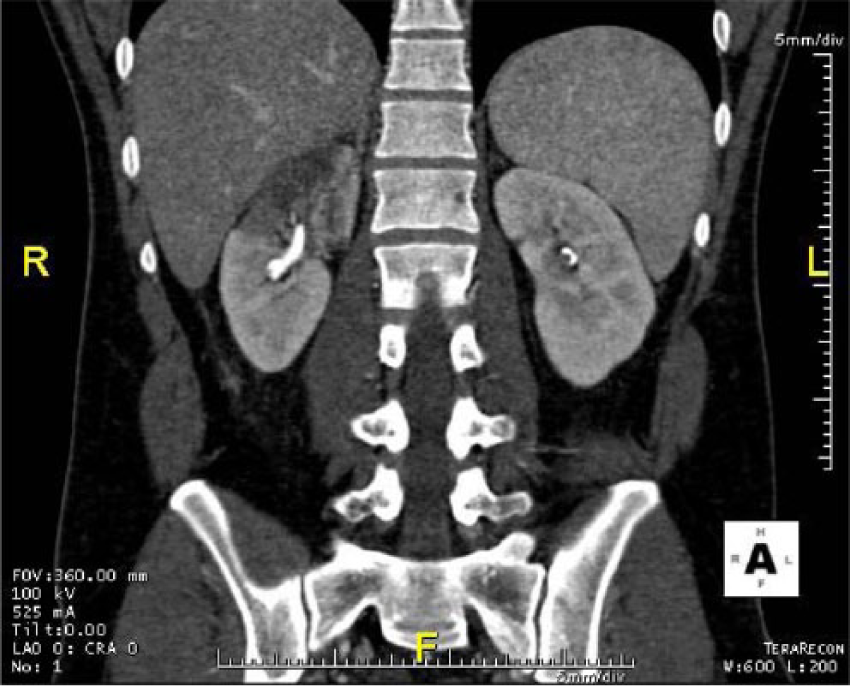
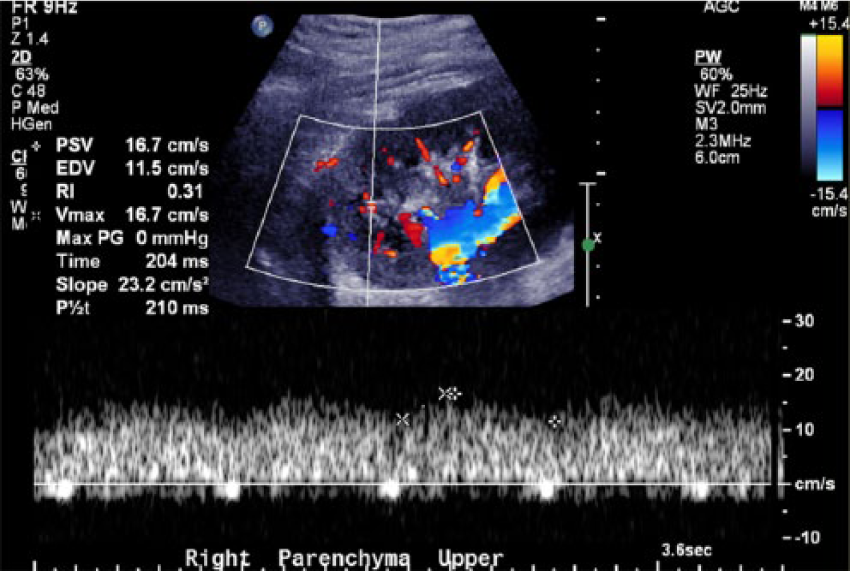
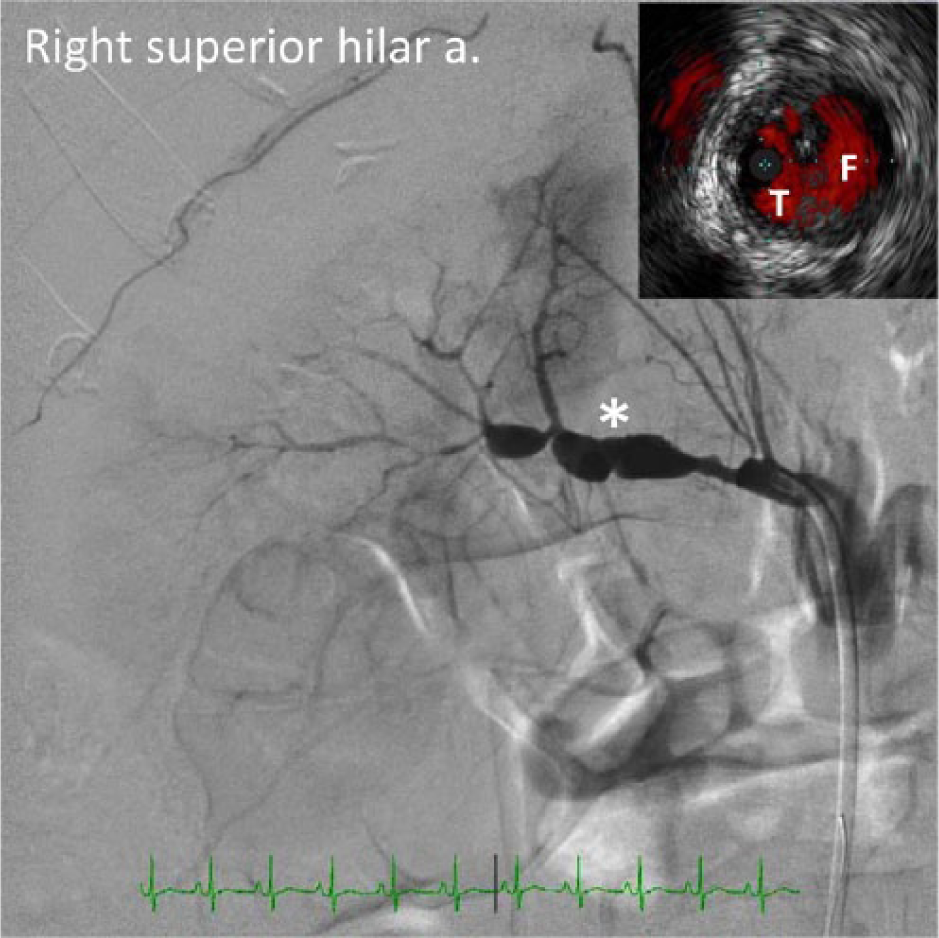
A 32-year-old previously healthy male presented to the emergency department with acute onset of right-sided abdominal and back pain. Review of his social history was positive for heavy daily cannabis use. Unenhanced abdominal computed tomography (CT) showed possible pyelonephritis that prompted treatment with oral antibiotics. After 7 days of persistent hypertension and pain, a follow-up contrast-enhanced abdominal CT revealed areas of infarction in the right kidney (Panel A). Duplex ultrasound confirmed decreased parenchymal flow with a monophasic pattern in the upper pole of the right kidney (Panel B). An abdominal aortogram demonstrated a perfusion defect in the same region (Panel C, dashed outline). Selective angiography of the right superior hilar artery confirmed the presence of a complex dissection extending into the distal segment (Panel D). Endovascular intervention was attempted, but the guidewire could not advance beyond the zone of dissection (asterisk). Intravascular ultrasound (IVUS) (Volcano Corporation; inset) with color imaging (ChromaFlo®) demonstrated a dissection flap with flow in both true (T) and false (F) lumens (entire IVUS recording available as a supplemental video). Extensive serological testing found no evidence of known coagulopathies or vasculitides. Intracranial and extracranial CT angiography showed no dissection, aneurysm or fibromuscular dysplasia (FMD). As the patient’s renal function and blood pressure remained stable, a conservative approach was opted for over surgical revascularization. The patient was treated with systemic anticoagulation, antihypertensives and analgesics and was discharged on hospital day 14.

Spontaneous renal artery dissection (SRAD) is a rare vasculopathy, where patients typically present with sudden abdominal pain and hypertension. SRAD is sometimes associated with connective tissue disorders such as Ehlers-Danlos syndrome and FMD. Unlike the classic form of FMD, however, SRAD has a strong male predominance. 1 Indeed, SRAD may belong to a separate entity called segmental arterial mediolysis (SAM), a non-inflammatory, non-atherosclerotic arteriopathy usually affecting medium-sized visceral arteries. 2 SAM is possibly triggered by chronic and recurrent vasoconstriction, which leads to partial or total vacuolization and lysis of the arterial media, followed by fibrin deposition at the medial–adventitial junction, which weakens the arterial wall and leads to aneurysm, dissection or rupture.
The vasoconstrictor effect of cannabis is well documented, and is associated with stroke, myocardial infarction, and limb arteritis, especially in young patients. Furthermore, cannabis use has been implicated in several recent cases of coronary and renal artery dissections. 3 Given the rising popularity of cannabis use for medicinal and recreational purposes, increased vigilance for and research into its possible cardiovascular complications is warranted.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.